w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Determination
of
an
unrelated
donor
pool
size
for
human
leukocyte
antigen-matched
platelets
in
Brazil
Carolina
Bonet
Bub
a,∗,
Margareth
Afonso
Torres
b,
Maria
Elisa
Moraes
b,
Nelson
Hamerschlak
a,
José
Mauro
Kutner
aaHospitalIsraelitaAlbertEinstein,SãoPaulo,SP,Brazil bLIGLaboratóriodeImunogenética,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received8September2015 Accepted18October2015
Availableonline28November2015
Keywords:
Platelettransfusion HLA
Refractoriness Donors
a
b
s
t
r
a
c
t
Background:Successfultransfusionofplateletrefractorypatientsisachallenge.Many poten-tialdonorsareneededtosustainhumanleukocyteantigenmatched-platelettransfusion programsbecauseofthedifferenttypesofantigensandtheconstantneedsofthesepatients. ForahighlymixedpopulationsuchastheBrazilianpopulation,thepoolsizerequiredto provideadequateplateletsupportisunknown.
Methods:Amathematicalmodelwascreatedtoestimatetheappropriatesizeofanunrelated donorpooltoprovidehumanleukocyteantigen-compatibleplateletsupportforaBrazilian population.Agroupof154hematologichumanleukocyteantigen-typedpatientswasused asthepotentialpatientpopulationandadatabaseof65,500humanleukocyteantigen-typed bonemarrowregistereddonorswasusedasthedonorpopulation.Plateletcompatibilitywas basedonthegradingsystemofDuquesnoy.
Results:Usingthemathematicalmodel,apoolcontaining31,940,1710and321donorswould benecessarytomatchmorethan80%ofthepatientswithatleastfivecompletelycompatible (nocross-reactivegroup),partialcompatible(onecross-reactivegroup)orlesscompatible (twocross-reactivegroup)donors,respectively.
Conclusion: ThephenotypicdiversityoftheBrazilianpopulationhasprobablymadeitmore difficultytofindcompletelycompatibledonors.However,thisheterogeneityseemstohave facilitatedfindingdonorswhencross-reactivegroupsareacceptedasproposedbythe grad-ingsystemofDuquesnoy.Theresultsofthisstudymayhelptoestablishunrelatedhuman leukocyteantigen-compatibleplatelettransfusions,aprocedurenotroutinelyperformedin mostBraziliantransfusionservices.
©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthorat:Av.AlbertEinstein,627/701,blocoE,3◦andar,Morumbi,05651-901SãoPaulo,SP,Brazil.
E-mailaddress:[email protected](C.B.Bub).
http://dx.doi.org/10.1016/j.bjhh.2015.10.005
Introduction
Plateletalloimmunizationiscommonlyseeninpatientswith hemato-oncological disorders requiring frequent red blood celland platelet transfusions1 and may beassociatedwith refractorinesstoplatelettransfusions(RPT).Theremayalso be anassociation between platelet transfusion failure and patientsurvival,whichincreasestheclinicalimportanceof RPT.2
RPT is defined as inappropriately low platelet count increments following exposure to antigens after two or more(usually consecutive)transfusionsandmustbe deter-minedbyobjectivedatawhichdetermineplatelettransfusion outcomes.3 Thiscondition may becausedby immuneand non-immunefactors.Morethan80%ofRPTcasesarerelated tonon-immunecauses.Thus,immunecausesoccurinless than 20% of the cases involving alloimmunization against humanleukocyteantigens(HLA)and,toalesserextenthuman plateletantigens(HPA),followingexposureaftertransfusion, pregnancy, or transplantation.Amongthe immune causes, HLAantibodiesareresponsibleforapproximately80–90%of RPTcasesand HPAantibodiesforapproximately10–20%of cases,associatedornotwithHLAantibodies.4
Providing an adequate post-transfusion platelet count incrementtorefractorypatientsisnotaneasytask; transfu-sionofHLA-matchedplateletsisonepossibility.5However,itis verydifficulttofindmultipleHLA-compatiblerelateddonors foroneindividual.
