w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Review
article
Hematopoietic
progenitor
cell
mobilization
for
autologous
transplantation
–
a
literature
review
Marco
Aurélio
Salvino
a,∗,
Jefferson
Ruiz
b aUniversidadeFederaldaBahia(UFBA),Salvador,BA,Brazil bSanofi,Brazila
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received17April2015 Accepted17July2015
Availableonline19August2015
Keywords:
Hematopoieticprogenitorcell mobilization
Autologoustransplant Plerixafor
Multiplemyeloma Non-Hodgkinlymphoma
a
b
s
t
r
a
c
t
Theuseofhigh-dosechemotherapywithautologoussupportofhematopoieticprogenitor cellsisaneffectivestrategytotreatvarioushematologicneoplasms,suchasnon-Hodgkin lymphomasandmultiplemyeloma. Mobilizedperipheralblood progenitorcellsare the mainsourceofsupportforautologoustransplants,andcollectionofanadequatenumber ofhematopoieticprogenitorcellsisacriticalstepintheautologoustransplantprocedure. Traditionalstrategies,basedontheuseofgrowthfactorswithorwithoutchemotherapy, havelimitationsevenwhenremobilizationsareperformed.Granulocytecolony-stimulating factoristhemostwidelyusedagentforprogenitorcellmobilization.Theassociationof plerixafor,aC-X-CChemokinereceptortype4(CXCR4)inhibitor,togranulocytecolony stim-ulatingfactorgeneratesrapidmobilizationofhematopoieticprogenitorcells.Aliterature reviewwasperformedofrandomizedstudiescomparingdifferentmobilizationschemes inthetreatmentofmultiplemyelomaandlymphomastoanalyzetheirlimitationsand effectivenessinhematopoieticprogenitorcellmobilizationforautologoustransplant.This analysisshowedthattheadditionofplerixafortogranulocytecolonystimulatingfactoris welltoleratedandresultsinagreaterproportionofpatientswithnon-Hodgkinlymphomas ormultiplemyelomareachingoptimalCD34+cellcollectionswitha smallernumberof
apheresiscomparedtheuseofgranulocytecolonystimulatingfactoralone.
©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
High-dose chemotherapy with autologous hematopoietic stemcelltransplantationisaneffectivestrategytotreat vari-oushematologicneoplasms,suchaschemosensitiverelapsed Hodgkin’slymphomas,1,2 non-Hodgkinlymphomas(NHL)3,4
and multiple myeloma (MM).5 Several clinical guidelines
andconsensusrecommendtheprocedureasstandard treat-ment in these conditions.6–11 According to the Center for
∗ Correspondingauthorat:RuaAugustoViana,s/n,Canela,40110-060Salvador,BA,Brazil.
E-mailaddress:[email protected](M.A.Salvino).
International Blood and Marrow Transplant Research (CIBMTR), 12,047autologoushematopoieticstemcell trans-plantations(AHSCT)werecarriedoutintheUnitedStatesin 2011,withMMandNHLbeingthemainindications.12InBrazil,
datafrom theBrazilianTransplant Registryshowthat1144 AHSCTwereperformedin2013,slightlyhigherthantheyear before.13
http://dx.doi.org/10.1016/j.bjhh.2015.07.011
TheCIBMTRshowsthatperipheralbloodprogenitorcells arethemainsourceusedtosupportautologoustransplants.12
In addition to the possible chemoresistance of the can-cer,mobilizationofhematopoietic progenitorcells(HPC) is anotherpotentiallylimitingstepforAHSCT,withhighfailure rates(between5%and40%)associatedwithhistoricallyused mobilizationstrategies.14
AconsensuspublishedbytheAmericanSocietyforBlood andMarrowTransplantation(ASBMT)recommendscollecting aminimumdoseof2×106CD34+cells/kgtoperformAHSCT,
butthedecisiontoacceptcollectionsofbetween1×106and
2×106CD34+ cells/kgcanbeindividualizedaccordingtothe
circumstancesofeachpatient.Ontheotherhand,largertarget numbersareneededifmultipletransplantsareplanned.15
Although the minimum dose of progenitor cells to be collectediswelldefined,theidealtargetorthedesirable max-imum dose isless clear. Some data show that the use of
≥5×106CD34+cells/kgleadstoquickerandmorepredictable
grafting, achieving platelet transfusions independence sig-nificantly earlier with potential reductions in transplant costs.16,17Thus,adequateprogenitorcellmobilizationisakey
stepwhenplanninganAHSCT.
Biology
related
to
mobilization
of
hematopoietic
progenitor
cells
and
therapeutic
targets
Although mature hematopoietic cells are physiologically releasedfromthebonemarrowtotheperipheralblood, imma-turecellsarefoundinthecirculationataverylowfrequency. About 0.05% or less of the total circulating leukocytes are HPC and express the CD34+ surfacemarker.18 HPC adhere
tothebonemarrowmicroenvironmentbyavarietyof adhe-siveinteractions.19 Furthermore,theyexpressawiderange
ofsurfacereceptors,suchasadhesionmoleculesassociated withangiopoietin-1lymphocytes,verylateantigen4(VLA4), andMac-1,C-X-Cchemokine receptorstype4(CXCR4)and type2(CXCR2), thesurfaceglycoproteins CD44and CD62L, andtyrosinekinasereceptorc-kit.19Thebonemarrowstroma
containsstromalcell-derivedfactor1(SDF-1),CXCchemokine GRO-,vascularcelladhesionmolecule(VCAM-1),KIT-ligand, P-selectin glycoprotein ligand and hyaluronic acid, all of which are ligands for the stem cell adhesion molecules.20
Preclinicaldatashowthatinhibitionofthesereceptor–ligand interactions resultsinincreasedmobilization ofprogenitor cells.19–21
Growth factors [granulocyte colony-stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF)] are the most widely used agents for progeni-tor cell mobilization; they have two main mechanisms of action. The first is the production of proteases by hyper-plasticmyelomonocytic series, which inducesthe cleavage ofSDF-1bypreventingitsbindingtoCXCR4.Themost stud-iedproteaseismatrixmetallopeptidase9(MMP-9),although dipeptidase CD26 seems to have a greater role in this process.22,23 Thesecond mainmechanismisalso
proteoly-sisinduced and isresponsible for degradation ofVCAM-1, osteopontinandfibronectin,leadingtoreducedadhesionof progenitorcellsthroughitsVLA-4receptorinbonemarrow stroma.23
Theadditionofachemotherapeutic agenttoacytokine inthemobilizationregimenhaseffectswhichare notfully elucidated.19Itisspeculatedthattheadditionof
