jcoloproctol(rioj).2016;36(2):104–114
w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Review
Article
Analysis
of
the
main
surgical
techniques
for
hemorrhoids
Magno
Otávio
Salgado
de
Freitas
a,∗,
Jaciara
Aparecida
Dias
Santos
b,c,
Maria
Fernanda
Santos
Figueiredo
a,
Cristina
Andrade
Sampaio
aaPost-graduationPrograminPrimaryCareinHealth,SurgicalClinicDepartment,UniversidadeEstadualdeMontesClaros(Unimontes),
MontesClaros,MG,Brazil
bUniversidadeEstadualdeMontesClaros(Unimontes),MontesClaros,MG,Brazil
cProgramofUndergraduateResearch,Fundac¸ãodeAmparoàPesquisadoEstadodeMinasGerais(FAPEMIG),BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received24September2015 Accepted6December2015 Availableonline22March2016
Keywords:
Hemorrhoidectomy Hemorrhoids PPH
a
b
s
t
r
a
c
t
Introduction:Surgicaltreatmentofhemorrhoidaldiseaseisusedinabout5–10%ofcases whereconservativetreatmentshavenotbeeneffective.
Objective:Tolearnthesurgicaltechniquesusedinthetreatmentofhemorrhoidaldisease gradesIIIandIVinthelightofliterature.
Methods:Thisisanexploratorystudy,withanintegrativereviewofliteraturepublishedfrom 2009to2015fromdatabasesLILACS,SciELO,MEDLINE,PUBMEDandthePortalofCAPES, usingthefollowingdescriptors:“hemorrhoidectomy”and“hemorrhoids”,intheperiodfrom MarchtoMay2015.
Results:Nineteenarticleswereselected.Inthefourmoredescribedtechniques,thesurgical timerangedfrom19.58to52min,withrelapsesfrom5%,from17.5to35minandrecurrences of7.5%to8.2%,23–35minwas20%and22.5%relapse,12.5and13.2min,3.5%ofrelapses.
Conclusion:Conventionaltechniquesarestillthemostcommonlyperformedwithagood acceptanceonthelong-termresolutionandlowrecurrencerate.
©2016SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense
(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Análise
das
principais
técnicas
cirúrgicas
para
doenc¸a
hemorroidária
Palavras-chave:
Hemorroidectomia Hemorroidas PPH
r
e
s
u
m
o
Introduc¸ão:Otratamentocirúrgicodadoenc¸ahemorroidáriaéutilizadoparacercade5a 10%doscasosemqueostratamentosconservadoresnãosurtiramefeito.
Objetivo:Conhecerastécnicascirúrgicasutilizadasnotratamentodadoenc¸ahemorroidária grauIIIeIVàluzdaliteratura.
∗ Correspondingauthor.
E-mail:[email protected](M.O.S.deFreitas).
http://dx.doi.org/10.1016/j.jcol.2015.12.008
jcoloproctol(rioj).2016;36(2):104–114
105
Métodos:Trata-sedeumestudoexploratório,comrevisãointegrativadaliteraturapublicada nosanosde2009a2015,dasbasesdedadosLILACS,SciELO,MEDLINE,PUBMEDenoPortal daCAPES;apartirdosseguintesdescritores:hemorroidectomiaehemorroidas,noperíodo demarc¸oamaiode2015.
Resultados: Foramselecionados19artigos.Nasquatrotécnicasmaisdescritas,otempo cirúrgicovarioude19,58a52minutoserecidivasde5%,de17,5a35minutoseasrecidivas de7,5%a8,2%,de23a35minutosehouvede20%a22,5%derecidivas,de12,5e13,2 minutose3,5%derecidivas.
Conclusão: Astécnicasconvencionaisaindasãoasmaisrealizadas,comboaaceitac¸ão quantoàresoluc¸ãoalongoprazoecombaixoíndicederecidivas.
©2016SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este éumartigoOpenAccesssobalicençadeCCBY-NC-ND
(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Hemorrhoidaldisease(HD)isaconditionthatafflictsabout 4.4%ofworldpopulation,andisthemostcommonanal dis-order.Theagedistributionshowsahigherincidenceamong patientsaged45–65yearswithdecreasedinvolvementafter 65years,andthefactthatmenaremorefrequentlyaffected thanwomen.1,2 Theprobablecauseoftheonset of hemor-rhoids,accordingtothetheoryofThompson,1975,wouldbe theprolapsedanalvascularcushions,whichareconstituted bymusclefibers–atissueoffibroelasticconsistenceand vas-cularplexuseswitharteriovenousanastomoses.3
TheHDmaybeinternalorexternal,dependingonits rela-tionshiptothedentateline.HDisfurtherclassifiedintogrades rangingfromonetofour,withthreeandfourdegreesthemost seriousones.Thepossibleetiologiesofthedisease include prolongedeffort,pregnancy,constipation,heredity,increased intra-abdominal pressure with obstruction of the venous return,andprobablyaging.Thus,patientswithhemorrhoids may reportabright redbleeding throughthe rectum, anal pain,protrudingmasses,itching,burninganddiscomfort.4
Currently, there are several therapeutic possibilities for the treatment of hemorrhoids, with the options ranging fromchangesineatinghabits,medicationsthatalleviatethe symptoms,theuseofoutpatienttechniquessuchas cryother-apy,sclerotherapy,laser photocoagulationand rubberband ligation,tosurgicalexcisiontechniquesforhemorrhoidal pro-lapsesaffectedbythedisease.5,6
Thesurgical treatmentis usedin about 5–10%of cases inwhichtheconservativetreatmenthadnoeffect;patients withsymptomaticoracuteGradeIIIorIVhemorrhoidswho havenotimprovedwithothertreatmentsareelectedforthe procedure.3
Surgicaltechniquesareoftendescribedasfivebasictypes: open and closed techniques, proposed byMilligan–Morgan andFerguson,respectively,andthesemi-closed,amputative, and stapled hemorrhoidopexy (PPH).5 Withregard torates ofcomplications,hemorrhoidectomypresentsratesranging from3%to12%,and themostcommon complicationsare: urinaryretention,localpain,bleeding,analstenosis,perianal fistula,analincontinence,andrecurrence.7
Inlightofthis,consideration mustbegiventothemain surgicaltechniquesusedinthe treatmentofgradesIIIand
IVhemorrhoidaldisease,aswellasaspectsinherenttoeach techniquethatwouldinterfereinthebestprognosisforthe patient – postoperativepain, recurrence, surgical time and returntonormalactivity.However,littlehasbeendiscussed intheliteratureabouttheseissues,andevenlessinBrazilian literature.Thus,thisstudyaimstoevaluatethesurgical tech-niquesusedinthetreatmentofgradesIIIandIVhemorrhoidal disease,accordingtothepertinentliterature.
