Department of Neurology, São Paulo University, School of Medicine at Ribeirão Preto, Ribeirão Preto SP, Brazil:1MD, Post
gradu-ate student; 2Psychologist;3MD; 4PHD; 5Associate Professor of Neurology.
Received 10 December 2003, received in final form 4 May 2004. Accepted 7 June 2004.
Dr. José G. Speciali - Faculdade de Medicina de Ribeirão Preto, Departamento de Neurologia - Av. Bandeirantes 3900 - 14049-900 Ribeirão Preto SP - Brasil. E-mail: hiltonmariano@uol.com.br
EFFECT OF EPISODIC TENSION-TYPE HEADACHE
ON THE HEALTH-RELATED QUALITY OF LIFE IN
EMPLOYEES OF A BRAZILIAN PUBLIC HOSPITAL
Hilton Mariano Silva Jr
1, Roberta P. Garbelini
2, Simone O. Teixeira
3,
Carlos A. Bordini
4, José G. Speciali
5ABSTRACT - Objective:To evaluate the impact of ETTH on HRQoL in a sample of employees of a Brazilian public hospital. Method:Three hundred and sixty Mário Gatti Hospital employees were asked about headache occurrence in the previous 6 months and completed a SF-36 and a pain questionnaires concern-ing impact of pain (0 to 10 scale) on daily activities, work efficiency, leisure and social activities in previous six months. Two groups were studied: 1. Episodic Tension-type headache group: 127 employees - 81 (63.8%) female and 46 (36.2%), male. 2. Control group: 124, 71 (57.3%) female and 53 (42.7%) male. Results:
ETTH had lowers scores than control in all domains of SF-36; in vitality and bodily pain the difference was statistically significant. Conclusion:Our results indicate that ETTH suffers have impact on HRQoL predom-inantly in vitality. Psychological factors associated to pain may explain this finding.
KEY WORDS: ETTH, headache, HRQoL, SF-36, TTH.
Efeito da cefaléia do tipo tensional episódica na qualidade de vida relacionada à saúde em fun-cionários de um hospital público brasileiro
RESUMO - Objetivo: Avaliar o Impacto de CTTE na QVRS em funcionários de um hospital brasileiro.
Método:Trezentos e sessenta empregados do Hospital Mário Gatti, foram entrevistados. O questionário para avaliação da QVRS SF-36 foi aplicado e a ocorrência de cefaléia nos últimos seis meses foi avaliada. O impacto da dor nas atividades diárias, de lazer, sociais e eficiência no trabalho foi estimado(escala de zero a dez). Resultados:Foram estudados dois grupos: 1. Cefaléia do tipo tensional episódica: 127 emprega-dos - 81 (63,8%) mulheres e 46 (36,2%), homens. 2. Grupo Controle: 124 funcionários, 71 (57,3%) mulheres e 53 (42,7%) homens. As médias do grupo CTTE foram menores que as do grupo controle nos oito aspec-tos avaliados pelo SF-36. Nos aspecaspec-tos vitalidade e dor a diferença foi estatisticamente significativa.
Conclusão:os indivíduos com CTTE apresentaram pior QVRS, predominantemente no aspecto vitalidade. É possível que fatores psicológicos associados à dor possam explicar este achado.
PALAVRAS-CHAVE: cefaléia, cefaléia tensional, QVRS, SF-36.
According to large-scale population surveys epi-sodic tension-type headache (ETTH) is the most pre-valent type of headache. Nevertheless, little has been published about the burden or effect of ETTH on health- related quality of life (HRQoL)1-9. Most of the
research assessing the effect of headaches on the HRQoL has been limited to migraine, indeed. Mi-graine has been associated with significant econom-ic, social and individual burden10 -15.
There are few studies of HRQoL in chronic dai-ly headache (CDH) patients in general population16
or even in specialized headache clinics17. Even though
the majority of the population suffers from ETTH,
information about the impact on HRQoL of those patients is scant.
The present study is aimed to evaluate the im-pact of ETTH on the health- related quality of life in a sample of employees of a Brazilian public hos-pital.
METHOD
After providing informed consent, individuals attend-ed to an evaluation session whose they completattend-ed the validated Portuguese version of the “Medical Outcomes Study Short Form- SF-36”18. Out of the 400 selected
em-ployees, 23 (5.8%) were excluded because they were on vacation; 5 (1.25%) because of removal from their work activities due to health problems and 7(1.75%), with the diagnosis of chronic diseases that could impair the HRQoL. Five employees (1.25%) refused to participate in the stu-dy. Soon after, the 360 remaining employees were asked about headache occurrence in the previous 6 months (clas-sified in agreement with the criteria of 1988 of the In-ternational Headache Society)19. One hundred and nine
employees were excluded from the study since they were diagnosed as suffering from others (non-tensional) hea-dache conditions.