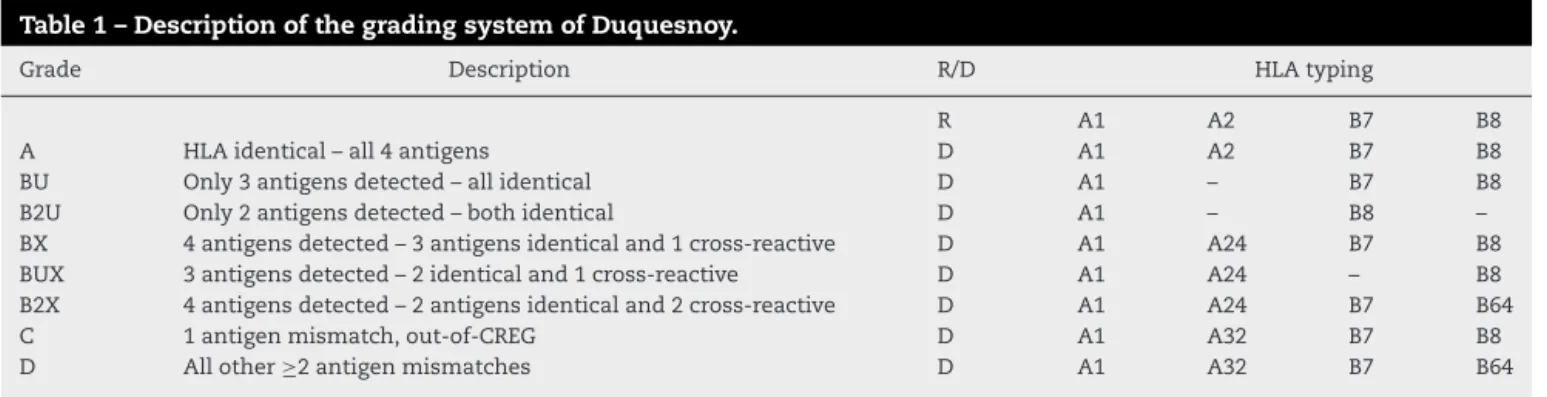
The HLA system is highly polymorphic6 and the prob-abilityoffinding identical matchesmay be around 10% of donations.7,8 When afullmatch cannotbefound,different strategiesareusedtoselectpartiallyHLA-matcheddonors. HLAclass Ispecificitiescan begrouped into cross-reactive groups (CREG), mismatches with antigenic similarity that resultinlessallorecognitionorimmuneactivation.9The grad-ing system described by Duquesnoy et al. in the 1970s10 (Table1)isdefinedaccordingtothepresenceofHLACREGs andisstillwidelyusedbytransfusionservices.Althoughin somecases,theselectionofmismatcheddonorsbasedonHLA CREGsmayfailtoproduceadequateincrements,11this strat-egycanincreasethenumberofpotentialdonorsinthesame donorbase.8
Poolsizecalculationscanbeanessentialcomponentfor therationalplanningofplateletsupportprograms.12Itis esti-mated that to provide atleast five completely compatible
donors formorethan 80% ofpatients,500, 1000, and1500 donorswouldbeneededfortheJapanese,EuropeanCaucasoid and North American Caucasoid populations, respectively.13 However, for a highly mixed population such as inBrazil, which is comprised of European, African and Amerindian roots,14thepoolsizerequiredtoprovidethesepatientswith adequateplateletsupportisunknown.
The unrelateddonor pool sizethat might be necessary if a center wants to provide patients with unrelated HLA-compatibleplatelets wasestimatedusingarandomsample from the Brazilianpopulation. A mathematical model was createdforcompatibilityanalysisanditsapplicationwas illus-tratedinapopulationof154cancerpatients.Thefindingsof thisstudymayhelptoestablishthetransfusionofunrelated HLA-compatibleplatelets,whichcurrentlyisnotaroutine pro-cedureinmanyBraziliancenters.
Methods
Studydatabase,designandsetting
A group of 154 HLA-typed patients who were submitted to bone marrow transplantation or who were candidates forthis procedure atHospital Israelita AlbertEinstein(São Paulo,Brazil)betweenJanuary2006andDecember2009were included in this retrospective study toillustrate apossible patientpopulation.
Adatabaseof65,500HLA-typedbonemarrowdonors, regis-teredintheLIGLaboratóriodeImunogenéticaLtda,SãoPaulo, Brazilwasusedinthisstudyasthepotentialdonor popula-tion.Thisdatabaseincludessamplesfromthesoutheastern (mainly),southernandnortheasternregionsofBraziland rep-resents a section ofthe National Registry of Bone Marrow Donors.AccordingtoaBraziliandemographiccensus,these regionsarerelatedto80%ofthepopulation15andmay rep-resentagoodpictureoftheHLAphenotypediversityofthe Brazilianpopulation.Thisstudy wasapprovedbyanEthics CommitteeandtheLocalReviewCommittee.
