w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
A
novel
approach
to
lower
rectal
anastomosis:
technique
innovation
and
the
preliminary
report
of
twenty
cases
Abbas
Alibakhshi
∗,
Yosra
Jahangiri,
Fereydoun
Sirati,
Sayed
Mahdi
Jalali,
Mohammad
Sadegh
Nikdad,
Arezou
Abbasi,
Mohsen
Afarideh
DepartmentofGeneralSurgery,ImamKhomeiniHospitalComplex(IKHC),TehranUniversityofMedicalSciences,Tehran,Iran
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received4December2015
Accepted25March2016
Availableonline13April2016
Keywords: Colorectalsurgery
Lowrectalstapleranastomosis Pull-through
Transanal Transabdominal
a
b
s
t
r
a
c
t
Backgroundandaims: Todescribeapracticaltechniqueinnovation(transanal‘Pull-through’ approach)asa feasible,safeandeffectivealternativetotheconventional transabdomi-nalstaplerlowrectalanastomosisinlesionsofminimalanatomicaldistinctionfromthe adjacentintactmucosa.
Materialandmethods:Prospectivecase-seriesofpatientswithlowrectalcancers,familial adenomatouspolyposis(FAP)andulcerativecolitisundergoingPull-throughtransectionand verylowrectalanastomosisusinglinearTA-90noncuttingstaplerandcircularstapler-cutter. Results:Inthisseries,twentypatients(11menand9women)underwentproctectomyby thetransanalPull-throughtechnique.Barringoneofthepatientsthatdevelopedapelvic abscessintheimmediatepostopfollow-up,surgicalprocedureandthelong-term follow-upperiodwasuncomplicatedwithnocriticalfindingsofleakage,stenosisandbleeding. Thepostoprateofinfectionandfecalincontinencewasnotsignificantlydifferentbetween gendersanddifferentagegroupsofthestudy.Themeanoperativetimewascalculated 169.9±11.1minutes.
Conclusion:Pull-throughtransectionprocedureusingtheTA-90non-cuttingstaplerisasafe, efficientandeconomically soundtechnique implicatedin low-lyingrectal lesions.The transanal‘Pull-through’approachisparticularlyhelpfulinsituationswherethedirect visu-alizationoflowerrectalmucosachangestheprognosisthroughdeterminingthemarginal extent of intact/involvedmucosa (e.g., FAP, villousadenomas, rectal polyps and
post-neoadjuvantchemoradiotherapytumors).
©2016SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](A.Alibakhshi). http://dx.doi.org/10.1016/j.jcol.2016.03.006
Uma
nova
abordagem
para
a
anastomose
retal
mais
baixa:
inovac¸ão
técnica
e
relatório
preliminar
de
cinte
casos
Palavras-chave: Cirurgiacolorretal
Anastomoseretalbaixacom grampos
Abordagempull-through
Transanal Transabdominal
r
e
s
u
m
o
Experiênciaeobjetivos: Descreverumainovac¸ãotécnicaprática(abordagemtransanal pull-through)comoumaalternativaviável,seguraeeficazàanastomosetransabdominalretal
baixaconvencionalcomgramposemlesõescommínimadiferenciac¸ãoanatômicacom
respeitoàmucosaintactaadjacente.
Materialemétodos: Estudoprospectivodesériedecasosdepacientescomcânceresretais baixos,poliposeadenomatosafamiliarecoliteulcerativasubmetidosàtransecc¸ão
pull-througheaumaanastomoseretalmuitobaixacomousodeumgrampeadorlinearnão
cortanteTA-90eumgrampeadorcortantecircular.
Resultados: Nestasérie,20pacientes(11homens,9mulheres)foramsubmetidosauma proctectomiapelatécnicatransanal pull-through.Àexcec¸ãodeum dospacientes,que
apresentouum abcessopélviconoseguimentopós-operatórioimediato,nãoocorreram
complicac¸õescomoprocedimentocirúrgicoeaolongodoprolongadoperíodode segui-mento,nemhouveachadoscríticosdevazamento,estenoseousangramento.Opercentual deinfecc¸ãoeincontinênciafecalnopós-operatórionãofoi significativamentediferente entregênerosenasdiferentesfaixasetáriasdospacientesenvolvidosnoestudo.Otempo cirúrgicomédiofoide169,9±11,1minutos.