Method
Thisisanexploratorystudythatoutlined,fromanintegrative reviewofscientific literatureoncurrent surgical, the tech-niquesusedinthetreatmentofgradesIIIandIVhemorrhoidal disease.Thechoiceofthismethodwasduetothepossibility ofgrouping,evaluateandsynthesizetheresultsofresearchon aparticularsubjectinanorganizedandsystematicmanner, usingitwiththeobjectiveofobtainingamorecomprehensive understandingofthestudiesontheproposedtheme,besides workingasa synthesistoolforpublished andscientifically establishedstudies.8
In this research, publications available from 2009 to 2015 inthe databases LILACS (Literatura Latino-Americana edoCaribeem Ciênciasda Saúde), SciELO(Scientific Elec-tronicLibraryOnline),MEDLINE(MedicalLiteratureAnalysis and Retrieval System Online), PUBMED and CAPES Portal were surveyed. The search took place from March toMay 2015. Thedescriptors usedwere “hemorroidectomia [hem-orrhoidectomy]”, “hemorroidas [hemorrhoids]” and “PPH”. These descriptorswere chosenbecausetheyallowtocover andthereforeenabletheachievementofadiversifiedresult withrespecttosurgicaltechniques.
The titles and abstracts ofarticles were scrutinizedfor identificationofthosestudieswhichlookedattheproposed objective,consideringthefollowinginclusion criteria: stud-iespublishedinnationalandinternationaljournalswritten inEnglish,SpanishandPortuguese,andaccessedwithafree andfulltext.Reviewarticles,theses,editorials,letterstothe editorandstudieswherethemainfocuswasnottheanalysis ofsurgicaltechniquesusedingradesIIIandIVhemorrhoidal diseasewereexcluded.
106
jcoloproctol(rioj).2016;36(2):104–114articleswasproduced,andthechosenvariableswere:name ofthestudy,authorship/year,journal,studyobjective,study design and conclusions/recommendations. These variables were arrangedinthe collectioninstrument inthe order in whichtheywerefoundandselectedduringthesearch.
Results
and
discussion
Fromthedefinedstrategy,theliteraturesearchresultedin202 articles,ofwhich70werefoundinMEDLINE,63inPUBMED, 17inLILACS,38intheCAPESportal,and14inSciELO.After reading thetitles and abstractsofthesearticles, 47 poten-tiallyrelevantstudieswerefoundandthencarefullyreadin theirentirety.Ofthesearticles,19wereselected,becausethey strictlyfollowedtheinclusioncriteria.
Theanalysisofthe selectedmaterialwasperformed by meansofacriticalandqualitativereadingwhichallowedthe identificationofconvergences,enablingthefollowing group-ingbythematicaxes:conventionaltechniques(Fergusonand Milligan–Morgan),PPH(procedureforprolapsedhemorrhoid), THD(transanalhemorrhoiddearterialization)andLigaSureTM; theseaxeswere alsodefined accordingto themainissues presentinthediscussionsandwiththestudyoutcomes: surgi-caltime,recurrence,postoperativepainandreturntoactivity. Aftertheinterpretationoftheresults,aknowledgesynthesis wascarriedout.
TheresultsarelistedinTable1,inwhichthetitleofthe study,authorship,journal,studyobjective,studydesignand conclusions/recommendationsareidentified.
Intheanalysisoftheselectedarticles,wefoundfour stud-iesthatcomparedconventional(openandclosed)techniques
versusPPHtechnique;fourstudiesthatevaluatedPPH tech-nique;twopublicationsthatanalyzedPPHversusTHD;four articles that addressed only conventional techniques; four studies that also analyzed conventional techniques versus
LigaSureTM; andonestudy thatsinglyexaminedTHD tech-nique. The number and percentage of productsrelated to theyearofpublicationwerealsoconsideredinthisstudy,as describedinTable2.
Itwasobservedthattheperiodwiththehighestnumber ofpublicationswastheyear2013:6(31.5%)articles.Theyears 2011,2014and2015producedonearticleeach(5.3%).Thus,itis clearthattherewasadecreaseinthenumberofpublications inthelast year,showingadecreased concernwithrespect totheissueathand.Regardingthecountryoforiginofthe publications,itwasclear(Table3)thatBrazilandChilehad thehighestnumberofpublications:3(15.7%)each.
Itwas foundthatthe fourmostwidelyusedtechniques were:conventional,PPH,THDandLigaSureTM.