Measuresandstatisticalanalysis
Patientsanddonors
HLAtypingwasperformedbythepolymerasechainreaction sequence specificoligonucleotide probe(PCR-SSOP)method forlociAandB.
Table1–DescriptionofthegradingsystemofDuquesnoy.
Grade Description R/D HLAtyping
R A1 A2 B7 B8
A HLAidentical–all4antigens D A1 A2 B7 B8
BU Only3antigensdetected–allidentical D A1 – B7 B8
B2U Only2antigensdetected–bothidentical D A1 – B8 –
BX 4antigensdetected–3antigensidenticaland1cross-reactive D A1 A24 B7 B8
BUX 3antigensdetected–2identicaland1cross-reactive D A1 A24 – B8
B2X 4antigensdetected–2antigensidenticaland2cross-reactive D A1 A24 B7 B64
C 1antigenmismatch,out-of-CREG D A1 A32 B7 B8
D Allother≥2antigenmismatches D A1 A32 B7 B64
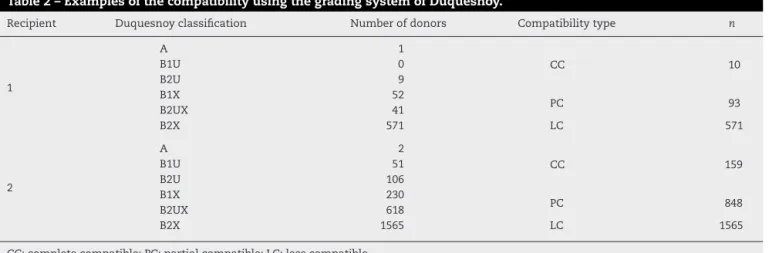
Table2–ExamplesofthecompatibilityusingthegradingsystemofDuquesnoy.
Recipient Duquesnoyclassification Numberofdonors Compatibilitytype n
1
A 1
CC 10
B1U 0
B2U 9
B1X 52
PC 93
B2UX 41
B2X 571 LC 571
2
A 2
CC 159
B1U 51
B2U 106
B1X 230
PC 848
B2UX 618
B2X 1565 LC 1565
CC:completecompatible;PC:partialcompatible;LC:lesscompatible.
Inorder tosearch thedonors tomatch each ofthe154 patientsautomatically,amathematicalmodelwasgenerated usingaVisualBasiccomputerprogram.16PlateletHLA com-patibility was based on the grading system of Duquesnoy andHLAcross-reactive antigenswere usedasdescribed in
Table1.17,18
Donors foreach patient were grouped according to the compatibilityfound defined ascompletely compatible (CC) formatchesA, B1U, B2U(no CREG present), partially com-patible(PC)forB1X,B2UXmatches(onlyoneCREGpresent) andlesscompatible(LC)forB2Xmatches(twoCREGspresent). Theresultsobtainedoftwoexamplesfromthemathematical modelvalidationprocessaredescribedinTable2.
An estimation of the required number of donors for eachpatientwascalculatedusingbinomialdistributionwith parametersgivenbytheproportionofcompatibilityobserved inthedonorpopulation.Thecurvestoestimatethedonorpool sizewerebuiltaccordingtothepercentageofpatientswithat
leastoneandfivecompatibledonorsforeachsimulatedpool size.Detailsofthe mathematicalmodelare availableupon request.
Theprojectionmodelwasappliedinordertodefinehow largethedonorpoolshouldbetoprovideatleastfiveCC,five PCorfiveLCdonorsfor80%ofthepatientpopulation,which wasconsideredanacceptablenumberofdonorsforplatelet supportduringthethrombocytopenicperiod.