Conclusão: Oprocedimentodetransecc¸ão pull-through comousodogrampeadornão cortanteTA-90étécnicasegura,eficazeeconomicamenteconfiávelparausoemlesões retaisbaixas.Aabordagemtransanalpull-throughtemparticularutilidadeemsituac¸ões nasquaisavisualizac¸ãodiretadealterac¸õesnamucosaretalmaisbaixamudao prognós-tico,medianteadeterminac¸ãodaextensãomarginaldamucosaintacta/envolvida(p.ex., FAP,adenomasvilosos,póliposretaisetumorespós-quimiorradioterapianeoadjuvante).
©2016SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este éumartigoOpenAccesssobalicençadeCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Althoughconventional end-to-endanastomosis (EEA)
tech-niquesare often viewed asan excellent option inaselect
number of lower colorectal diseases,1 the problems of a
complicatedanastomosis;inparticularinsiteswithlimited
anatomical access such as depth of the pelvic cavity, has
ledmanygastrointestinaloncologistsurgeonstoseek alter-nativetreatingoptionstoovercomethischallenge.Ensuring theanastomoticsecurityisespeciallyimportantbecauselife threateningpotentialofEEAfailureinrectalcancersufferers
isassociatedwithincreasedrecurrencerate,which further
deterioratestheprognosis.2–4
Currently,intra-abdominaltransectionofrectallesionsis routinelyperformedusingdifferenttypesofstaplers.5
How-everand aside from concerns over a possibleanastomotic
leak that could persist with double stapling,6
operator-dependencyandthehighexpensesofcurvedstapler-cutters
used in these settings, many preclude its widespread use
in certain regions with limited financial power.
Addition-ally, unconfident determination of safe margin border in
lesionswith seeminglyinseparablegrossmorphology from
theadjacentintactmucosa(e.g.,familialadenomatous
poly-posis[FAP]andpost-neoadjuvantchemoradiotherapyrectal
tumors) is another restraint to the use oftransabdominal
procedures.
Herein,weaimedtodescribeanovelyetsimpleand
prac-ticaltechniqueinnovationforperforminglowandverylow
rectalanastomosesusingdifferentsetofstaplerswithaneye
toresolvetheaforementionedshortcomings
Material
and
methods
Weprospectivelyexaminedtheproposed‘Pull-through’EEA
techniqueontwentyconsecutivecandidatesofelective
proc-tectomywhofulfilledtheeligibilitycriteriatoenterourstudy
in the Imam KhomeiniHospital Complex (IKHC, atertiary
referralteachinghospitalaffiliatedwithTehranUniversityof MedicalSciences)fromJanuary2011toFebruary2012. Institu-tionalreviewboard(IRB)exemptionswerepreviouslyobtained
inaccordancewiththeHumanSubjectsResearchpolicy.In
addition, writteninformedconsentwasreceivedfromeach
oftheparticipating patients.From ourperspective,
sugges-tive indicationsfortransanalPull-through approachto the
lower rectalanastomosis includedsmall tomoderate sized
lesionsofthemiddletoverylowerrectum,post-neoadjuvant
chemoradiation therapy tumors without a palpable tumor
margin, FAP, villousadenoma, otherbenign/malignant
out-growntissuesandotherindicationsofelectiveproctectomy
(e.g.,ulcerativecolitis,UC).Weexcludedobesepatients(body massindex>30kg/m2)duetoacomplicatedcourseofsurgery,
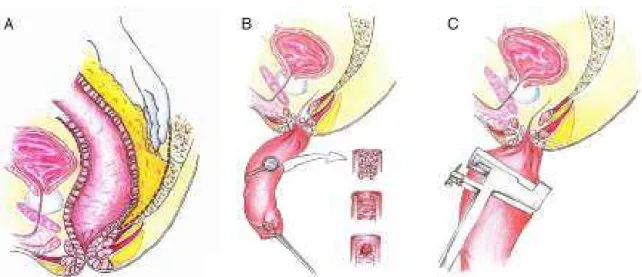
Fig.1–Intra-operativeimagesofthestapled“Pull-through”end-to-endanastomosis(EEA)inapatientswithfamilial adenomatouspolyposis(FAP).(A)Transanalgraspoflowerrectumasfacilitatedbytheuseofspongestick;(B)applicationof thelinearnun-cutterTA-90staplerinthestableileoanalEEAanastomosis.Notethelevelatwhichtransectionisperformed onthelowerrectallumenshouldbeimmediatelyadjacenttothedentatelineinpatientswithFAP.