cyclophos-phamide togrowth factors has a synergistic effect on the release ofgranulocyticproteasesinthebonemarrowasits administrationinisolationleadstocleavageofSDF-1,CXCR4 andc-kitadhesionmolecules.19Furthermore,thetoxicityof
chemotherapeuticagentsonbonemarrowstromacanrelease HPCasaresultofdamagetothefunctionalabilityofstromal cellsinsupportingthem.19
Plerixafor(AMD3100)isareversiblybicyclaminhibitorof CXCR4 that breaks the binding betweenSDF-1 and CXCR4 receptors, blocking the chemotactic signaling with stromal cells.23Amongthehypothesesforitsmobilizationmechanism
isthelossofsensitivityofprogenitorcellstoSDF-1caused by the inhibition of CXCR4. Consequently, these cells are attractedtothecirculationthroughsignalingprobablyrelated tosphingosine-1-phosphate(S1P),asphingolipidimplicated inthechemotaxiscontrolofprogenitorcellsfrombone mar-row, blood and other tissues.23 Studies also suggest that
plerixafor keeps the progenitor cells in the circulation by binding to CXCR4,leading toa loss of chemoattraction to SDF-1, decreasing HPC homing, which also contributes to mobilization.24
Mobilization
of
hematopoietic
progenitor
cells
for
multiple
myeloma
and
lymphoma:
results
of
the
historically
most
used
strategies
show
limitations
Traditionally, the most widelyused mobilization strategies have beenthe use ofgrowth factorsalone (G-CSF/GM-CSF) or in combination with chemotherapeutic agents. Among the available growth factors, the most commonly used is recombinant G-CSFfilgrastim, whileothers,suchas, G-CSF pegfilgrastim,G-CSFlenograstimandGM-CSFmolgramostim, areusedlessfrequently.14
G-CSFaloneasfirst-linemobilizationisanattractiveoption owingtothepredictablemobilizationkinetics,whichinturn allows predictable apheresis scheduling and staffing while decreasingcostsofgrowthfactorsandthecollection proce-durecomparedwithcyclophosphamide(CY).25–27
GM-CSFhasbeenshowntobeinferiortoG-CSFinterms ofnumberofstemcellscollectedandinpost-transplantation outcomesrelatedtohematopoieticrecovery,transfusionand antibioticsupport,febrileepisodesandhospitalizations.28,29
Itis mostoftenused inremobilizationstrategies, alone or in combination with other cytokines or chemotherapy.28,29
Data on the use of pegfilgrastimin steady-state mobiliza-tionarebothlimitedandmixed,butonestudydemonstrated predictable mobilization kinetics and similar collection yieldsandapheresis dayscomparedwithaseparate G-CSF cohort.30
CYmaybeincorporatedintotheinitialinductionor sal-vagetherapycycles,ormaybeadministeredasastandalone cycle separatelyfrom standardtherapy. Themostcommon stand-aloneregimensincludecyclophosphamideatarangeof dosesbetween2and7g/m2.CYisassociatedwithhighercell
engraftmentkinetics,35–40 but alsomay resultinmore
tox-icity,febrile neutropenia,transfusions,hospitalizationsand highercosts.14,34,41ThepublishedliteratureonthevariousCY
approachesisvast.Ingeneral,studiesdemonstratethatCY willmobilizemorestemcellsthanG-CSFaloneandhelpin theroleofmobilizingtraditionallydifficultpatients,suchas thosewithlymphoma.42,43
Theprimarygoalofmobilizationistocollectasufficient numberofprogenitorcellsforthepatienttoundergoAHSCT. Theoptimalmobilization,however, requirescollection ofa targetnumberofcellsandalsostrategiestominimizethetime andnumberofapheresis,reducingthecostoftheprocedure andavoidingcomplicationsrelatedtomobilization,suchas hospitalizationduetofebrileneutropenia.15
Asystematicreviewofrandomized clinical trials evalu-atedtheresultsof28studiescomparingdifferentmobilization schemes. Eighteen included onlypatients with MMand/or lymphomas14 and only four of these were multicenter. Table1showsthecharacteristicsofinterventionsandresults observedinstudies includedinthissystematicreviewthat recruited≥10patientsineacharmand compareddifferent regimensofgrowthfactorswithandwithoutchemotherapy (Table1).
Thesestudiesshowthat,ingeneral,strategieswithhigher dosesofG-CSFaloneorchemotherapywiththeadditionof growth factors (G-CSF and/or GM-CSF) result in increased numberofCD34+ cellscollected.Furthermore,some
strate-giesreducedthenumberofapheresisneededtoachievetarget collection.14
Althoughthissystematicreviewhaslimitations suchas restrictedsamplesizeofstudies,theirmoderatequalityand variabilityinthepopulation,itdemonstratesthelimitations oftechniqueshistoricallyusedinHPCmobilization.Amajor retrospective analysis, involving 2177 patients undergoing attemptedmobilizationinthreeItaliancentersbetween1999 and2007,showedarateofpoormobilizers(definedasa collec-tionof<2×106CD34+cells/kg)ofonly15%corroboratingdata
fromrandomizedtrials.44
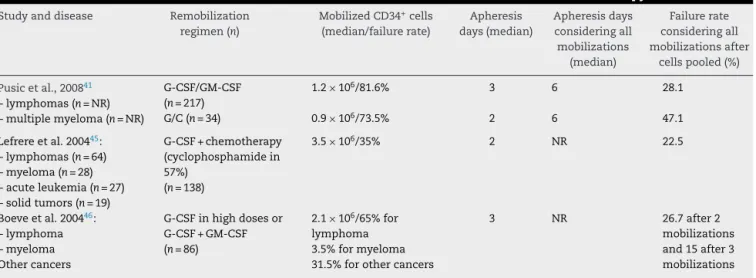
Insufficientinitialmobilizationleadstonewmobilization procedures(remobilization),whichcannegativelyinfluence disease progression and significantly increase the use of resources.41Severalstudiesevaluatedthesuccessof
remobi-lizationwithtraditionalmeasuresbasedontheuseofgrowth factors.Aretrospectiveanalysisassessedtheresultsof remo-bilizationofregimenscontainingG-CSFand/orGM-CSF,alone orcombined withchemotherapyin251 patientswith lym-phomaorMM.41Afterremobilization,only18.4%ofpatients
whousedG-CSForGM-CSFand26.5%ofthosewhoreceiveda growthfactorassociatedwithchemotherapyachieved collec-tionsof≥2×106CD34+ cells/kg.Whencellscollected inthe
firstmobilization werepooled, thefailurerates were28.1% inthegroupremobilizedwithgrowthfactoraloneand47.1% inthegroupremobilizedwithgrowthfactorassociatedwith chemotherapy(Table2).41
Publisheddatasuggestthat,althoughremobilizationwith growthfactorscanrescuepatientswhofailedthefirst mobi-lization,theproportionofpatientsnotmeetingtheminimum collectionofHPCrequiredtoperformAHSCTishigh(around 30%),confirmingtheneedtoevaluatemoreeffective mobiliza-tionstrategies.