Conventionalsurgicaltechniques
Themostcommonlyusedconventionaltechniqueswerethe open(Milligan–Morgan)andtheclosed(Ferguson)technique. Theopentechniqueisconsideredthegoldstandardforthe surgicaltreatmentofgradeIVhemorrhoidaldisease.Initially, thistechniquewasproposedbySalmonin1830and popular-izedsince1937byMilliganandMorgan;basicallyitconsists oftheexcisionofthehemorrhoidaltissuewithligationand
dissectionofthevascularpedicle,leavingthewoundopento healbysecondaryintention.6
Ontheotherhand,theclosedtechniqueisconsideredas aclassicalprocedure;itwasdescribedintheliteratureby Fer-gusonin1931andpublishedin1959byJamesFergusonand RichardHeaton.Thistechniqueischaracterizedbythe exci-sionofthehaemorrhoidaltissue,followedbytheligationof the vascular pedicle, but withsutures appliedtodissected andresectedareas.Thesurgicalprocedureincludesareduced surgicaltime,besidesprovidingthepatientwithlessscar for-mationandpreservationofanalsensitivity.6
Surgicaltimeandreturntonormalactivity
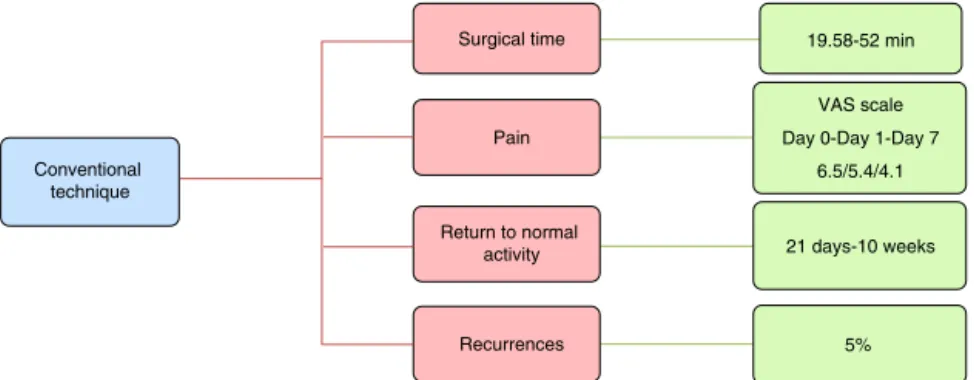
AccordingtodatadescribedinFig.1,thesurgicaltimeofthe conventional techniquerangedfrom 19.58to52min.Thus, the comparativestudybetweenLigaSureTM versusFerguson techniques,carriedoutinthesurgerysectoroftheRegional HospitalofRancagua,inChile,9showedthattheclosed tech-nique showed a surgical time of 24.3±7min. In contrast, thecomparisonbetweenthesesametechniquesdescribedby theDepartmentofSurgery,BanarasHinduUniversity,India, showedasurgicaltimeforFerguson’stechniqueof29min.10
Ontheotherhand,thecomparativestudybetween hem-orrhoidectomytechniquebylaserversusconventional open techniquethatwasheldinAlokaHospital,Kosovo,showed a surgical time of 26.74min.2 The investigation developed inChinawiththeopentechnique(Milligan–Morgan)gotthe shortersurgicaltime,whichwas19.58±2.71min.11Thelonger surgicaltimehasbeenreportedinaBrazilianstudythat com-paredtheconventionaltechniqueandPPHinahospitalinSão Paulo,withtheconventionaltechnique,ittookapproximately 52minandlasted PPH 31minwithstatistical significance.7 Alongsurgicaltimecanexposethepatienttoahigherrisk ofinfectionasthepatientloseshis/herfirstprotective bar-rier(skin)againstmicroorganisms,withperianalandperineal sepsisasapotentialcomplication.12
With respecttothe return toactivity,patients returned afterperiodsfrom21daysto10weeks.InthestudyofKhanna etal.,10thisperiodwasof21days.Intheircomparativestudy between theclosed and semi-closed techniquesperformed intheOutpatientSurgeryDepartmentoftheHospitalBarros LucoTrudeauinChile,Azolasetal.13pointoutthatthereturn wasinabout30days.Inhispublication,Roldós14describes thatthereturntonormallifeforhispatientsoccurredwithin an interval of29 days. Marianelliet al.7 described intheir studythatthereturntonormalactivityoccurredin10weeks. A meta-analysisthat examined theresultsofcomparisons ofconventional hemorrhoidectomy versusLigaSureTM in10 articles,showedthattheuseofLigaSureTM wasstatistically superior in many ways, including less operating time and postoperativepain,fasterreturntoactivityandlowerrateof complications.1
Painandrecurrences
j
coloproctol
(rio
j).
2
0
1
6;
3
6(2)
:104–114
107
Table1–Distributionofthestudiesselected,accordingtothestudyname,authorship,journal,studyobjective,studydesignandconclusions/recommendations, 2009–2015.
Studyname Authorship Journal Studyobjective Studydesign Conclusions/recommendations Evaluaciónfuncionaly
encuestade satisfaccióndelos pacientesoperadosde hemorroidescon técnicadePPH
Heine,Cápona,López, Larach,Larach,Kronberg, etal.(2010)
RevistaChilenadeCirugía Knowingtheevolutionand perceptionofpatients operatedforhemorrhoids withthePPHtechniquein themediumterm.
Investigativestudy Mostpatientsfavorablyassessed thehemorrhoidectomytreatedby PPHintermsofresolutionof postoperativesymptoms, functionalstatus,andoverall satisfactioninthemediumterm. Surgicalcomplications
in2840casesof hemorrhoidectomyby Milligan–Morgan, Fergusonand combinedtechniques
Santos,Coutinho,Meyer, SampaioandCruz(2012)
JournalofColoproctology Reviewandupdate87cases ofsurgicalcomplications fromaseriesof2840 patientsundergoing hemorrhoidectomyusing Milligan–Morgan,Ferguson andmixedtechniquesover theperiodof46yearsof professionalactivityinthis specialty(1965–2011).
Originalarticle Theacceptanceofthesurgical indicationforhemorrhoidectomy was25.7%,beingmorecommon andbetteracceptedbywomen thanbymen.Thisoperationwas performedmoreofteninpatients inthefourth,fifthandthird decadesoflifeandtheoverall incidenceofsurgical
complicationswas3.0%.Themost commoncomplicationswereanal stenosisandseverebleeding,with nodifferencebetweensurgical techniques.
Hemorroidectomia convencionalversus
Hemorroidopexia Mecânica(PPH). Estudoretrospectivo de253casos
Marianelli,Machado, Almeida,Baraviera, Falleiros,Lolli,etal.(2009)
RevistaBrasileirade Coloproctologia
Reviewtheexperienceof thecoloproctologyservice, HSPM-SP,insurgical treatmentofhemorrhoidal disease.