The 251 remaining employees were divided into two study groups:
1. Episodic Tension-type headache group (n = 127, 81 (63.8%) females and 46 (36.2%) males. The group mean age was 36.4 years with a standard deviation of 8.52.
2. Control group (without headache complaint): the-re wethe-re 124 individuals, 71 (57.3%) females and 53 (42.7%) males, with the mean age of 37.8 and a standard devi-ation of 10.2.
There is no statistically significant difference between ETTH and control concerning female distribution.
The pain intensity was assessed on a 10 - point scale where 1 to 3 is defined as “mild”, 4 to 7 as “moderate” and 8 to 10 as “severe”. The degree of disability was asse-ssed by a questionnaire concerning the impact of pain (from 0 to 10 scale) on daily activities, work efficiency, leisure and social activities in the previous six months. The impact was ranked as follows: minimal/ no impact (0 to 2 score), mild (3 to 5 score), moderate (6 to 8 score) and severe (9 to 10 score).
RESULTS
Headache frequency and intensity - As for ETTH, in 54(42.5 %) individuals attacks used to occur up
to once a month; 31 (30. 7%) from 1 to 3 attacks per month; 19 (15%), from 4 to 7 episodes per month; and 15 (11.8%) from 8 to 13 episodes per month. Concerning pain intensity, 42 (33%) experienced only mild attacks, 71 (56%) experienced moderate attacks and 14 (11 %), severe attacks.
Disability - Impact of ETTH on daily activities in
the previous six months - Sixty-two (49%) employ-ees quantified the impact of the pain in the daily activities between 0 and 2; 45 employees (35%) bet-ween 3 and 5; 17 (14%), betbet-ween 6 and 8. Only three employees (2%) reported an important impact (bet-ween 9 and 10), (Fig 1).
Impact of ETTH on leisure, social and family ac-tivities in the previous six months - Sixty-six emplo-yees (52%) quantified the impact of pain in leisure activities, social and family between 0 and 2; 36 em-ployees (28%), between 3 and 5; 19 (15%), between 6 and 8.Six employees (5%), between 9 and 10 (Fig 2).
Impact of ETTH on work efficiency in the previ-ous six months- Seventy-two employees (57%) quan-tified the impact of pain on work efficiency bet-ween 0 and 2; 36 employees (28%), betbet-ween 3 and 5; 14 (11%), between 6 and 8; and 5 employees (4%), between 9 and 10 (Fig 3).
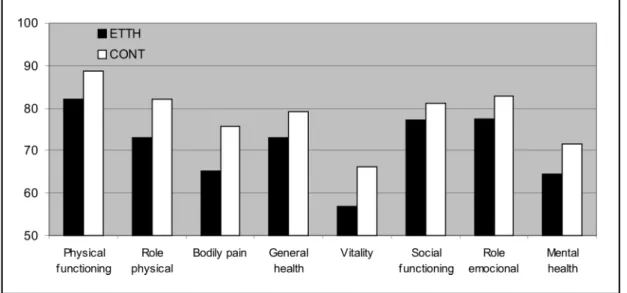
SF-36 scores - Using the Mann - Whitney test for definition of the variables with statistically signif-icant differences, the eight domains by SF-36 were compared between the episodic tension-type hea-dache group and the control (Fig 4).
In the parameters of general health (p = 0.063), mental health (p = 0.114), role physical (p = 0.805),
Fig 1. Distribution of the employees according to level of impact of ETTH on daily activities.
social function (p = 0.20), physical function (p = 0.131), and role emotional (p = 0.221) the groups did not present statistically significant differences. In the domain of vitality (p < 0.0113) and bod-ily pain (p < 0.05) the values obtained by the Epi-sodic Tension-type headache group were signifi-cantly smaller than control.
DISCUSSION
In spite of being is the most common headache disorder, literature concerning the burden of ten-sion-type headache on health - related quality of life is very limited. Prior to 1988, the lack of a pro-per classification system was the main reason to this fact. By that time, no precise and operational de-finition of tension-type headache was available and several imprecise terms were used. The terms mus-cle contraction headache, tension headache, psy-chogenic headache, psychomiogenic headache, es-sential and stress headache had been used inter-changeably2. In the 1988 International Headache
Classification19the tension-type headache (TTH) has
been precisely defined and classified in two forms, the Episodic Tension-Type headache (ETTH) and the Chronic Tension- Type headache (CTTH). Some clin-ical features also contribute to the absence of stu-dies of the effect of ETTH on the HRQoL: the pain is usually mild to moderate in severity, the pain has no prodome or aura and the associated features of migraine, such vomiting, are absent. Besides, ETTH does not usually interfere with daily activities and physical activity normally has no influence on hea-dache intensity1. On the other hand, migraine, which
is associated to a great economic and individual bur-den, is more often seen in clinical settings. Migrai-ne has, understandably, occupied the attention of most investigators.