Challenges
for
the
identification
and
prospective
characterization
of
poor
mobilizers
after
strategies
based
on
the
use
of
growth
factors
The possibility ofpredicting mobilization failure based on patient’s characteristicsintheearlymobilizationprocessis highlydebatable.15Eachstudyproposesdifferentdefinitions
ofpoormobilizers,limitingtheuniformityofthe characteris-ticsthatprospectivelyidentifythesepatients.18
Someidentifiablecharacteristicsbeforemobilizationhave often been associated with a higher risk of failure of procedures inpatients withlymphoproliferativediseases.29
Althoughsomeofthesefactorsareunanimouslypointedout inthe literatureaspredictiveofpoormobilization,suchas theintensityofpriorexposuretochemotherapyorradiation, theuseofchemotherapeuticagentsandfailureinaprevious attemptofmobilizationothers,suchaspatientage,havea morecontroversialrelationshipwithpoormobilization.47
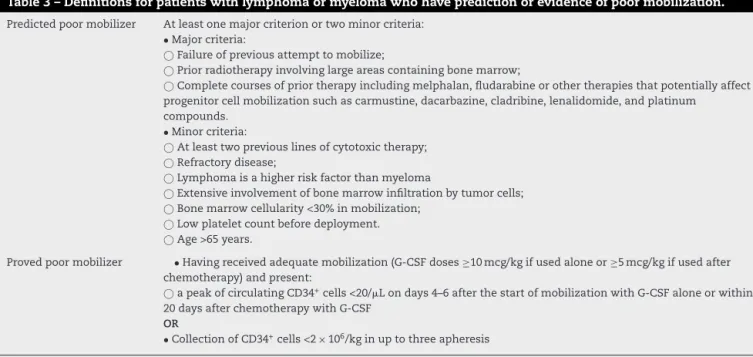
The Italian working group, Gruppo Italiano Trapianto di MidolloOsseo(GITMO),recentlyproposedadefinitionfor‘poor mobilizers’forpatientswithlymphomaormyeloma.48This
definitioncamefromaconsensusofexpertsand considers thefactorsdescribedinTable3.
Theconcept ofproved poormobilizer basedon the cir-culating CD34+ cell countafter 4–6 daysofmobilization is
very relevantgiventhe availabilityofpreemptivestrategies withpotentialforreducingriskofcomplicationsrelatedtothe necessityofagreaternumberofapheresisorhigherneedfor remobilizationsandpossiblereducedcost.
Use
of
plerixafor
to
mobilize
hematopoietic
progenitor
cells:
randomized
clinical
trials
showing
its
effectiveness
Plerixaforhasprovedtobeanagentthatgeneratesrapid mobi-lizationofHPCinmurinemodelsandsubsequentlyinhealthy humanvolunteers.49ThephaseIandIIstudiesattestedthe
mobilizing effect and safety of the G-CSF plus plerixafor combination inpatients withNHL and MM. Therapidand significantincreaseinwhitebloodandCD34+cellcountsin
peripheralblood,includedpatientswhosefailuretomobilize withG-CSFalonewasproven.49–51Thecombination
guaran-teedcollectionsof≥2×106CD34+cells/kgin95.9%ofpatients
with77.6% achievingacollectionof≥5×106CD34+ cells/kg
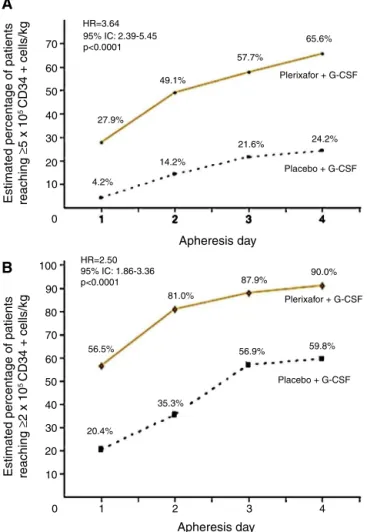
(22.4%ofpatientsachievedthisdoseafteronlyoneapheresis). Tworandomized,comparative,double-blind,placebo con-trolled and prospective multicenter studies evaluated the use ofG-CSFplusplerixafor versusG-CSF aloneinthe ini-tialmobilizationstrategyofpatients.Thesestudiesrecruited 298 patientswithNHL52 and 302patients withMM.53 NHL
patientstreatedwiththecombinedtherapyobtained65.6% of successful collections of ≥5×106CD34+ cells/kg versus
24.2%intheG-CSFarm.Collectionof≥2×106CD34+cells/kg
wasachievedby90%withthecombinationagainst59.8%in theG-CSFgroupwithinfourapheresisdays(p-value<0.001) (Figure1).ThemediannumberofCD34+ cellscollectedwas
Table1–Randomizedclinicaltrialsevaluatingdifferentmobilizationstrategiesincludinggrowthfactorswith/without chemotherapy.14
Study Interventions(n) Collected
CD34+cells
(median/×106)
Numberof apheresis
(median)
Patients failedto mobilize(%)
Cyclophosphamideassociatedwithgrowthfactor
Faconetal.,1999 CY4g/m2+filgrastim5mcg/kg/d+ancestim
20mcg/kg/d(n=55)
12.4a 1a 14.5
CY4g/m2+filgrastim5mcg/kg/d(n=47) 8.2 2 19.1
Gazittetal.2000 CY3g/m2+molgramostim250mcg/m2(n=10) NR 2 40.0
CY3g/m2+filgrastim10mcg/kg/d(n=13) NR 3 23.0
CY3g/m2+molgramostim250mcg/m2+filgrastim
10mcg/kg/d(n=12)
NR 1 41.7
Narayanasamietal.2001 Filgrastim10mcg/kg/d(n=23) 2.5 Nodifference NR CY5g/m2+filgrastim10mcg/kg/d(n=24) 7.2* Nodifference NR
Pavoneetal.2002 DHAP+filgrastim5mcg/kg/d(n=38) 5.9 2 13.2 CY+filgrastim5mcg/kg/d(n=34) 7.1 2 11.8 Vela-Ojedaetal.2000 IFO+molgramostim5mcg/kg/d(n=28) 3.1 3 14.3 CY4g/m2+molgramostim5mcg/kg/d(n=28) 5.3 3 10.7
Growthfactoralone
Stiffetal.2000 Filgrastim10mcg/kg/d(n=51) 3.6 NR 26.0 Filgrastim10mcg/kg/d+ancestim20mcg/kg/d(n=56) 2.4 NR 16.4
Otherchemotherapycombinationsassociatedwithgrowthfactors
Copelanetal.2009 R+VP-16+filgrastim10mcg/kg/d(n=28) 9.9* 3 3.6
VP-16+filgrastim10mcg/kg/d(n=27) 5.6 4 14.8 Hartetal.2009 IEE+filgrastim5mcg/kgb.i.d+EPO(n=14) 15.4 1.3 0
IEE+filgrastim5mcg/kgb.i.d(n=12) 12.6 1.8 16.7 Ozceliketal.2009 CE+filgrastim10mcg/kg/d(late)(n=23) 10.8 1 13.0 CE+filgrastim10mcg/kg/d(early)(n=25) 10.5 1 16.0
CY:cyclophosphamide;IFO:ifosfamide;DHAP:dexamethasone+cytarabine+cisplatin;IEE:ifosfamide+epirubicin+etoposide;EPO: erythro-poietin;CE:cyclophosphamide+etoposide;NR:notreported.
a Statisticallysignificantdifference.