withthepotentialofanalrimincarcerationwerealsoexcluded fromthestudy.
Surgicaltechnique
Patients were scheduled for the operation, received bowel
preparation in the OR and placed in a lithotomy/V
posi-tion.Underthegeneralanesthesia,aperi-umbilicalmidline
incisionwascuttodiagnosticallyexploretheabdomenand
determinewhetherthemassisresectable,withfurther supra-pubicextensionoftheincisionline.Initialstepsofprocedure
wereperformedasperthestandardtransabdominalstapled
anastomosis.Followingamidtolowrectaltransection
(keep-ing a minimum 5-cm distancefrom the superior plane of
levators and pelvic floor), a peri-rectal dissectionwas
per-formed toease the passageof freed rectal stump down a
dilatedanalcanalasdescribedbelow.Ofnote,amechanical barrierwasformerlylocatedbetweenthefieldofresectionand thesuperiorleveloflevatorstoavoidmechanicalsphincteric
manipulationanddamageduringthePull-throughprocedure.
TheLigaSure vessel sealingsystem (ValleyLaboratory Inc.,
Boulder,CO)wasemployedfortheresectionof mesorectosig-moidcolonortotalmesorectalexcision(TME)tofreerectum
from the nearby bony sacrum. Considering the
anatomi-calproximitybetweenurinary tractand lateral rectalwall,
dispatching their inter-connecting adhesions required an
exhaustivelymeticulousapproach.Bychangingthesurgical
positiontocommencetransanaleversion,alargespongestick
clampwasenteredinsidetheanalcanaltodrawandevert
theseveredrectumcutedgeresultingintherectal exterior-izationandexposureofinner surface(i.e.,exposureofthe rectalmucosa).Weensuedtheoperationbyresectingselected
mucosalspecimenswitha1.9mmdistance(anincreasefrom
the maximum 1.5mmdistance inthe transabdominal
sta-pler method) from the predetermined site of safe margin
as marked by alinear noncutting TA-90mmstapler
(Covi-dienTATM 90mm).InFAPandother globalpathologies,the
lineofstaplingshouldbeideallypositionedashigh upthe
everted rectumas possible,next tothe pectinate (dentate)
linetoextirpatetheresidualat-riskrectalmucosa.Priortothe
insertionoftheanalcanal,oversewnandcontinuously
run-ningsuturesreinforcedthenewlyformedrectal/analpouchto ensureanincreasedlevelofstability;thushelpingreducethe
riskofleakinganastomosis.25-mmanvilof29–33mm
circu-larstapler(PROXIMATE®ILSCircular,Ethicon,Endo-Surgery,
Cincinnati,OH,USA)wasanchoredendoluminallyon
proxi-malcolon/distalileumtoformastandardstapledanastomosis
withtherectal/analpouch.Beforethetransanalpassageof
circular stapler in preparation forfiring, anvil was reposi-tionedfromtiltedtoaflatpositiontoenableanastomosisof
the pouchwithproximalcolonicJ-pouch/distalilealpouch.
Finally,attachmentofthespikeofcircularstaplertotheanvil
head signaled the conclusion of Pull-through lower rectal
EEA. Assurancefora fully functioninglower rectal
anasto-mosis was post-operatively assessed through air injection
(Figs.1and2).