With respect to frequency of pain, Rasmussen et al.1reported that 23 % of tension-type headache
patients experienced from 8 to14 days per year with pain and 36 % experienced several attacks per month. Lavados and Tenhamm3observed that 32.7%
of the women and 42.2% of the men with ETTH experienced from 2 to 4 episodes per month. Sch-wartz et al.4found that 71.8% of the ETTH suffers
experienced 30 or fewer episodes per year. In Bra-zil, Vincent et al.20found an average frequency of
2.7 episodes of ETTH per month and Bigal9
report-ed that 57.4% of the sample of university students suffer from ETTH experienced from 1 to 5 days with pain a month. So, our results are quite similar to previous publications.
In this study, the impact of ETTH on work effi-ciency was assessed on a 0 to 10 scale and 57% of
Fig 4. Comparison of SF-36 scores between ETTH group and control. Fig 3. Distribution of the employees according to level of
our study subjects reported minimal interference. In the same way, Schwartz et al.4observed that only
8.3% of the ETTH suffers reported lost workdays due to their headaches and Pryse-Phillips et al.5,
in Canada, reported that only 8% of TTH suffers experienced time off paid work because of hea-dache. Lavados and Tenhamm3reported that 86.9%
of the subjects with ETTH frequently experience pain during the work, although 52.3% reported that never or rarely missing work due the pain.
As for the impact of ETTH on leisure, social and family activities, the Canadian study5showed that
18% of the TTH suffers canceled family activities and 26% canceled social activities because of pain. Lavados and Tenhamm3reported that 74.3% of the
individuals with ETTH frequently experienced pain during social or family activities, although 48.8% reported that never or rarely lost such activities be-cause of pain.
Recently, HRQoL measures have been recogni-zed as providing additional data about the impact of several chronic diseases21and the SF-36 is the most
widely used generic instrument for measuring HRQoL. The instrument is translated into numer-ous languages, and the validity of the eight subsca-les is confirmed in general populations and in a wide variety of patient groups in more than two thousands articles. Our sample experienced a signi-ficant impact on the domain vitality of the SF-36. The analysis of this aspect is based on the amount of time in the previous four weeks in which the indi-vidual felt full of energy in contrast with the peri-ods of fatigue or exhaustion. This parameter seem-ingly is extremely affected by the headache12,15,17and
other pain syndromes, such as chronic low back pain22. Osterhaus et al.12reported that the score
ob-tained by the migraineurs in vitality was not only smaller than obtained by the depressed individu-als. Wang et al.23studied 901 patients of a headache
clinic in Taiwan and noted that the vitality domain was highly correlated with symptoms of anxiety and depression evaluated by the Hospital Anxiety and Depression Scale. Holroyd et al.24reported that
chro-nic tension-type headache suffers were 3 to 15 ti-mes more likely than matched controls to receive a diagnosis of an anxiety or mood disorder with al-most half of the patients exhibiting clinically sig-nificant levels of anxiety or depression. Solomon et al.25 observed a significantly higher percentage
of tension-type headache patents with poor health associated with mental health than patients with
migraine. Among Brazilian patients with ETTH, symptoms of anxiety and depression were observed in 60% and 32%, respectively26. Serrano-Duenas27
studied 89 patients with chronic TTH and compa-red their level of depression (on the Hamilton scale) with 31 patients with migraine with typical aura and a control group of 34 asymptomatic volunteers, matched for age, marital and job status. The author observed a similar level of depression between the TTH group (33.7%) and migraine group (32.2%). In order to study the relationship between pri-mary headache syndromes and mood disorders, Mi-tsikostas and Thomas28studied 470 headache
out-patients and 150 age - and sex-matched healthy subjects using a specific questionnaire that includ-ed the Hamilton rating scales for anxiety and de-pression. These authors reported that the average scores for anxiety and depression were significant-ly higher in headache sufferers than in healthy people.
In this study, we examined the impact of ETTH in individuals’ lives and on HRQoL in a sample of em-ployees of a Brazilian public hospital. Even though our sample is not being a general population-ba-sed one, the clinical features and disability patterns reported herein are quite similar to previous pub-lished data. Our study showed that in a sample of ETTH sufferers, pain has reduced HRQoL scores in the domain of vitality compared with controls. It is possible that pain cause an affective distress that could lead to “decreased vitality”. For sure, additio-nal work is required to assess the clinical utility of HRQoL and disability assessment in a large popu-lation of ETTH suffers.