1.98×106cells/kg).52Incidenceofadverseevents,mostlymild
tomoderate,wassimilarbetweengroupswithonly5.3%of seriouseventsinthecombinationgroupand6.9%intheG-CSF groupduringthemobilization period.52Themostcommon
non-seriousadverseeventswerediarrhea(38%),injectionsite erythema(29.3%),nausea(17.3%),headache(11.3%)andbone pain(10.7%),allofwhichwereeasilymanageable.52
MMpatientstreatedwithG-CSFplusplerixaforobtained
≥6×106CD34+cells/kgwithintwoapheresisdays,with86.8%
achievingthistargetversus55.9%intheG-CSFgroup(p-value <0.0001).Thecombinationwasalsomoreeffectivetocollect
≥6×106CD34+cells/kgwithinfourapheresisdays(75.7%vs.
51.3%;p-value<0.001)and≥2×106CD34+cells/kgdays(95.3%
vs.88.3%;p-value=0.031)36(Figure2).Themediannumberof
Table2–ResultsobtainedwithremobilizationwithG-CSFand/orGM-CSFwithorwithoutchemotherapy.
Studyanddisease Remobilization regimen(n)
MobilizedCD34+cells
(median/failurerate)
Apheresis days(median)
Apheresisdays consideringall mobilizations
(median)
Failurerate consideringall mobilizationsafter
cellspooled(%)
Pusicetal.,200841
–lymphomas(n=NR) –multiplemyeloma(n=NR)
G-CSF/GM-CSF (n=217)
1.2×106/81.6% 3 6 28.1
G/C(n=34) 0.9×106/73.5% 2 6 47.1
Lefrereetal.200445:
–lymphomas(n=64) –myeloma(n=28) –acuteleukemia(n=27) –solidtumors(n=19)
G-CSF+chemotherapy (cyclophosphamidein 57%)
(n=138)
3.5×106/35% 2 NR 22.5
Boeveetal.200446:
–lymphoma –myeloma Othercancers
G-CSFinhighdosesor G-CSF+GM-CSF (n=86)
2.1×106/65%for
lymphoma 3.5%formyeloma 31.5%forothercancers
3 NR 26.7after2 mobilizations and15after3 mobilizations
Table3–Definitionsforpatientswithlymphomaormyelomawhohavepredictionorevidenceofpoormobilization. Predictedpoormobilizer Atleastonemajorcriterionortwominorcriteria:
•Majorcriteria:
Failureofpreviousattempttomobilize;
Priorradiotherapyinvolvinglargeareascontainingbonemarrow;
Completecoursesofpriortherapyincludingmelphalan,fludarabineorothertherapiesthatpotentiallyaffect progenitorcellmobilizationsuchascarmustine,dacarbazine,cladribine,lenalidomide,andplatinum
compounds.
•Minorcriteria:
Atleasttwopreviouslinesofcytotoxictherapy;
Refractorydisease;
Lymphomaisahigherriskfactorthanmyeloma
Extensiveinvolvementofbonemarrowinfiltrationbytumorcells;
Bonemarrowcellularity<30%inmobilization;
Lowplateletcountbeforedeployment.
Age>65years.
Provedpoormobilizer •Havingreceivedadequatemobilization(G-CSFdoses≥10mcg/kgifusedaloneor≥5mcg/kgifusedafter chemotherapy)andpresent:
apeakofcirculatingCD34+cells<20/Londays4–6afterthestartofmobilizationwithG-CSFaloneorwithin
20daysafterchemotherapywithG-CSF
OR
•CollectionofCD34+cells<2×106/kginuptothreeapheresis
AdaptedbyJantunenetal.47andGruppoItalianoTrapiantodiMidolloOsseo.48
CD34+cellscollectedwasalsohigherinthecombinationgroup
(12.97vs.7.31×106cells/kg).Theincidenceofadverseevents
wassimilarbetweenstudygroups.Themostcommon non-seriousadverseeventsoccurredwereinjectionsiteerythema (20.4%),diarrhea(18.4%),nausea(16.3%),bonepain(9.5%)and fatigue (8.2%), all ofwhich were easily manageable.53 The
majorityoftheseeventsoccurred intheperiodafter mobi-lizationandwereunrelatedtothestudydrug.53
Thesestudiesshowthatthecombinationofplerixaforwith G-CSF iswell tolerated and resultsin agreater proportion ofNHLorMMpatientsachievingCD34+ cellcollections
con-sideredoptimal fortransplant withinasmaller number of apheresisdayswhencomparedwithG-CSFalone.
Strategies
for
preemptive
use
of
plerixafor
Manystudies,including phaseIIIstudies,haveshownthat theuseofplerixaforreducesriskofpoorprogenitorcell mobi-lizationandriskoffailurefromupto40%tolessthan10%. However,thecostofplerixaformaybealimitingfactorforits unrestricteduseintheinitialmobilization.54
An alternative strategy discusses the use of plerixafor as rescue treatment in patients failing prior mobilization. Micallefetal.analyzed52patientswithNHLwhofailedthe ini-tialmobilizationwithG-CSFinaphaseIIIstudy.Theanalysis showedthatpatientswhoreceivedremobilizationwithG-CSF associatedwithplerixaforpresentedamediancollectionof 2.9×106CD34+ cells/kg inremobilizationaftera medianof
threeapheresis.55 Inthis study,63.5% ofpatients achieved
acollectionof≥2×106CD34+ cells/kg inuptofour
aphere-sisdaysinthesecondmobilizationand88.75%wereableto undergothetransplant.