Documentarystudy Themostwidelyusedmethodfor thesurgicaltreatmentof hemorrhoidswasconventional hemorrhoidectomy.Itwasalso observedthatmechanical hemorrhoidopexy(PPH)showed shorteroperativetimeandfaster postoperativerecovery.Moreover, therewasagreatertendencyto latecomplicationsand recurrences,withthepatientsin needofanewsurgeryinthe conventionalhemorrhoidectomy group.
Hemorroidectomía cerraday
semicerrada:Estudio prospectivo aleatorizado
Azolas,Villalón,Danilla, Hasbún,Gaticaand Salamanca(2010)
RevistaChilenadeCirugía Comparetheresultsof closedversusthe half-closedsemicerrada hemorrhoidectomyin termsofpain, complications,surgical timeandhealing.
108
j
coloproctol
(rio
j).
2
0
1
6;
3
6(2)
:104–114
Table1–(Continued)
Studyname Authorship Journal Studyobjective Studydesign Conclusions/recommendations Estudiocomparativo
entre
hemorroidectomía cerradadeFergusony hemorroidectomía comLigaSureTM
Jaramillo,Beltrán,Bozzo, andLarracheaeGonzález (2011)
RevistaColombianade Cirurgia
Compareconventional hemorrhoidectomy, representedbyFerguson techniqueversus
hemorrhoidectomywith LigaSureTM.
Originalarticle Thehemorrhoidectomywith LigaSureTMsignificantlyshortens
thesurgicaltime,being comparableintermsof postoperativepainandof complicationswithFerguson hemorrhoidectomy. Nuevatécnica
quirúrgicaparael tratamientodela enfermedad hemorroidal
Roldós(2010) RevistaCubanadeCirurgia Reducethemorbidityof surgicaltreatmentofthe disease.
Originalarticle Theproposedtechniqueprovides anewoptiontoimprove
postoperativemorbidityofsurgical treatmentinpatientswith hemorrhoidaldisease.New randomizedcontrolledtrialson hemorrhoidectomytechniquesare needed.
AnálisisyResultadosde laOperaciónde Fergusonemel Tratamientodela Enfermedad Hemorroidal
Ferrari,Jamier,Barrionuevo andAndrada(2013)
RevistaArgentinade Coloproctologia
Prospectivelyevaluatethe resultsobtainedfroma seriesof
hemorrhoidectomy proceduresperformedwith Fergusontechnique.
Originalarticle Thehemorrhoidectomywiththe Fergusontechniqueresultedinan appropriateandeffective procedureforthetreatmentof gradeIIorIIIhemorrhoidal disease,withalowrateof postoperativecomplications. Procedimientopara
hemorroidescon prolapsodemucosa: TécnicadeLongo. Reportepreliminar.
Mederos,Pintoand Manzaneda(2009)
RevistaMedicaHerediana Evaluatetheefficacyand safetyofPPHinpatients withgradesIIIandIV hemorrhoidswithrectal mucosaprolapse.
Originalarticle HemorrhoidectomybyPPHis effectiveintreatingsymptomsof gradeIIIandIVhemorrhoidswith prolapseofthemucosa,atleastin theshortandmediumterm. Hemorroidectomíacom
LigaSureTMvs.
diatermia
convencional:Análisis retrospectivo monocéntrico
Papis,Parodi,Herrerías, Sánchez,Gómez,Sierra, etal.(2013)
ActaGastroenterologica Latinoamericana
Comparethesurgical outcomesbetweenthe hemorrhoidectomy performedaccordingto Milligan–Morgantechnique withuseofLigaSureTMand
thatperformedwith conventionaldiathermy.
Originalarticle Thehemorrhoidectomyperformed withLigaSureTMprovedtobea
safetechnique,withalowrateof postoperativepainandfewer complications.
Milligan–Morgan hemorrhoidectomy withanalcushion suspensionand partialinternal sphincterresection forcircumferential mixedhemorrhoids
Lu,Shi,Wang,Wu,Liuand Wen(2013)
WorldJournalof Gastroenterology
Identifyamoreeffective treatmentprotocolfor mixedcircumferential hemorrhoids.
j
coloproctol
(rio
j).
2
0
1
6;
3
6(2)
:104–114
109
Table1–(Continued)
Studyname Authorship Journal Studyobjective Studydesign Conclusions/recommendations Clinicalobservationson
thetreatmentof prolapsing hemorrhoidswith tissueselecting therapy
Wang,Zhang,Zeng,Zhang, Zhu,Liu,etal.(2015)
WorldJournalof Gastroenterology
Comparetheeffectsand postoperative
complicationsbetweenthe tissuefromstapled therapeuticsand Milligan–Morgan hemorrhoidectomy.
Originalarticle Therapywiththeuseofastapler forsevereprolapsedhemorrhoidis asatisfactorytechniquefor obtainingfasterrecovery,lower complicationratesandhigher operatingsafety.
Laser
Hemorrhoidoplasty Procedurevs.Open Surgical
Hemorrhoidectomy:a TrialComparing2 Treatmentsfor HemorrhoidsofThird andFourthDegree
Maloku,Gashi,Lazovic, IslamiandJuniku-Shkololli (2014)
ActaInformaticaMedica Comparethelaser procedureforsymptomatic hemorrhoidswithanopen surgicalprocedurein outpatientcare
Originalarticle Thelaserprocedurefor hemorrhoidswasmoreeffective thanopensurgical
hemorrhoidectomy.Postoperative painandsurgicaltimeareonly twoindicatorsforthisdifference.
Comparisonof LigaSureTM
Hemorrhoidectomy withConventional Ferguson’s Hemorrhoidectomy
Khanna,Khanna,Bhadani, SinghandKhanna(2010)
IndianJournalofSurgery CompareLigaSureTM
hemorrhoidectomyversus
conventionalFerguson’s ‘closed’hemorrhoidectomy forthetreatmentofgrade IIIandIVhemorrhoids.
Originalarticle TheLigaSureTM
hemorrhoidectomyisasafeand effectiveprocedure,withless bloodloss,postoperativepain,and complicationscomparedwith conventionalhemorrhoidectomy. Technically,itismuchsimpler,by obviatingtheuseofsuturesand hemostasis.