Eachpatientwasprescribed tostart his/herroutinediet
onthe postopday3.Perioperativeandlong-termfollow-up
ofthe patientsincluded recorded dataon fecalcontinence
andthefrequencyofbowelmovementsaswellastherateof
developingcomplications,recurrences,morbiditiesand
mor-talities.Previousestimationofpreoperativestagingthrough
computedtomography(CT)scanimagery±endoscopy
Fig.2–SequentialoverviewofthePull-throughprocedureinschematicrepresentations.(A)Totalmesorectalexcision(step 1);(B)thetransanal“Pull-through”end-to-endanastomosis(EEA)isparticularlyoptimizedforpathologiesthatdonot obstructthelumenandarenotreadilydistinguishedfromthenormalneighboringmucosa(e.g.,familialadenomatous polyposis,ulcerativecolitisandpost-chemoradiationtumors(step2);(C)lateralplaneviewoftheevertedrectalmucosa underthedirectviewofsurgeonfollowingstaplingwithTA-90mmlinearstapler-noncutter(step3).
Statisticalanalysis
ClinicalendpointdataforthisstudywasenteredtoPASW soft-wareV18.0(IBMCorp.,Armonk,NY).Categoricalvariablesare
expressedasfrequencies(%)and were comparedbyFisher
exacttest.Continuousbaselinecharacteristicsareexpressed
as mean±standard deviation (SD). Since the normality of
data was previouslyassessed and rejected by goodness of
fitShapiro–Wilktest,between-groupcomparisonsacrossthe
twoandthreegroupswasmadeusingMann–WhitneyUand
Kruskal–WallisHtests,respectively.Two-sidedstatistical sig-nificancewaspresetatp<0.05.
Results
Fromthe20analyzedcases(twelvemenandeightwomen),
nine had rectal cancer (seven cases of rectal cancer had
underwentprevious neoadjuvantchemoradiationsessions),
oneulcerativecolitis(UC)and theten others hadFAP. The
average distance of the mass lesion from the anal verge,
asconfirmed byrigid sigmoidoscopy work-upwas
approx-imately 6cm. The mean±SD length of remaining rectal
cuffforcreatingcolorectal/ileo-rectal pouchwas measured
at 3.4±2.2cm (excluding FAP patients), depending on the
locationoftumor/lesionfromthedentatelineandwitha
min-imumof2cmsafemargindistancefromthedistaltumorfree
border.ForpatientswithFAP,rectaltransectionwascarefully donejustabovethedentatelinetodiminishtheriskof
micro-metastasisandrecurrencesofremainingpolyps.Medianage
ofstudy participants was 49 years,ranging from 18 to 71.
Histopathologyevaluationsdemonstrated allresected
sam-plestohavetumor-free margins. Themeanoperativetime
wascalculated169.9±11.1minutes,withnosignificant differ-encebetweengenders(170.8±9.7forfemalesvs.169.1±12.6 formales;p=0.6)anddifferentagegroups(171.0±5.7forage group<30,166.0±9.7for30≤agegroup<50and174.4±12.9;
p=0.2). The observation ofa slight leak afterair injection
promptedustoperformtwodefunctioningileostomyinour
series, one in a patient with post-neoadjuvant rectal
can-cer and another in a case with UC. Excluding one of the
patients who developeda pelvicabscessinthe immediate
postop follow-up, therewere nocritical post-surgical
com-plicationsnamely,bleeding,leakage,incontinenceandfistula
formation. Mild and transient (lastingfor 3and 4months,
respectively)gasincontinence,notinterferingwithengaging
in dailynormalactivities, occurred intwo cases(one with
rectal cancer and the other with FAP;assessed by clinical
evaluation).Woundinfectionwasalsoreportedintwocases,
withneitherrequiringreoperation.Themean±SD
hospital-izationperiodwas5.7±1.1daysandpatientsweredischarged thereafter;similarlywefoundnostatisticallysignificant
dif-ferencesintermsofhospitalstaybetweenfemalesandmale
anddifferencecategoriesofparticipants”age(pforall
non-significant). Patientswere followedforameanpreoperative
periodof2.5±0.6years,withnoreportofstricture,functional
outcomesandmortalityduringthisperiod.