Somecentersdevelopedalgorithmsforthepreemptiveuse ofplerixaforinwhichpatientsinitiallyreceivecustomary regi-mensformobilization.Inthiscase,plerixaforisindicated,if
necessary,toimmediatelyrescuepatientswithverifiedpoor mobilizationbeforecollectionofprogenitorcells.17,56
Onestudyevaluated314patientswithmyeloma, amyloid-osisorlymphomaundergoingmobilizationwithG-CSF and testedtwoalgorithmsforplerixaforuse.Oneusedplerixafor onlyinpatientswithaCD34+cellcountinperipheralblood
of<10/LonDay4ofmobilizationoronanydayof aphere-sis,withcollectionsof<0.5×106CD34+ cells/kg(plerixafor-1
algorithm –including 216patients). Theother used plerix-afor ifCD34+ cellcountinperipheralblood reached<10/L
onDay4ofmobilization(<20/Lifmultipletransplantswere planned) or if collection was <1.5×106CD34+ cells/kg on
Day 1ofapheresis or <0.5×106CD34+ cells/kg inany
sub-sequentapheresisday(plerixafor-2algorithm–including98 patients). The target was the collection of ≥4×106CD34+
cells/kg (optimalcollection)or≥2×106CD34+ cells/kg
(min-imum collection). The results were compared with those obtainedinanothercohortof278patientsmobilizedbefore theintroductionofplerixafor,andwithdatafromthesame prospectivedatabaseoftransplant(MayoClinic),presenting similarcharacteristics.57 Someotherstudiesevaluating
dif-ferentalgorithmsforthepreemptiveuseofplerixaforshowed lowercollectingfailureratesof0–7%.57,58
A reviewofpharmacoeconomicstudiespresentedsome algorithmsforthepreemptiveuseofplerixaforthatresulted inreducedconsumptionofseveralhealthresources, includ-ingthepossibilityofreducingthetotalcostofmobilization procedures.54
Cost
effective
analyses
Therearesomeanalysesrelatedtoplerixaforcost–benefitin frontlineandinremobilizationscenarios,56,59–62buttheywere
HR=3.64 95% IC: 2.39-5.45 p<0.0001
49.1%
57.7%
65.6%
Plerixafor + G-CSF
24.2% 21.6%
Placebo + G-CSF 14.2%
4.2% 27.9%
70
60
50
40
30
20
10
0
100
90
80
70
60
50
40
30
20
10
0 1 2 3 4
1 2 3 4
Apheresis day
Apheresis day
20.4%
35.3%
56.9% 59.8%
Placebo + G-CSF Plerixafor + G-CSF
90.0% 87.9%
81.0%
56.5% HR=2.50 95% IC: 1.86-3.36 p<0.0001
Estimated percentage of patients reaching
≥
5 x 10
5 CD34 + cells/kg
Estimated percentage of patients reaching
≥
2 x 10
5 CD34 + cells/kg
A
B
Figure1–Percentageofpatientswithnon-Hodgkin
lymphomaachievingcollectiontargetsof≥5×106CD34+
cells/kg(A)andof≥2×106CD34+cells/kg(B)after
mobilizationwithG-CSFplusplaceboorG-CSFplus
plerixafor.
AdaptedfromDiPersioetal.52
HR=2.54 p<0.001
77.9%
86.8% 86.8%
55.9% 48.9%
35.3%
17.3% 54.2%
Plerixafor + G-CSF Placebo + G-CSF
5 4
3 2
1 1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Days
Percentage reaching target
Figure2–Percentageofpatientswithmultiplemyeloma
achievingcollectiontargetsof≥6×106CD34+cells/kgafter
mobilizationwithG-CSFplusplaceboorG-CSFplus
plerixafor.
AdaptedfromDiPersioetal.53
Table4–Costanalysis.
Baseline Plerixafor-1 Plerixafor-2 pvalue
Patients 280 219 98
Totalcostperpatienta
Median $12,500 $12,500 $20,000 Minimum $3000 $5000 $5500
Maximum $146,750 $93,000 $89,750 0.01 Mean $17,150 $21,532 $20,617
AdaptedfromMicaleffetal.56
a Costanalysisincludesremobilizationcostsandhasbeenadded
totheoriginalmobilizationregardlessofwhentheremobilization occurred.
these analysesis thatthe calculated costs didnotinclude supportivecarecosts,includingtransfusions,antimicrobials, hospitalization,cryopreservation,nursingandmedicalcosts, patient’spersonalcosts,logistics,orevencostswithprevious failures,remobilization56,59–62and,specifically,theworse
out-comeinlymphomaandmyelomapatientsfailuretoundergo AHSCT.41,63,64,65
InthestudyofMicallefetal.,56althoughtheearlier
identi-ficationofpoormobilizersandadditionofplerixaforresults in higher per-patient costs over baseline, it is associated withhigherapheresisyields,fewerdaysofmobilizationand collection, and lower failure rates. The median total costs of mobilization per patient, including any remobilization attempt,wasUS$12,500inthebaselinegroup,US$12,500in theplerixafor-1group,andUS$20,000intheplerixafor-2group (Table 4). Althoughboth the medianand mean costswere higherintheplerixafor-2group,themobilizationfailurerate was1%,withfewerdaysofapheresis,fewerdaysofplerixafor, andfewertotaldaysofmobilizationandcollectioncompared totheplerixafor-1algorithm.56Thereisanurgencytohave
moreaccuratepharmacoeconomicmatrixestocalculatethe otherimportantandneglectedcostsmentionedaboveandto decideabouttherealcost–benefitineachinstitution.
Consensus recommendations suggest the use of plerix-aforasamobilizationstrategyparticularlyinpatientswitha highertargetforcollectionofprogenitorcells,asapreemptive approachbasedonthemonitoringoftheCD34+cellcountand
incasesofremobilization.15 TheEuropeanGroupforBlood
Apheresis (target cell count = 2.0 Mio CD34+ cells/kg BW)+
Pre-emptive plerixafor <10 cells/μL CD34+ cell count prior to apheresis
10-20 cells/μL >20 cells/μL∗
Dynamic approach based on the patient’s disease characteristics and
treatment history
Figure3–EuropeanGroupforBloodandMarrow
Transplantationpositionregardingmobilization.
andMarrowTransplantation(EGBMT)recommends preemp-tiveuseofplerixaforinpatientswithCD34+cellcounts<10/L
beforeapheresis31(Figure3).Eachcentershoulddevelopand
implementitsownalgorithmsforapplyingdifferent mobiliza-tionstrategies,withthegoalofoptimizingcollectionyields andcosts–benefits.
Conclusion
Collectionofadequate numbersofHPCisacritical stepin autologoustransplantationprocedures.Traditionalstrategies, basedontheuseofgrowthfactorswithorwithout chemother-apy, havesome limitations even whenremobilizations are performed.