Milligan–Morgan Hemorrhoidectomyvs
Stapled
Hemorrhoidopexy.
Kashani,Mehrvarz,Nzeini andErfanian(2012)
TraumaMonthly Evaluateandcomparethe resultsofthesetwosurgical proceduresintermsof recovery,improvementof symptomsandincidenceof complications
Originalarticle Bothtechniquesareeffective methodsforthetreatmentof gradeIIIandIVhemorrhoidsand areassociatedwitharecoveryrate over95%.Overall,theresultsare thesameforbothtechniques.Low postoperativepainwastheonly advantageofstaplingtechnique
110
j
coloproctol
(rio
j).
2
0
1
6;
3
6(2)
:104–114
Table1–(Continued)
Studyname Authorship Journal Studyobjective Studydesign Conclusions/recommendations Comoo
Coloproctologista BrasileiroVêaDoenc¸a Hemorroidária–Análise deDadosColhidosde QuestionárioDirigido aosEspecialistas FiliadosàSociedade Brasileirade Coloproctologia
Cruz,Alvarenga, Constantino,Andrade, Gomes,Faria,etal.(2009)
RevistaBrasileirade Coloproctologia
Analyzetheresponsesto anextensivequestionnaire with52questionsabout hemorrhoidaldisease(HD)
Originalarticle Themainsurgicalindicationfor hemorrhoidaldiseasewasthe intensityofsymptoms(64.47%), withapreferenceforthe Milligan–Morganopentechnique (65.79%).
Transanal haemorrhoidal dearterialisationwith mucopexyversus
stapler
haemorrhoidopexy:a randomizedtrialwith long-termfollow-up
Lucarelli,Picchio, Caporossi,DeAngelis,Di Filippo,etal.(2013)
AnnalsoftheRoyalCollege ofSurgeonsofEngland
Comparethelong-term resultsoftransanal hemorrhoidal dearterialization(THD)
versusmucopexyand stapledhaemorrhoidopexy (SH)inthetreatmentof gradeIIIandIV hemorrhoids.
Originalarticle TherecurrencerateafterTHDwith mucopexyissignificantlyhigher thanafterlong-termSH,although theresultsweresimilarwith respecttothecontrolofsymptoms andpatientsatisfaction.
Resultadosauma ˜no trasdesarterialización hemorroidalguiada pordoppler
Gomez-Rosado, Sanchez-Ramirez, Capitan-Morales, Valdes-Hernandez, Reyes-Diaz,Cintas-Catena, etal.(2012)
CirugiaEspa ˜nola Evaluatethesafetyand efficacyofthistechnique (Doppler-guided hemorrhoidal dearterialization)after 1-yearfollow-up.
Originalarticle Doppler-guidedhemorrhoidal dearterializationappearstobe effectiveafteroneyear,withalow complicationrate.
Stapled
hemorrhoidectomy; resultsofa prospectiveclinical trialinSaudiArabia
GurayaandKhairy(2013) JournalofClinicaland DiagnosticResearch
Evaluatetheeffectiveness ofstapled
hemorrhoidectomy(SH)in termsofcureofsymptoms andcontrolof
postoperativepain.
Originalarticle SHisasafe,fastandconvenient surgicaloptiongradeIIIandIV hemorrhoids,withalow complicationrate,minimal postoperativepain,andearly dischargefromhospital. Stapled
hemorrhoidopexye Initialexperience fromageneral surgerycenter
Jaiswal,GuptaandDavera (2013)
MedicalJournalofArmed ForcesofIndia
Knowingtheinitial experienceofahospital service,regardingstapling technique.
jcoloproctol(rioj).2016;36(2):104–114
111
Conventional technique
Surgical time 19.58-52 min
Pain
VAS scale
Day 0-Day 1-Day 7
6.5/5.4/4.1
Return to normal
activity 21 days-10 weeks
Recurrences 5%
Fig.1–Distributionofstudiesaccordingtosurgicaltime,pain,returntoactivityandrecurrencesintheconventional
technique,2009–2015.
pain,itrangesfrom0to10(where0isrelatedtoatotalabsence ofpainand10beingthemaximumlevelofbearablepain).15
Onaverage,painondayzeroreceivedagrade=6.5 (mod-erate);onday1,5.4(moderate);andonday7,4.1(light),with 5%ofrecurrences.Jaramilloetal.9observedintheirstudythat painonday0receivedagrade=6.1;onday1,4.8;andonday7, 6.3.Therewerenorecurrences.Intheirstudy,Khannaetal.10 foundthatthepaininVASscaleatday0=8.6;onday1=6.4; andonday7=1.6,with5%ofrecurrences.Therecurrencerate wasconfirmedbythestudybyKashanietal.16;thesefindings comparedPPHversusMilligan–Morgantechniqueinahospital inIran;however,thepaingradewas=4.6ondayzeroand=2.3
Table2–Distributionofthesampleaccordingtothe yearofpublication,2009–2015.
Year n %
2009 3 15.8
2010 4 21
2011 1 5.3
2012 3 15.8
2013 6 31.5
2014 1 5.3
2015 1 5.3
Total 19 100
Table3–Distributionofthesampleaccordingthe countryoforiginofthestudies,2009–2015.
Year n %
SaudiArabia 1 5.3
Argentina 1 5.3
Brazil 3 15.7
Chile 3 15.7
China 2 10.52
Cuba 1 5.3
Spain 2 10.5
India 2 10.5
Iran 1 5.3
Italy 1 5.3
Kosovo 1 5.3
Peru 1 5.3
Total 19 100
onday7.Luetal.11onlyratedthepainasmild,moderateor severe,andtherateofrecurrencewasnotevaluated.
Animportantpointinrelationtoconventionaltechnique isalowerrecurrenceratethat,asdescribedintheliterature, rangesfrom3.1to31%.7Inthisstudy,therecurrenceratewas alsolowerincomparisonwithTHDtechniquesandPPH,which suggestsbetterefficiency/effectivenessofthetechnique,from Ceratoetal.3pointofview,whocorroboratethesefindings, emphasizingthatthecurrentmeta-analyzesandcohort stud-iescomparingPPHversusconventionalsurgeryshowedhigher recurrenceinpatientswhoweretreatedwithPPH.