REFERENCES
1. Rasmussen B K, Jensen R, Schroll M, Olesen J. Epidemiology of headache in a general population: a prevalence study. J Clin Epidemiol 1991; 44:1147-1157.
2. Rasmussen BK. Epidemiology of headache. Cephalalgia 1995;15:45-68. 3. Lavados PM, Tenhamm E. Epidemiology of tension-type headache in
Santiago, Chile: a prevalence study. Cephalalgia 1998;18:552-558. 4. Schwartz B S, Stewart W F, Simon J, Lipton R B. Epidemiology of
ten-sion-type headache. JAMA1998;279:381-383.
5. Pryse-Phillips W, Findlay H, Tugwell P, Edmeads J, Murray TJ, Nelson RF. A canadian population survey on the clinical, epidemiologic and social impact of migraine and tension-type headache. Can J Neurol Sci 1992;19:333-339.
6. Roh JK, Kim JS, Ahn YO. Epidemiologic and clinical characteristics of migraine and tension type headache in Korea. Headache 1998;38:356-365. 7. Zivadinov R, Willheim K, Sepic-Grahovac D, et al. Migraine and ten-sion-type headache in Croatia: a population-based survey of precipi-tating factors. Cephalalgia 2003;23:336-343.
8. Köseoglu E, Naçar M, Talaslioglu A, Çetinkaya F. Epidemiological and clinical characteristics of migraine and tension type headache in 1146 females in Kayseri, Turkey. Cephalalgia 2003;23:381-388.
quali-ty of life and performance of a universiquali-ty student population. Headache 2001;41:710-719.
10. Osterhaus J T, Gutterman D L, Plachetka JR. Healthcare resource and lost labour costs of migraine headache in the US. Pharmacoeconomics 1992;2:67-76.
11. Stang P E, Osterhaus J T. Impact of migraine in the United States: data from the National Health Interview Survey. Headache1993;33:29-35. 12. Osterhaus JT, Townsend RJ, Gandek B, Ware JE Jr. Measuring the
func-tional status and well-being of patients with migraine headache. Headache1994;34:337-343.
13. de Lissovoy G, Lazarus SS. The economic cost of migraine: present state of knowledge. Neurology 1994;44(Suppl 4):S56-S62.
14. Lipton RB, Bigal ME, Kolodner K, Stewart WF, Liberman JN, Steiner TJ. The family impact of migraine: population-based studies in the USA and UK. Cephalalgia 2003;23:429-440.
15. Terwindt GM, Ferrari MD, Tijhuis M, Groenen SM, Picavet HSJ, Launer LJ. The impact of migraine on quality of life in the general population. The GEM study. Neurology 2000;55:624-629.
16. Guitera V, Muñoz P, Castillo J, Pascual J. Quality of life in chronic dai-ly headache:a study in general population. Neurology 2002;58:1062-1065. 17. Monzón MJ, Láinez MJ. Quality of life in migraine and chronic daily
headache patients. Cephalalgia 1998;18:638-643.
18. Ciconelli RM, Ferraz MB, Santos W, et al. Brazilian-portuguese version of the SF-36: a reliable and valid quality of life outcome measure. Rev Bras Reumatol 1999;39:143-150.
19. Headache Classification Committee of the International Headache
Society. Classification and diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Cephalalgia 1988;8(Suppl 7):1-96. 20. Vincent M, Rodrigues AJ, Oliveira GV, et al. Prevalence and indirect
costs of headache in a Brazilian company. Arq Neuropsiquiatr 1998;56:734-743.
21. Stewart AL, Greenfield S, Hays RD, et al. Functional status and well-being of patients with chronic conditions: results from the medical outcomes study. JAMA 1989;262:907-913.
22. Gatchel PJ, Mayer T, Dersh J, Robinson R, Polatin P. The association of the SF-36 health status survey with 1-year socioeconomic outcome in a chronically disabled spinal disorder population. Spine 1999;24:2162-2170. 23. Wang SJ, Fuh JL, Lu SR, Juang KD. Quality of life differs among headache diagnoses: analysis of SF-36 survey in 901 headache patients. Pain 2001;89:285-292.
24. Holroyd KA, Stensland M, Lipchik GL, et al. Psychosocial correlates and impact of chronic tension- type headaches. Headache 2000;40:3-16. 25. Solomon GD, Skobieranda FG, Gragg LA . Does quality of life differ
among headache diagnoses? Analysis using the Medical Outcome Study Instrument. Headache 1994;34:143-147.
27. Matta AP G, Moreira PM. Depressive symptoms and anxiety in patients with chronic and episodic tension-type headache. Arq Neuropsiquia-tr 2003;61:991-994.
28. Serrano-Duenas M. Cefalea tipo tensional crônica y depresión. Rev Neurol 2000;30:822-826.