Theadditionofplerixaforshowsaconsistentincreasein collectionratesuccess,reducingthenumberofapheresisand notincreasingtoxicity.Strategiesofpreemptiveuseof plerix-aforhavebeenconsideredapromisingwaytooptimizeand rationalizethe useofthisagentinpatientswhohavehigh chanceoffailurewithclassic mobilizationbased onG-CSF withor withoutchemotherapy. Thisstrategywould reduce failureinmobilization,especiallyinpoormobilizers,ensuring collectionandtransplantationaswellasreducingtimeand costsofthemobilizationprocedure.However,external valid-ityofthesealgorithmsislimited,soitisrecommendedthat eachinstitutionsetsupastrategyappropriatetoitsstandards forthepreemptiveuseofplerixafor.
Funding
PublicationsupportprovidedbySanofi.
Conflicts
of
interest
Dr.MarcoAurelioSalvinoreceives consultingand speaking fees.HeismemberofSanofiHematologyAdvisoryBoard.
Dr.JeffersonRuizworksashematology/oncologyscientific advisorforSanofi,Brazil.
r
e
f
e
r
e
n
c
e
s
1. LinchDC,WinfieldD,GoldstoneAH,MoirD,HancockB, McMillanA,etal.Doseintensificationwithautologous bone-marrowtransplantationinrelapsedandresistant Hodgkin’sdisease:resultsofaBNLIrandomisedtrial.Lancet. 1993;341(8852):1051–4.
2. SchmitzN,PfistnerB,SextroM,SieberM,CarellaAM,Haenel M,etal.Aggressiveconventionalchemotherapycompared withhigh-dosechemotherapywithautologoushaemopoietic stem-celltransplantationforrelapsedchemosensitive Hodgkin’sdisease:arandomisedtrial.Lancet. 2002;359(9323):2065–71.
3. PhilipT,GuglielmiC,HagenbeekA,SomersR,VanderLelieH, BronD,etal.Autologousbonemarrowtransplantationas comparedwithsalvagechemotherapyinrelapsesof chemotherapy-sensitivenon-Hodgkin’slymphoma.NEnglJ Med.1995;333(23):1540–5.
4. SchoutenHC,QianW,KvaloyS,PorcelliniA,HagbergH, JohnsenHE,etal.High-dosetherapyimproves
progression-freesurvivalandsurvivalinrelapsedfollicular non-Hodgkin’slymphoma:resultsfromtherandomized EuropeanCUPtrial.JClinOncol.2003;21(21):
3918–27.
5.KorethJ,CutlerCS,DjulbegovicB,BehlR,SchlossmanRL, MunshiNC,etal.High-dosetherapywithsingleautologous transplantationversuschemotherapyfornewlydiagnosed multiplemyeloma:asystematicreviewandmeta-analysisof randomizedcontrolledtrials.BiolBloodMarrowTransplant. 2007;13(2):183–96.
6.LjungmanP,BregniM,BruneM,CornelissenJ,deWitteT,Dini G,etal.Allogeneicandautologoustransplantationfor haematologicaldiseases,solidtumoursandimmune disorders:currentpracticeinEurope2009.BoneMarrow Transplant.2010;45(2):219–34.
7.HoppeRT,AdvaniRH,AiWZ,AmbinderRF,AounP,BelloCM, etal.Hodgkinlymphoma,version2.2012featuredupdatesto theNCCNguidelines.JNatlComprCancNetw.
2012;10(5):589–97.
8.ZelenetzAD,GordonLI,WierdaWG,AbramsonJS,AdvaniRH, AndreadisCB,etal.Non-Hodgkin’sLymphomas,Version 4.2014.JNatlComprCancNetw.2014;12(9):
1282–303.
9.AndersonKC,AlsinaM,BensingerW,BiermannJS,CohenAD, DevineS,etal.Multiplemyeloma,version1.2013.JNatl ComprCancNetw.2013;11(1):11–7.
10.HahnT,WingardJR,AndersonKC,BensingerWI,BerensonJR, BrozeitG,etal.Theroleofcytotoxictherapywith
hematopoieticstemcelltransplantationinthetherapyof multiplemyeloma:anevidence-basedreview.BiolBlood MarrowTransplant.2003;9(1):4–37.
11.OlianskyDM,GordonLI,KingJ,LaportG,LeonardJP, McLaughlinP,etal.Theroleofcytotoxictherapywith hematopoieticstemcelltransplantationinthetreatmentof follicularlymphoma:anevidence-basedreview.BiolBlood MarrowTransplant.2010;16(4):443–68.
12.CIBMTR,CenterforInternationalBloodandMarrow TransplantResearch.SummarySlides2014(PowerPoint); 2014.Availablefrom:http://www.cibmtr.org/ReferenceCenter/ SlidesReports/SummarySlides/pages/index.aspx[cited 28.06.15].
13.RegistroBrasileirodeTransplantes:Dimensionamentodos transplantesnoBrasileemcadaestado(2006–2013).São Paulo;2013.Availablefrom:http://www.abto.org.br/abtov03/ Upload/file/RBT/2013/rbt2013-parcial(1).pdf[cited28.06.15]. 14.SheppardD,BredesonC,AllanD,TayJ.Systematicreviewof
randomizedcontrolledtrialsofhematopoieticstemcell mobilizationstrategiesforautologoustransplantationfor hematologicmalignancies.BiolBloodMarrowTransplant. 2012;18(8):1191–203.
15.GiraltS,CostaL,SchriberJ,DipersioJ,MaziarzR,McCartyJ, etal.Optimizingautologousstemcellmobilizationstrategies toimprovepatientoutcomes:consensusguidelinesand recommendations.BiolBloodMarrowTransplant. 2014;20(3):295–308.
16.SienaS,SchiavoR,PedrazzoliP,Carlo-StellaC.Therapeutic relevanceofCD34celldoseinbloodcelltransplantationfor cancertherapy.JClinOncol.2000;18(6):1360–77.
17.LimatS,Woronoff-LemsiMC,DeconinckE,RacadotE,Jacquet M,HerveP,etal.Cost-effectivenessofCD34+dosein peripheralbloodprogenitorcelltransplantationfor non-Hodgkin’slymphomapatients:asinglecentrestudy. BoneMarrowTransplant.2000;25(9):997–1002.
18.MohtyM,HoAD.Inandoutoftheniche:perspectivesin mobilizationofhematopoieticstemcells.ExpHematol. 2011;39(7):723–9.
20.BonigH,PapayannopoulouT.Mobilizationofhematopoietic stem/progenitorcells:generalprinciplesandmolecular mechanisms.MethodsMolBiol.2012;904:1–14.
21.ToLB,HaylockDN,SimmonsPJ,JuttnerCA.Thebiologyand clinicalusesofbloodstemcells.Blood.1997;89(7):2233–58.