Relapsescausetheoccurrenceofmultipledisorders,since thepatientwillhavetoundergoanewsurgicalprocedure. Evi-denceoflesserpainaftersurgeryandfasterrecoverytimes forpatientssubmittedtoPPHwasalsoobserved,whenthis techniquewascomparedwiththeconventionaltechnique.3
Studies suggest that in comparison with the conven-tionaltechnique,theuseofLigaSureTMtechniquemaybenefit patientsintermsoflesspostoperativepainandfewer compli-cations,sincetheintenseandprolongedpostoperativepain, caused by removal of hemorrhoids always constitutes an importantconcernforbothsurgeonsandforpatients.17
Procedureforprolapsedhemorrhoid(PPH)
ThistechniquewasdescribedbyLongoin1993asanew sur-gicaloptionforthetreatmentofhemorrhoidaldisease;with PPH,anannulusofmucosaandsubmucosaisremovedwith theuseofacircularstaplerabovethedentateline,with fixa-tionthehemorrhoidalpadforcorrectionoftheprolapse.18
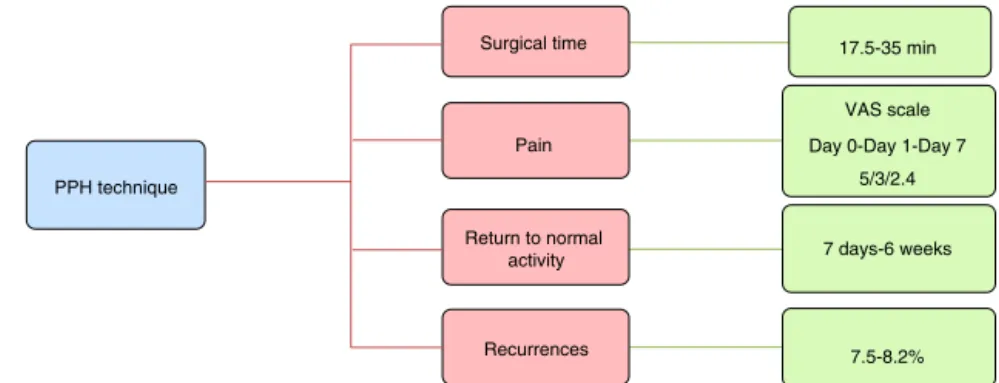
PPHshowedasurgicaltimevariationof17.5–35min.Not allstudiesassessedpainbyVASscale;insomearticlespain wasdescribedasmildortolerable;theaverageinthosestudies thatusedtheVASscalewas:ondayzero,grade5(moderate); onday1,grade3(mild);andonday7,grade2.4(light).The returntonormalactivitytookplaceinaperiodfrom7days to6weeks,witharecurrenceraterangingfrom7.5%to8.2% (Fig.2).
Surgicaltimeandreturntonormalactivity
112
jcoloproctol(rioj).2016;36(2):104–114PPH technique
Surgical time
Return to normal activity
Recurrences Pain
17.5-35 min
VAS scale
Day 0-Day 1-Day 7
5/3/2.4
7 days-6 weeks
7.5-8.2%
Fig.2–Distributionofstudiesaccordingtosurgicaltime,pain,returntoactivityandrecurrencesinthePPHtechnique,
2009–2015.
foundasurgicaltimeof31min,withatimeofreturnto activ-ityof6weeks.Wang etal.,20intheircomparativestudy of Milligan–MorganversusPPHtechniquesconductedina hospi-talinChina,notedasurgicaltimeof18.3min;however,these authorsdidnotevaluatethereturntoactivity.
ThestudysolelyonPPHtechniqueconductedbyMederos etal.18 ina hospitalinPeruhad theshortersurgicaltime, 17.5min;andinthestudybyGurayaandKhairy,12theduration ofthesurgicalprocedurewas21.7min,andasintheseother citedstudies,thereturntoactivityhasnotbeenevaluated.
Painandrecurrences
InstudiesusingtheVASscale,theaveragepainondayzero wasgrade5;onday1,grade3;andonday7,grade2.4,with recurrenceof7.5–8.2%.Thus,Kashanietal.16demonstrated thatthemostintensepaingotgrade4onday0and1.7onday 7,withrecurrenceof7.5%.Wangetal.18obtainedgrade5on day0;grade3onday1;andonsubsequentdays,anaverageof 2.4;therecurrencewasnotevaluated.InthestudybyLucarelli etal.,19theaverageofthethreesituationsofpainassessment intheVASscalewas=3,witharecurrenceof8.2%.
AswasseenwiththeapplicationoftheVASscale, postop-erativepainwaslower,particularlyonday7,comparedwith theconventionaltechnique.Thisfindingmayalsobe associ-atedwithanearlierreturntonormalactivityandwithabetter well-beingofthepatient,alsointhe immediate postopera-tiveperiod.However,althoughPPHpresentsalargenumber ofcomplications,generallytheoverallindexissimilartothat oftheconventionaltechnique.3
However,althoughPPHpresentsalargenumberof compli-cations,generallytheoverallpercentageissimilartothatof theconventionaltechnique.Inaddition,PPH“isnoteffective forbulkyexternalhemorrhoids,orforthethrombosedones”.3
LigaSureTM
ThistechniquewasdescribedbyJoelSayfan2001;init,one usesabloodvesselsealanttoolknownasLigaSureTM.21
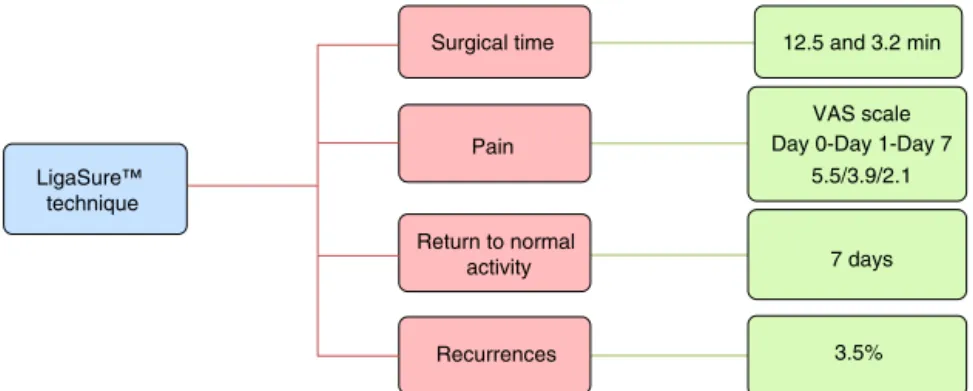
Using LigaSureTM, surgical times ranged from 12.5 to 13.2min.Onaverage,theEVAscaleondayzerowas5.5 (mod-erate);onday1,3.9(slight);andonday7,2.1(light).Patients returnedtoactivityafter7days;3.5%ofthemrelapsed(Fig.3).