Validationofthemathematicalmodel
Themathematical modelwasvalidated byrandomlyusing 10%(15/154)ofthepatientgroup.TwoHLAexpertsselected compatibledonorsbasedontheCREGdefinitionand manu-allygroupedthembasedonthegradingsystemofDuquesnoy usingthefiltertooloftheExcelprogram.Thesame compat-ibledonorswereobtainedbothbymanualselectionandby themathematicalmodel.Duringthisvalidationperiodthere
CC match
P
ercent of patients
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
0 10 000 20 000 30 000 40 000
Number of donors
50 000 60 000
% of patients with at least 1 CC donor match % of patients with at least 5 CC donor match
PC match
P
ercent of patients
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
0 5000 10 000 15 000 20 000
Number of donors
% of patients with at least 1 PC donor match % of patients with at least 5 PC donor match
Figure2–Percentageofpatientswithatleastoneorfivepartiallycompatible(PC)humanleukocyteantigenmatched plateletsfromanumberofregistereddonors.Dashedlinesrepresent95%confidenceintervals.
were noerrors duetofailures ofthe model, therefore,the automationtoolprovidedreliablehistocompatibilityanalyses.
Results
Probabilityforfindingmatcheddonors
Thecompatibilityprogramrevealedthatofthe154patients, 141 (91.6%) had at least five CC in the database of 65,500
registereddonors,andallpatients(100%)hadatleastfivePC andLCdonors.
Requiredpoolsizetomatch80%ofthepatientpopulation
withatleastonedonor
Figures1–3showthataccordingtothisprojectionmodelitis necessarytohaveapoolcontaining6502,341and65donors, respectivelytomatchaminimumof80%ofthepatientswith atleastoneCC,PCorLCdonor.Morethan65,500donorswould
LC match
P
ercent of patients
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
0 500 1000 1500 2000 2500
Number of donors
% of patients with at least 1 LC donor match % of patients with at least 5 LC donor match
benecessarytofindatleastoneCCdonorforallpatients(100% successrate).
Requiredpoolsizestomatch80%ofthepatient
populationwithatleastfivedonors
Poolsof31,940,1710and321donorswouldbenecessaryto provideatleastfiveCC,PCorLCdonorsto80%ofthepatients, respectivelyaccordingtotheprojectionmodel(Figures1–3). Poolsof23,393and2500donorswouldbeenoughtomatch 100%ofthepatientswithfivePCandLCdonors,respectively.
Discussion
The present projection model shows that pools of31,940, 1710and321donorswouldbenecessarytomatch80%ofthe patientswithatleastfiveCC,PCorLCdonors,respectively. Thiscalculation, basedonadifferentmathematicalmodel, hasalreadybeenperformedfortheJapanese,European Cau-casoidandNorthAmericanCaucasoidpopulationsinwhich 500,1000,and1500donorcandidateswouldbeneededtofind atleast fiveLCdonorsformorethan 80%ofeach ofthese populations.Ontheotherhand,tofindatleastfiveCC,5000, 18,000and25,000preselecteddonorcandidateswouldbe nec-essaryforthesepopulations,respectively.13Inanotherstudy, the authors concluded that 1500platelet donorswould be requiredtosupply75%ofthepatientswitheightLCdonors intheNorth AmericanCaucasoid population.This calcula-tionwouldmeetthetransfusionneedsofcommunitydonor plateletapheresisprogramsinareferencecenter(Seattle)of theUnitedStates.19
Brazil’sethnicandgeneticheterogeneity,whichisrelated tothe allelic variants present inthe first populations that inhabitedthecountry,20combinedwiththeexistenceofmany HLApolymorphisms,hasmostlikelymadeitmoredifficultto findatleastoneCC,evenwhenadatabaseof65,500 individ-ualsisused.However,thisheterogeneityseemstohaveacted asafacilitatorwhencross-reactiveantigensareaccepted,as inthegradingsystemofDuquesnoy.
BX or B2X mismatched products have already been reported as an acceptable match for platelet transfusions when the recipients’ lymphocytotoxic antibodies have low reactivity,21 even though this type of blood product can increasethechancesofalloimmunizationand makefuture transfusions difficult. Thisstudy shows that, for this level ofcompatibility,the poolmay befeasibleand should have 321–1710 donors. However, to provide five matching CC donors,alargernumberofdonorswouldbeneeded(31,940). Thesedatasupportthestrategyofincludinganysingle cross-reactive antigen while selecting donors, particularly if the patienttobetransfusedpresentslowtitersofantibodiesand consequentlyalowprobabilityofalloimmunization.