22.AlvarezP,CarrilloE,VelezC,Hita-ContrerasF,Martinez-Amat A,Rodriguez-SerranoF,etal.Regulatorysystemsinbone marrowforhematopoieticstem/progenitorcellsmobilization andhoming.BiomedResInt.2013;2013:312656.
23.AngelopoulouMK,TsirkinidisP,BoutsikasG,Vassilakopoulos TP,TsirigotisP.Newinsightsinthemobilizationof
hematopoieticstemcellsinlymphomaandmultiple myelomapatients.BiomedResInt.2014;2014:835138.
24.BonigH,PapayannopoulouT.Hematopoieticstemcell mobilization:updatedconceptualrenditions.Leukemia. 2013;27(1):24–31.
25.ChaoNJ,GrimaDT,CarrumG,HolmbergL,FungHC,BrownS, etal.Chemo-mobilizationprovidessuperiormobilizationand collectioninautologousstemcelltransplantsbutwithless predictabilityandatahighercost.Blood(ASHAnnual MeetingAbstracts).2011;118:4048.
26.DesikanKR,BarlogieB,JagannathS,VesoleDH,SiegelD, FassasA,etal.Comparableengraftmentkineticsfollowing peripheral-bloodstem-cellinfusionmobilizedwith granulocytecolony-stimulatingfactorwithorwithout cyclophosphamideinmultiplemyeloma.JClinOncol. 1998;16(4):1547–53.
27.HoggattJ,PelusLM.Hematopoieticstemcellmobilization withagentsotherthanG-CSF.MethodsMolBiol.
2012;904:49–67.
28.WeaverCH,SchulmanKA,Wilson-RelyeaB,BirchR,WestW, BucknerCD.Randomizedtrialoffilgrastim,sargramostim,or sequentialsargramostimandfilgrastimafter
myelosuppressivechemotherapyfortheharvestingof peripheral-bloodstemcells.JClinOncol.2000;18(1):43–53.
29.AroraM,BurnsLJ,BarkerJN,MillerJS,DeforTE,Olujohungbe AB,etal.Randomizedcomparisonofgranulocyte
colony-stimulatingfactorversusgranulocytemacrophage colony-stimulatingfactorplusintensivechemotherapyfor peripheralbloodstemcellmobilizationandautologous transplantationinmultiplemyeloma.BiolBloodMarrow Transplant.2004;10(6):395–404.
30.HosingC,QazilbashMH,KebriaeiP,GiraltS,DavisMS,Popat U,etal.Fixed-dosesingleagentpegfilgrastimforperipheral bloodprogenitorcellmobilisationinpatientswithmultiple myeloma.BrJHaematol.2006;133(5):533–7.
31.MohtyM,HubelK,KrogerN,AljurfM,ApperleyJ,BasakGW, etal.Autologoushaematopoieticstemcellmobilisationin multiplemyelomaandlymphomapatients:aposition statementfromtheEuropeanGroupforBloodandMarrow Transplantation.BoneMarrowTransplant.2014;49(7): 865–72.
32.AlegreA,TomásJF,Martínez-ChamorroC,Gil-FernándezJJ, Fernández-VillaltaMJ,ArranzR,etal.Comparisonof peripheralbloodprogenitorcellmobilizationinpatientswith multiplemyeloma:high-dosecyclophosphamideplus GM-CSFvsG-CSFalone.BoneMarrowTransplant. 1997;20(3):211–7.
33.DesikanKR,TricotG,MunshiNC,AnaissieE,SpoonD,Fassas A,etal.Precedingchemotherapy,tumourloadandage influenceengraftmentinmultiplemyelomapatients mobilizedwithgranulocytecolony-stimulatingfactoralone. BrJHaematol.2001;112(1):242–7.
34.DingliD,NowakowskiGS,DispenzieriA,LacyMQ,HaymanS, LitzowMR,etal.Cyclophosphamidemobilizationdoesnot improveoutcomeinpatientsreceivingstemcell
transplantationformultiplemyeloma.ClinLymphoma Myeloma.2006;6(5):384–8.
35.NarayanasamiU,KantetiR,MorelliJ,KlekarA,Al-OlamaA, KeatingC,etal.Randomizedtrialoffilgrastimversus chemotherapyandfilgrastimmobilizationofhematopoietic progenitorcellsforrescueinautologoustransplantation. Blood.2001;98(7):2059–64.
36.DazziC,CarielloA,RostiG,ArgnaniM,SebastianiL,FerrariE, etal.IsthereanydifferenceinPBPCmobilizationbetween cyclophosphamideplusG-CSFandG-CSFaloneinpatients withnon-Hodgkin’slymphoma?LeukLymphoma. 2000;39(3/4):301–10.
37.GlaspyJA.Economicconsiderationsintheuseofperipheral bloodprogenitorcellstosupporthigh-dosechemotherapy. BoneMarrowTransplant.1999;23Suppl.2:S21–7.
38.HiwaseDK,BollardG,HiwaseS,BaileyM,MuirheadJ, SchwarerAP.Intermediate-doseCYandGCSFmoreefficiently mobilizeadequatenumbersofPBSCfortandemautologous PBSCtransplantationcomparedwithlow-doseCYinpatients withmultiplemyeloma.Cytotherapy.2007;9(6):539–47.
39.HamadaniM,KochuparambilST,OsmanS,CumpstonA, LeadmonS,BunnerP,etal.Intermediate-doseversus low-dosecyclophosphamideandgranulocytecolony stimulatingfactorforperipheralbloodstemcellmobilization inpatientswithmultiplemyelomatreatedwithnovel inductiontherapies.BiolBloodMarrowTransplant. 2012;18(7):1128–35.
40.SizemoreCA,LaporteJ,HollandHK,MccollumJ,WestermanJ, MorrisLE,etal.Acomparisonoftoxicityandmobilization efficacyfollowingtwodifferentdosesofcyclophosphamide formobilizationofhematopoieticstemcellsin
non-Hodgkin’slymphomapatients.BiolBloodMarrow Transplant.2010;16Suppl.2:S206.
41.PusicI,JiangSY,LanduaS,UyGL,RettigMP,CashenAF,etal. Impactofmobilizationandremobilizationstrategieson achievingsufficientstemcellyieldsforautologous transplantation.BiolBloodMarrowTransplant. 2008;14(9):1045–56.
42.DamonLE,JohnsonJL,NiedzwieckiD,ChesonBD,HurdDD, BartlettNL,etal.Immunochemotherapyandautologous stem-celltransplantationforuntreatedpatientswith mantle-celllymphoma:CALGB59909.JClinOncol. 2009;27(36):6101–8.