Surgicaltimeandreturntonormalactivity
InthestudyconductedbyKhannaetal.,10thesurgicaltime was12.5minandthereturntoactivityoccurredin7days.In thestudybyJaramilloetal.,9thesurgicaltimewas13.2min, and the return to activity also took place in 7 days. The LigaSureTM techniqueshowedthesmallestvariationin sur-gicaltime;therefore,thisisanoptimalsurgicaloptionwith regardtothecontrolofpost-operativeinfections,aswellas promotinganearlierreturntopreoperatoryroutine.
Painandrecurrence
Khanna et al.10 report that the pain in VAS scale on day zero=4.9; on day 1=3.8; and on day 7=1.4; recurrences occurred in3.5%ofcases.Jaramilloetal.9 reportedthat,in theirstudy,thepaininVASscaleonday0=6.1;onday1=4.1; andonday7=2.8.Norecurrenceswerereported.
ThehemorrhoidalresectionwithLigaSureTMisanoptimal alternative,byallowingsurgicaltimereduction,ofthe anal-gesicsneededinthefirst24h,andofpostoperativepain.21,22 Thepresenceofseverepainwithinthefirst24haftersurgery maypromoteurinaryretentionandconstipation.10
Compared with conventional hemorrhoidectomy, the LigaSureTM method attenuates postoperative pain and the needtoprescribeparenteralanalgesia,sincethereisa mini-malthermalexpansionandalsobythelackofsutures.3
Hemorrhoidaltransanaldearterialization(THD)
DescribedbyMorinagaetal.in1995inordertobeanew sur-gicalapproachinthetreatmentofhemorrhoids,THD“usesa kitwithanoscopethatreachestheupperportionofthedistal rectum,wherewithaDopplerdevicepinpointstheterminal branchesofthehemorrhoidalarteriesinpositions1,3,5,7,9 and11hintherectalcircumference”.Thesevesselsare cran-iocaudallyconnected[...]“totheupperandlowerportionsof
the ligationand areattached; withthis,prolapsereduction andfixationoccur”.3
jcoloproctol(rioj).2016;36(2):104–114
113
Surgical time
Pain
Return to normal activity LigaSure™
technique
Recurrences
12.5 and 3.2 min
VAS scale Day 0-Day 1-Day 7
5.5/3.9/2.1
7 days
3.5%
Fig.3–Distributionofstudiesaccordingtosurgicaltime,pain,returntoactivityandrecurrencesintheLigaSureTM
technique,2009–2015.
THD technique
Surgical time 23-25 min
VAS scale Day 0-Day 1-Day 7
5.5/3.0/1.4
7-14 days
20-22.5% Pain
Return to normal activity
Recurrences
Fig.4–Distributionofstudiesaccordingtosurgicaltime,pain,returntoactivityandrecurrencesintheTHDtechnique,
2009–2015.
Surgicaltimeandreturntonormalactivity
InthestudybyLucarellietal.,19thesurgicaltimewas35min andthereturntoactivitytookplacein14days.Ontheother hand,inthestudybyGomez-Rosadoetal.,22performedina clinicinSpainandthatevaluatedonlyTHD,thesurgicaltime wasabout23min,andthereturntoactivitytookplacein8 days.
ComparedwithLigaSureTM,THDshowedarelativelylonger surgicaltime; however,this surgicaltime issimilartothat for PPH, and shorter than that for the conventional tech-nique,suggestingthat THDisagoodoption. Thereturn to activityoccurred inashortertimewhencomparedto con-ventionaltechniquesandPPH.Inaddition,THDhasthebest cost-benefit ratio, as well as a less intense postoperative painversusPPH.Thediseaserecurrencewassimilarforboth techniques.3
Painandrecurrence
Thevariationinobservedpainwassimilartothatfoundby Gomez-Rosadoet al.,22and therecurrenceratewasaround 22.5%.;ontheotherhand,thestudy conductedbyLucarelli etal.19demonstratedanaveragepaingradeofapproximately 4(light)intheevaluateddays, with20%recurrencerate. A studycomparing THDversus PPHfortreatmentofgradeIII hemorrhoidal disease concluded that both techniques are comparable.THDhasthebestcost-effectiverate,aswellas alessintensepainversusPPH.Recurrenceratesweresimilar.1 Incontrast,thestudy demonstrateshigherrecurrencerates forTHDtechnique.
ItwasobservedthatafterthepublicationofThompson’s studiesin1975onthepathophysiologyofthisdisease, sev-eralsurgicaloptionshaveemerged,inanattempttocorrect thechangesinthevascularcushionsandsupportingtissue ofthesestructures.Therefore,surgicaltreatmentshouldbe basedonsymptoms,disease classification,andselectionof individual patients,soonecanofferthe bestsurgical tech-niqueforeachcase.Thus,anaspectexceedinglyimportant, tobeexaminedbythesurgeon,isthepropercareofthepain postoperatively,sincepaincanbeahindrancetotheuseofa particulartechnique,evenwhenmoremodernandefficient.3
Conclusion
Conventional techniquesare still the most practiced,with goodacceptanceastothelong-termresolutionandtothelow recurrencerate,despiteaperiodofslowerrecoveryandmore intensepain.Thelatesttechniques,asTHDandLigaSureTM, showgoodresultsingradeIIIdisease,withshortersurgical timesandlesspain,butwithunsatisfactorylong-termresults. Thusnewstudiesarerequiredforasaferevaluation.