Discussion
Colorectalsurgerieshavedrasticallyevolvedduringthepast
few decades.The emergence ofColo- and ileoanalstapled
EEAtechniqueshavepropelledthe developmentofmodern
verylowrectalanastomosisandreducedtheriskofleakage
andother complications.7,8 Forlowanastomosisingeneral,
ahigherincidenceofurgentdefecation,fecalincontinence,
evacuation disorders, coupled with frequent bowel
move-ments are expected.9 However, very low rectal resections
locatedwithin5cmdistancefromtheanalvergerepresenta
technicallysuperiorchallengeduetohavingacomparatively
increasedriskforanastomoticcomplicationandthe
Considering numerous problems characteristic of the
resectionoflow lyingrectaltumors, surgeonshavesought
manyalternativemanualorrobotictechniques,toapproach
lesionsofthisareaofthegut.10–15 In1972,Parksdescribed
reestablishinganorectalcontinuitywithahandsewncoloanal
anastomosis by a perineal approach in intersphincteric
resectionofbenignconditions.16 Sincethen,manyauthors
haveadoptedahand-sewncoloanalanastomosismethodor
variationsthereof,evenasasalvageprocedurefollowingfailed attemptsofstapledanastomosis.17
Whilethecoloanalhandsewnanastomosisisconsidered
bymanyasanexcellentoption,17stapledEEAisrecentlybeing
preferredbysomesurgeons,5 whichhasled tocontroversy
instandardizationofcareinlowlyingrectalcancers.18
Sev-eralMeta-analysesand Cochrane-basedsystematicreviews
have compared the efficacy of the handsewn and stapled
anastomoses in lower rectal operations with controversial
results.19–22 Although ileostomy closure using stapler and
suturedanastomotictechniqueswerecomparableintermsof
anastomoticleak,surgicalsiteinfection,readmission, reop-erationsandhospitalizationperiod,stapledanastomosiswas associatedwithashorteroperativetimeandlowerriskof post-operativesmallbowelobstruction.23Neverthelessandasour
experiencewithcolorectalanastomosissuggest,
transabdo-minalstapledtechnique(indepthofthepelviccavity)hastwo
majordrawbacks:
(I) Inadequate transabdominal stapling performed by the
novice surgeon is associatedwith an increasedrisk of
post-surgicalanastomoticdehiscencethatmayresultin
reparation,highermorbidity,hospitalstayandmortality,
permanentcolostomywithahighrateof,24 anal
steno-sisandlocalrecurrencesoftherectaltumors.25Straight EEAlinescreatedbylinearTA-90staplingdeviceinsteadof gastrointestinalanastomosis(GIA)/Contourstapler-cutter curvedlines,andincreasedside-to-sideanastomoticspan
from40mminthetransabdominalstapleranastomosisto
90mminthePull-throughprocedurepreventsischemia
intheEEAcorners(triangleischemia)andfoldingofthe coloncutedges,respectivelyandsafeguardthecolorectal anastomosis.
(II) In post-neoadjuvant chemoradiotherapy rectal cancers
or FAP, safe margin determination becomes a
diffi-cult taskdue to mainlynon-palpable lesions.Assuch,
directmucosalinspectioninthe transanalPull-through
approach would be superior to the blind
transec-tion in conventional stapled anastomosis to clearly
differentiate intact from involved rectal mucosa and
subsequentlypreventinvasiveovertreatmentprocedures
that could potentially result in a dysfunctioning anal
sphincter.
Our described approach is in many ways, an upgrade
tothe predecessor Pull-throughtechniqueas developedby
Toupet, which in turn is a modification of Duhamel
Pull-through procedure.26 The essence of Toupet Pull-through
techniqueincludes ananterior colorectal intubationand a
temporary perineal colon anus. The author suggested the
newly found anastomosis can doubly protect against the
developmentoffistulaefromanastomoticdisunion.27Whilst
the maximum anastomoticsupportgained from the initial
useoflinearnoncutterstaplerandsubsequentoversewingof
suturedtumormarginscanobviatetheneedfortheproximal
ostomy,24 ourapproachisunique toprovidedirectperineal
visualization of non-palpable lesions (e.g., FAP and
post-chemoradiationrectalcancers)whereaprecisesafemargin
determination remains fundamental to achieve consistent
results.