43.GeislerCH,KolstadA,LaurellA,AndersenNS,PedersenLB, JerkemanM,etal.Long-termprogression-freesurvivalof mantlecelllymphomaafterintensivefront-line
immunochemotherapywithinvivoepurgedstemcellrescue: anonrandomizedphase2multicenterstudybytheNordic LymphomaGroup.Blood.2008;112(7):2687–93.
44.PerseghinP,TerruzziE,DassiM,BaldiniV,ParmaM,Coluccia P,etal.Managementofpoorperipheralbloodstemcell mobilization:incidence,predictivefactors,alternative strategiesandoutcome.Aretrospectiveanalysison2177 patientsfromthreemajorItalianinstitutions.TransfusApher Sci.2009;41(1):33–7.
45.LefrereF,LevyV,MakkeJ,AudatF,Cavazzana-CalvoM,Miclea JM.Successfulperipheralbloodstemcellharvestingwith granulocytecolony-stimulatingfactoraloneafterprevious mobilizationfailure.Haematologica.2004;89(12):1532–4.
46.BoeveS,StrupeckJ,CreechS,StiffPJ.Analysisof
remobilizationsuccessinpatientsundergoingautologous stemcelltransplantswhofailaninitialmobilization:risk factors,cytokineuseandcost.BoneMarrowTransplant. 2004;33(10):997–1003.
47.JantunenE,KvalheimG.Mobilizationstrategiesin
hard-to-mobilizepatientswithlymphoidmalignancies.EurJ Haematol.2010;85(6):463–71.
hocworkinggroupGruppoItalianoTrapiantodiMidollo Osseo.BoneMarrowTransplant.2012;47(3):342–51.
49.StiffP,MicallefI,McCarthyP,Magalhaes-SilvermanM, WeisdorfD,TerritoM,etal.Treatmentwithplerixaforin non-Hodgkin’slymphomaandmultiplemyelomapatientsto increasethenumberofperipheralbloodstemcellswhen givenamobilizingregimenofG-CSF:implicationsforthe heavilypretreatedpatient.BiolBloodMarrowTransplant. 2009;15(2):249–56.
50.DevineSM,FlomenbergN,VesoleDH,LiesveldJ,WeisdorfD, BadelK,etal.RapidmobilizationofCD34+cellsfollowing administrationoftheCXCR4antagonistAMD3100topatients withmultiplemyelomaandnon-Hodgkin’slymphoma.JClin Oncol.2004;22(6):1095–102.
51.FlomenbergN,DevineSM,DipersioJF,LiesveldJL,McCarty JM,RowleySD,etal.TheuseofAMD3100plusG-CSFfor autologoushematopoieticprogenitorcellmobilizationis superiortoG-CSFalone.Blood.2005;106(5):1867–74.
52.DiPersioJF,MicallefIN,StiffPJ,BolwellBJ,MaziarzRT, JacobsenE,etal.PhaseIIIprospectiverandomized double-blindplacebo-controlledtrialofplerixaforplus granulocytecolony-stimulatingfactorcomparedwithplacebo plusgranulocytecolony-stimulatingfactorforautologous stem-cellmobilizationandtransplantationforpatientswith non-Hodgkin’slymphoma.JClinOncol.2009;27(28):4767–73.
53.DiPersioJF,StadtmauerEA,NademaneeA,MicallefIN,StiffPJ, KaufmanJL,etal.PlerixaforandG-CSFversusplaceboand G-CSFtomobilizehematopoieticstemcellsforautologous stemcelltransplantationinpatientswithmultiplemyeloma. Blood.2009;113(23):5720–6.
54.ShaughnessyP,ChaoN,ShapiroJ,WaltersK,McCartyJ, AbhyankarS,etal.Pharmacoeconomicsofhematopoietic stemcellmobilization:anoverviewofcurrentevidenceand gapsintheliterature.BiolBloodMarrowTransplant. 2013;19(9):1301–9.
55.MicallefIN,StiffPJ,DiPersioJF,MaziarzRT,McCartyJM, BridgerG,etal.Successfulstemcellremobilizationusing plerixafor(mozobil)plusgranulocytecolony-stimulating factorinpatientswithnon-Hodgkinlymphoma:resultsfrom theplerixaforNHLphase3studyrescueprotocol.BiolBlood MarrowTransplant.2009;15(12):1578–86.
56.MicallefIN,SinhaS,GastineauDA,WolfR,InwardsDJ,Gertz MA,etal.Cost-effectivenessanalysisofarisk-adapted
algorithmofplerixaforuseforautologousperipheralblood stemcellmobilization.BiolBloodMarrowTransplant. 2013;19(1):87–93.
57.AbhyankarS,DeJarnetteS,AljitawiO,GangulyS,MerkelD, McGuirkJ.Arisk-basedapproachtooptimizeautologous hematopoieticstemcell(HSC)collectionwiththeuseof plerixafor.BoneMarrowTransplant.2012;47(4):483–7.
58.AbusinGA,Abu-ArjaRF,GingrichRD,SilvermanMD,Zamba GK,SchlueterAJ.Analgorithmforutilizingperipheralblood CD34countasapredictoroftheneedforplerixaforin autologousstemcellmobilization–cost-effectiveness analysis.JClinApher.2013;28(4):293–300.
59.MicallefIN,SinhaS,GastineauDA,WolfR,InwardsDJ,Gertz MA,etal.Acosteffectiveanalysisofarisk-adaptedalgorithm forplerixaforuseinautologousperipheralbloodstemcell mobilization.BiolBloodMarrowTransplant.2011;17Suppl. 2:S159–60.
60.LiJ,HamiltonE,VaughnL,GraiserM,RenfroeH,Lechowicz MJ,etal.Effectivenessandcostanalysisofjustin-time salvageplerixaforadministrationinautologoustransplant patientswithpoorstemcellmobilizationkinetics. Transfusion.2011;51(10):2175–82.
61.VishnuP,RoyV,PaulsenA,ZubairAC.Efficacyand cost–benefitanalysisofrisk-adaptiveuseofplerixaforfor autologoushematopoieticprogenitorcellmobilization. Transfusion.2012;52(1):55–62.
62.KymesSM,PusicI,LambertDL,GregoryM,CarsonKR, DiPersioJF.Economicevaluationofplerixaforforstemcell mobilization.AmJManagCare.2012;18(1):33–41.
63.GertzMA,WolfRC,MicallefIN,GastineauDA.Clinicalimpact andresourceutilizationafterstemcellmobilizationfailurein patientswithmultiplemyelomaandlymphoma.Bone MarrowTransplant.2010;45(9):1396–403.
64.PavoneV,GaudioF,ConsoleG,VitoloU,IacopinoP,GuariniA, etal.Poormobilizationisanindependentprognosticfactorin patientswithmalignantlymphomastreatedbyperipheral bloodstemcelltransplantation.BoneMarrowTransplant. 2006;37(8):719–24.