Successfultransfusionofpatientswithplateletrefractory thrombocytopenia is extremely important. However, many potentialdonorsareneededtosustainHLA-matchedplatelet transfusionprogramsbecauseoftheconsiderablevarietyof HLA types and the constant needs of these patients. The questionoftherequireddonorpoolsizeshouldalsoconsider feasibilityandcosts.12 Thelatterisoneofthereasonswhy
therearenowell-establishedunrelatedHLA-matchedplatelet transfusionprogramsinmostBrazilianservices.Poolsize cal-culationsmayprovideessentialdataforrationalplanningof platelettransfusionsupportprogramsandguideinstitutions thataimtobuildaplateletdonorregistry.
TheuseofHLA-matchedplateletsisnottheonlyapproach usedtomanagealloimmuneRPT.Crossmatchingandsupport withantigennegativeplateletunitsallowrapidselectionof donors, mainly inpatients with uncommonHLA typesfor whomitmightbevirtuallyimpossibletofindHLA-compatible donors.22–24 Recently,the use oftheHLAMatchmaker algo-rithm has been reported as an emerging concept for the managementofrefractorypatients.25,26 Thecombinationof matching compatible antigens and the application of mis-matchacceptabilitydeterminedbyserumscreeningforHLA antibodieshasofferedaneffectiveapproachtoanHLA-based platelettransfusionsupportpolicyforrefractorypatients.27,28 Thelackofantibodyspecificityisamajorlimitationinthis study asitdoes notaccountforthe relativefrequenciesof certainantibodiesinthepopulation.
Although the frequency of immune refractoriness has declined during the past decade due tothe application of universal leukoreductionofplateletpreparations,2,29 RPTis acomplexprocessandposesagreatchallengeinthe treat-mentofthrombocytopenicpatients.However,universalblood leukoreduction isnotfrequentin thetransfusion practices ofBrazilandthusRPTisstilladifficultnationwideproblem. Knowinghowlargethedonorpoolhastobe,mayhelpand stimulatedifferentcentersinBraziltobuildunrelatedplatelet donorpanels.
Inconclusion, accordingtothe projectionmodel,31,940 and321donorswouldbenecessarytoprovideatleastfiveCC orLCdonors,respectivelyto80%ofthepatientsinthe Brazil-ianpopulation.Furthermore,23,393and2500donorswould beenoughtomatch100%ofthepatientswithfivePCandLC donors,respectively.Ontheotherhand,theCCpoolsizeto match100%ofpatientsisnotpossibletocalculatepossibly becauseofthegreatracialmiscegenationofBrazilians.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BajpaiM,KauraB,MarwahaN,KumariS,SharmaRR, AgnihotriSK.Plateletalloimmunizationinmultitransfused patientswithhaemato-oncologicaldisorders.NatlMedJ India.2005;18(3):134–6.
2.KerkhoffsJL,EikenboomJC,vandeWateringLM,van Wordragen-VlaswinkelRJ,WijermansPW,BrandA.The clinicalimpactofplateletrefractoriness:correlationwith bleedingandsurvival.Transfusion.2008;48(9):1959–65.
3.RebullaP.Refractorinesstoplatelettransfusion.CurrOpin Hematol.2002;9(6):516–20.
5. SacherRA,KicklerTS,SchifferCA,ShermanLA,BraceyAW, ShulmanIA.Managementofpatientsrefractorytoplatelet transfusion.ArchPatholLabMed.2003;127(4):409–14.
6. ChooSY.TheHLAsystem:genetics,immunology,clinical testing,andclinicalimplications.YonseiMedJ.
2007;48(1):11–23.
7. Delaflor-WeissE,MintzPD.Theevaluationandmanagement ofplateletrefractorinessandalloimmunization.Transfus MedRev.2000;14(2):180–96.
8. SchifferCA,KellerC,DutcherJP,AisnerJ,HoggeD,Wiernik PH.PotentialHLA-matchedplateletdonoravailabilityfor alloimmunizedpatients.Transfusion.1983;23(4):286–9.
9. RodeyGE,FullerTC.Publicepitopesandtheantigenic structureoftheHLAmolecules.CritRevImmunol. 1987;7(3):229–67.
10.DuquesnoyRJ,FilipDJ,RodeyGE,RimmAA,AsterRH. SuccessfultransfusionofplateletsmismatchedforHLA antigenstoalloimmunizedthrombocytopenicpatients.AmJ Hematol.1977;2(3):219–26.