Itshouldbenotedtheproposed ‘Pull-through’approach
to lower rectalanastomoses bearssomeconsiderable
limi-tations. Transanal extractionofthe lower rectal part turns
ineffective once comparatively large lesions of rectal
ade-nomas blockthe entryoffull-thicknessrectalmucosa into
the dilatedanal opening. Additionally,extirpation ofrectal
mucosainpatientswithFAPrequiresexpertandmeticulous
transectionofrectumdowntothedentatelinetolowerthe
risk ofresidual microscopic polyp and metastasis. Finally,
because of the limited number ofincluded patients and a
relatively short-term follow-up period, the safety and
effi-cacyofthedescribedtechniqueisnotentirelyapplicableto thepatientsofpreviousstudies.Theadvantagesofthis
tech-nique includea thorough scrutiny of tumormargin under
directvisualizationofrectalmucosa,minimalriskof compli-cations(e.g.,anastomoticleak), simplicityofthe procedure
compared to transabdominal stapler EEA (in particular, in
patients withanatomically smallpelvis).Thecost-effective
natureoftransanalPull-throughapproachduetoaffordable
use oflinearnoncuttingTA-90staplers(costperunitupto
$150) as opposed to the additional high costs imposed by
the use ofcurved staplercutter (up toa total of$500 per
surgical set in our country) can be a viable resource
sav-ing strategyinthesettings ofmiddletolowerrectaltumor
surgeries.
Conclusion
Indicated for medium to low rectal anastomoses, the
sphincter-preserving transanal Pull-through EEA is an
effi-cient clinical asset and easily applicable to both benign
andmalignantdiseases.ImplementationofthePull-through
approach using a TA-90 linear stapler-noncutter and by a
directly visualized mucosectomy (as an alternative to the
expensiveintra-operativeendoscopyinlaparoscopicsettings) isassociatedwithsignificantlylesseconomicburdensonthe
patients. Werecommendcomparativestudiesinvolvingthe
conventional transabdominalstapledorhand-sewn
anasto-mosis methods, and the described Pull-through technique
to endorse the preferred standard ofcare in each setting.
Futurelarge-scalestudiesofthePull-throughapproachshould confirm its safety,efficiencyand feasibilityand investigate whetherthisapproachisequallyreproducibleinlaparoscopic settings.
Conflicts
of
interest
Acknowledgements
Theauthors wishtothankthe patientsand staff ofImam
KhomeiniHospitalComplex(IKHC)fortheirgracious
partici-pationinthisstudy.
r
e
f
e
r
e
n
c
e
s
1. FazioVW,KiranRP,RemziFH,CoffeyJC,HeneghanHM,Kirat HT,etal.Ilealpouchanalanastomosis:analysisofoutcome andqualityoflifein3707patients.AnnSurg.2013;257:679–85. 2. NandakumarG,SteinSL,MichelassiF.Anastomosesofthe
lowergastrointestinaltract.NatRevGastroenterolHepatol. 2009;6:709–16.
3. PaunBC,CassieS,MacLeanAR,DixonE,BuieWD. Postoperativecomplicationsfollowingsurgeryforrectal cancer.AnnSurg.2010;251:807–18.
4. TelemDA,ChinEH,NguyenSQ,DivinoCM.Riskfactorsfor anastomoticleakfollowingcolorectalsurgery:acase–control study.ArchSurg.2010;145:371–6.
5. KöhlerA,AthanasiadisS,OmmerA,PsarakisE.Long-term resultsoflowanteriorresectionwithintersphincteric anastomosisincarcinomaofthelowerone-thirdofthe rectum.DisColonRectum.2000;43:843–50.
6. AverbachAM,ChangD,KosloweP,SugarbakerPH. Anastomoticleakafterdouble-stapledlowcolorectal resection.DisColonRectum.1996;39:780–7.
7. Villanueva-SáenzE,Sierra-MontenegroE,Pe ˜na-RuizEsparza JP,MartínezHernández-MagroP,Bola ˜nos-BadilloLE.Double staplertechniqueincolorectalsurgery.CirCiruj.
2008;76:49–53.
8. FingerhutA,HayJM,ElhadadA,LacaineF,FlamantY,French AssociationsforSurgicalResearch.Supraperitonealcolorectal anastomosis:hand-sewnversuscircularstaples—a
controlledclinicaltrial.Surgery.1995;118:479–85.