114
jcoloproctol(rioj).2016;36(2):104–114environmentthatarecrucialtoagoodunderstandingofthe hemorrhoidectomy.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. ImbelloniLE,VieriaEM,CarneiroAF.Postoperativeanalgesia
forhemorrhoidectomywithbilateralpudendalblockadeon
anambulatorypatient:acontrolledclinicalstudy.J
Coloproctol.2012;32:291–6.
2. MalokuH,GashiZ,LazovicR,IslamiH,Juniku-ShkololliA.
Laserhemorrhoidoplastyprocedurevsopensurgical
hemorrhoidectomy:atrialcomparing2treatmentsfor
hemorrhoidsofthirdandfourthdegree.ActaInformMed.
2014;22:365–7.
3. CeratoMM,CeratoNL,PassosP,TreiguerA,DaminDC.
Tratamentocirúrgicodashemorróidas:análisecríticadas
atuaisopc¸ões.ArqBrasCirDig.2014;27:66–70.
4. ChenJS,YouJF.Currentstatusofsurgicaltreatmentfor
hemorrhoidssystematicreviewandmeta-analysis.Chang
GungMedJ.2010;33:488–500.
5. MottaMM,SilvaJúniorJB,SantanaLO,FernandesIL,Moura
AR,PrudenteACL,etal.Tratamentodadoenc¸ahemorroidária
comligaduraelástica:estudoprospectivocom59pacientes.
RevBrasColoproct.2011;31:139–46.
6. FerrariLC,JamierL,BorrionuevoM,AndradaDG.Análisisy
ResultadosdelaOperacióndeFergusonemelTratamientode
laEnfermedadHemorroidal.RevArgentColoproct.
2013;24:85–9.
7. MarianelliR,MachadoSPG,AlmeidaMG,BaravieraAC,
FalleirosV,LolliRJ,etal.HemorroidectomiaConvencional
VersusHemorroidopexiaMecânica(PPH).Estudo
Retrospectivode253Casos.RevBrasColoproct.2009;29:30–7.
8. SouzaMT,SilvaMD,CarvalhoR.Revisãointegrativa:oqueée
comofazer.Einstein.2010;8:102–6.
9. JaramilloLI,BeltránMA,BozzoI,LarracheaP,GonzálezF.
Estudiocomparativoentrehemorroidectomíacerradade
FergusonyhemorroidectomíacomLigaSureTM.RevColomb
Cir.2011;26:171–9.
10.KhannaR,KhannaS,BhadaniS,SinghS,KhannaAK.
Comparisonofligasurehemorrhoidectomywithconventional
Ferguson’shemorrhoidectomy.IndianJSurg.2010;72:294–7.
11.LuM,ShiGY,WangGQ,WuY,LiuY,WenH.Milligan–Morgan
hemorrhoidectomywithanalcushionsuspensionandpartial
internalsphincterresectionforcircumferentialmixed
hemorrhoids.WorldJGastroenterol.2013;19:5011–5.
12.GurayaSY,KhairyG.Stapledhemorrhoidectomy;resultsofa
prospectiveclinicaltrialinSaudiArabia.JClinDiagnRes.
2013;7:1949–52.
13.AzolasR,VillalónR,DanillaE,HasbúnA,GaticaF,Salamanca
J.Hemorroidectomíacerradaysemicerrada:Estudio
prospectivoaleatorizado.RevChilenaCir.2010;62:382–6.
14.RoldósLEV.Nuevatécnicaquirúrgicaparaeltratamientode
laenfermedadhemorroidal.RevCubanaCir.2010;49.
15.SilvaFC,DeliberatoPCP.Análisedasescalasdedor:revisãode
literatura.RevBrasCiênSaúde.2009;7:86–9.
16.KashaniSMT,MehrvarzS,NaeiniSMM,RezaE.
Milligan–Morganhemorrhoidectomyvsstapled
hemorrhoidopexy.TraumaMon.2012;16:175–7.
17.PapisD,ParodiM,HerreríasF,SánchezA,GómezL,SierraJE,
etal.HemorroidectomíaconLigasurevsdiatermia
convencional:Análisisretrospectivomonocéntrico.Acta
GastroenterolLatino-am.2013;43:284–7.
18.MederosLAB,EleraJOAP,PinedaAJM.Procedimientopara
hemorroidesconprolapsodemucosa:TécnicadeLongo.
Reportepreliminar.RevMedHered.2009;20:190–4.
19.LucarelliP,PicchioM,CaporossiM,DeAngelisF,DiFilippoA,
StipaF,etal.Transanalhaemorrhoidaldearterialisationwith
mucopexyversusstaplerhaemorrhoidopexy:arandomised
trialwithlong-termfollow-up.AnnRCollSurgEngl.
2013;95:246–51.
20.WangZG,ZhangY,ZengXD,ZhangTH,ZhuQD,LiuDL,etal.
Clinicalobservationsonthetreatmentofprolapsing
hemorrhoidswithtissueselectingtherapy.WorldJ
Gastroenterol.2015;21:2490–6.
21.NahasSC,PintoRA,DiasAR,ChowB,NahasCSR,Marques
CFS,etal.Médicosresidentespodemrealizarcomseguranc¸a
eeficiênciatécnicasdeMilligan–Morgan,Fergusone
grampeadoresnotratamentocirúrgicodashemorróidas?Arq
BrasCirDig.2011;24:210–4.
22.Gomez-RosadoJC,Sanchez-RamirezM,Capitan-MoralesLC,
Valdes-HernandezL,Reyes-DiazML,Cintas-CatenaJ,etal.
Resultadosauma ˜notrasdesarterializaciónhemorroidal