11.MoroffG,GarrattyG,HealJM,MacPhersonBR,StroncekD, HuangST,etal.Selectionofplateletsforrefractorypatients byHLAmatchingandprospectivecrossmatching.
Transfusion.1992;32(September(7)):633–40.
12.MickeyR.DonorpoolsizesforHLAmatching.Transfusion. 1989;29(4):285–6.
13.TakahashiK,JujiT,MiyazakiH.Determinationofan appropriatesizeofunrelateddonorpooltoberegisteredfor HLA-matchedplatelettransfusion.Transfusion.
1987;27(5):394–8.
14.ParraFC,AmadoRC,LambertucciJR,RochaJ,AntunesCM, PenaSD.ColorandgenomicancestryinBrazilians.ProcNatl AcadSciUSA.2003;100(1):177–82.
15.InstitutoBrasileirodeGeografiaeEstatística(IBGE). ContagemdaPopulac¸ão;2007.Availablefrom:http://www. ibge.gov.br/home/estatistica/populacao/contagem2007/ default.shtm[cited2013January].
16.MICROSOFT.MS-Excel.versão14.02010paraMicrosoft Windows2010.Availablefrom:
http://office.microsoft.com/pt-br/excel/default.aspx.
17.RodeyGE,NeylanJF,WhelchelJD,RevelsKW,BrayRA.Epitope specificityofHLAclassIalloantibodies.I.Frequencyanalysis ofantibodiestoprivateversuspublicspecificitiesinpotential transplantrecipients.HumImmunol.1994;39(4):272–80.
18.RodeyGE,RevelsK,FullerTC.EpitopespecificityofHLAclass Ialloantibodies:II.Stabilityofcross-reactivegroupantibody
patternsoverextendedtimeperiods.Transplantation. 1997;63(6):885–93.
19.BolgianoDC,LarsonEB,SlichterSJ.Amodeltodetermine requiredpoolsizeforHLA-typedcommunitydonorapheresis programs.Transfusion.1989;29(4):306–10.
20.PenaSD.Reasonsforbanishingtheconceptofracefrom Brazilianmedicine.HistCiencSaudeManguinhos. 2005;12(2):321–46.
21.HusseinMA,LeeEJ,FletcherR,SchifferCA.Theeffectof lymphocytotoxicantibodyreactivityontheresultsofsingle antigenmismatchedplatelettransfusionstoalloimmunized patients.Blood.1996;87(9):3959–62.
22.O’ConnellBA,LeeEJ,RothkoK,HusseinMA,SchifferCA. Selectionofhistocompatibleapheresisplateletdonorsby cross-matchingrandomdonorplateletconcentrates.Blood. 1992;79(2):527–31.
23.PetzLD,GarrattyG,CalhounL,ClarkBD,TerasakiPI,Gresens C,etal.Selectingdonorsofplateletsforrefractorypatientson thebasisofHLAantibodyspecificity.Transfusion.
2000;40(12):1446–56.
24.HodE,SchwartzJ.Platelettransfusionrefractoriness.BrJ Haematol.2008;142(3):348–60.
25.BrooksEG,MacPhersonBR,FungMK.Validationof HLAMatchmakeralgorithminidentifyingacceptableHLA mismatchesforthrombocytopenicpatientsrefractoryto platelettransfusions.Transfusion.2008;48(10):
2159–66.
26.BubCB,Gonc¸alezAC,Barjas-CastroML,SousaLC,doMonte SJ,CastroV.Theuseofapotentialnoveltoolinvirtual crossmatchingforplatelettransfusioninplatelet refractoriness.VoxSang.2016;110(1):70–8.
27.DuquesnoyRJ.Structuralepitopematchingfor HLA-alloimmunizedthrombocytopenicpatients:anew strategytoprovidemoreeffectiveplatelettransfusion support?Transfusion(Paris).2008;48(2):221–7.
28.NambiarA,DuquesnoyRJ,AdamsS,ZhaoY,OblitasJ,Leitman S,etal.HLAMatchmaker-drivenanalysisofresponsesto HLA-typedplatelettransfusionsinalloimmunized thrombocytopenicpatients.Blood.2006;107(4):1680–7.
29.SlichterSJ,DavisK,EnrightH,BraineH,GernsheimerT,Kao KJ,etal.Factorsaffectingposttransfusionplatelet