9. BittorfB,StadelmaierU,GöhlJ,HohenbergerW,MatzelKE. Functionaloutcomeafterintersphinctericresectionofthe rectumwithcoloanalanastomosisinlowrectalcancer.EurJ SurgOncol.2004;30:260–5.
10.VelezJP,VillavicencioRT,SchrautW,LeeK.Outcomeanalysis ofexternalcoloanalanastomosis.AmJSurg.1999;177:467–71. 11.JooJS,LatulippeJF,AlabazO,WeissEG,NoguerasJJ,Wexner
SD.Long-termfunctionalevaluationofstraightcoloanal anastomosisandcolonicJ-pouch.DisColonRectum. 1998;41:740–6.
12.WilliamsN,Seow-ChoenF.Physiologicalandfunctional outcomefollowingultra-lowanteriorresectionwithcolon pouch–analanastomosis.BrJSurg.1998;85:1029–35.
13.HuberFT,HerterB,SiewertJR.Colonicpouchvs.side-to-end anastomosisinlowanteriorresection.DisColonRectum. 1999;42:896–902.
14.ManceauG,KarouiM,BretonS,BlanchetAS,RousseauG, SavierE,etal.Rightcolontorectalanastomosis(Deloyers procedure)asasalvagetechniqueforlowcolorectalor coloanalanastomosis:postoperativeandlong-term outcomes.DisColonRectum.2012;55:363–8.
15.KangJ,HurH,MinBS,LeeKY,KimNK.Roboticcoloanal anastomosiswithorwithoutintersphinctericresectionfor lowrectalcancer:startingwiththeperianalapproach followedbyroboticprocedure.AnnSurgOncol.2012;19:154–5. 16.ParksA.Transanaltechniqueinlowrectalanastomosis.Proc
RSocMed.1972;65:975.
17.TekkisP,TanE,KontovounisiosC,KinrossJ,GeorgiouC, NichollsRJ,etal.Hand-sewncoloanalanastomosisforlow rectalcancer;techniqueandlongtermoutcome.Colorectal Dis.2015.
18.RullierE,DenostQ,VendrelyV,RullierA,LaurentC.Low rectalcancer:classificationandstandardizationofsurgery. DisColonRectum.2013;56:560–7.
19.NeutzlingCB,LustosaSA,ProencaIM,daSilvaEM,MatosD. Stapledversushandsewnmethodsforcolorectal
anastomosissurgery.TheCochraneLibrary;2012. 20.MatosD,AtallahÁN,CastroAA,SilvaLustosaSA.Stapled
versushandsewnmethodsforcolorectalanastomosis surgery.TheCochraneLibrary;2001.
21.MacRaeHM,McLeodRS.Handsewnvs.stapledanastomoses incolonandrectalsurgery.DisColonRectum.1998;41:180–9. 22.ChoyPY,BissettIP,DochertyJG,ParryBR,MerrieA,Fitzgerald
A.Stapledversushandsewnmethodsforileocolic anastomoses.TheCochraneLibrary;2011.
23.SajidM,CraciunasL,BaigM,SainsP.Systematicreviewand meta-analysisofpublished,randomized,controlledtrials comparingsutureanastomosistostapledanastomosisfor ileostomyclosure.TechColoproctol.2013;17:631–9. 24.NurkinS,KakarlaVR,RuizDE,CanceWG,TiszenkelHI.The
roleoffaecaldiversioninlowrectalcancer:areviewof1791 patientshavingrectalresectionwithanastomosisforcancer, withandwithoutaproximalstoma.ColorectalDis.
2013;15:309–16.
25.AkasuT,TakawaM,YamamotoS,YamaguchiT,FujitaS, MoriyaY.Riskfactorsforanastomoticleakagefollowing intersphinctericresectionforverylowrectal
adenocarcinoma.JGastrointestSurg.2010;14:104–11. 26.KatkhoudaN,KhalilMR,ManhasS,GrantS,VelmahosGC,
UmbachTW,etal.AndréToupet:surgeontechnicianpar excellence.AnnSurg.2002;235:591.