r e v b r a s o r t o p . 2014;49(1):74–77
w w w . r b o . o r g . b r
Case
Report
Lipoma
arborescens
of
the
knee:
a
case
report
夽
,
夽夽
Daniel
Rodrigo
Klein
Servic¸odeOrtopediaeTraumatologia,HospitalArquidiocesanoCônsulCarlosRenaux,Brusque,SC,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received2December2012 Accepted22March2013
Keywords:
Knee
Lipomaarborescens Synovialmembrane
a
b
s
t
r
a
c
t
Casereportofafemalepatientof26yearswhocomplainedofpainandrecurrentepisodes ofjointswellinginhisleftkneeabout10yearsago.Afteranamnesis,physical examina-tionandradiographicimagingandmagneticresonancewerediagnosedwitharborescent lipomaoftheknee,andthepatientunderwentarthroscopictreatmentforresectionofthe lesion.Postoperativelythepatientwasreferredtophysicaltherapyrehabilitationwithgood evolution.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Lipoma
arborescente
de
joelho:
relato
de
caso
Palavras-chave:
Joelho
Lipomaarborescente Membranasinovial
r
e
s
u
m
o
Relatodecasodeumpacientedosexofemininode26anosqueapresentavaqueixasde doreseventuaise episódiosrecorrentesdederramearticularno joelhoesquerdohavia aproximadamente10anos.Apósanamnese,examefísico,examesradiográficoseexames deimagemporressonânciamagnéticafoifirmadoodiagnósticodelipomaarborescente dejoelho.Apacientefoisubmetidaatratamentoartroscópicopararessecc¸ãodalesão.No pós-operatóriofoiencaminhadaparareabilitac¸ãofisioterápica,comboaevoluc¸ão.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora Ltda.Todososdireitosreservados.
Introduction
Arborescentlipomaisararebenignintra-articularlesion char-acterizedbydiffusereplacementofsynovialtissuebymature adipocytes,causingavillouslipomatousproliferationofthe sinovialmembrane.1
Typically,this isamonoarticular condition. Theknee is themostcommonlyaffectedjoint.Thehighestincidenceof
夽
Pleasecitethisarticleas:KleinDR.Lipomaarborescentedejoelho:relatodecaso.RevBrasOrtop.2014;49:74–77.
夽夽
StudyconductedatOrthopedyandTraumatologyService,HospitalArquidiocesanoCônsulCarlosRenaux,Brusque,SC,Brazil. E-mail:[email protected]
presentation occurs inthe fourthand fifthdecades oflife, withnopredilectionforgender.2Thetypicalclinical
presenta-tionconsistsofrepetitioneffusions,oftenwithlargevolume, accompaniedbyadiffuseandintermittentpain.Intheknee theconditioncommonlyaffectsthesuprapatellarpouch,with asoftconsistencyonpalpation.Weshouldsuspectthe diag-nosisinapatientwhoseclinicalhistoryisoffrequentjoint effusions,occasionalpainandincreasedvolumeinthe supra-patellaraspect.Radiographicstudiesmaybenormalorshow
2255-4971/$–seefrontmatter©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
rev bras ortop.2014;49(1):74–77
75
Fig.1–Increasedvolumeintheleftknee.
nonspecificchanges, suchas increasedsoft tissue or even degenerativechanges.2Magneticresonanceimaging(MRI)is
theprimarydiagnostictest.Theimageofamassofsynovial villousarchitecture,withisointensitywithsubcutaneousfat, isconsideredbysomeauthorsaspathognomonicfor arbores-cent lipoma,which enablesthe establishmentofdiagnosis evenbeforethe resultsofthe anatomopathological exami-nation.Therecommendedtreatmentisopenorarthroscopic synovectomy,withveryrarecasesofrecurrenceofpatology.3
Case
report
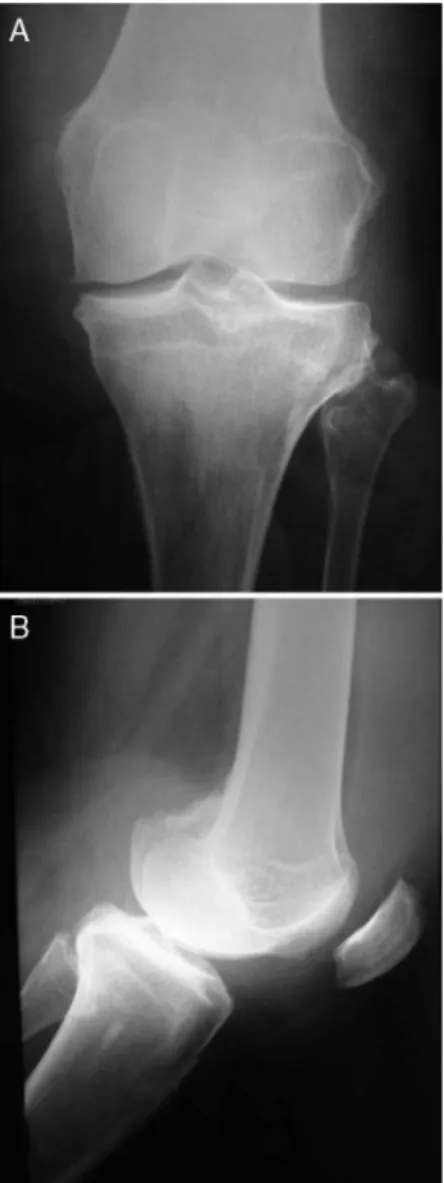
Female,26 years old.Thepatientreportedthat, since ado-lescence, had episodes of swelling and occasional pain in theleftkneewithoutanytriggeringtraumaticevent.Denied ahistoryofgivingwayorlockingofthe joint,havingseen several doctors; sometimes, she underwent arthrocentesis withoutdiagnosis.Hersymptomswerereasonablywell con-trolledwithphysicaltherapytomaintainmusclecontroland rangeofmotion.Onphysicalexamination,shehadbilateral genuvalgus, withswellinginthe leftknee (Fig.1).Shealso presentedapalpablemassofsoftandpainlessconsistency inthelateralaspect,andapositivekeysigninferring mod-eratejoint effusion,rangeofmotionwithaudiblecrackling inflexion-extension arcand pain withcompression ofthe patellofemoraljoint. Themaneuversin search ofligament andmeniscallesionswere negative,withnoother relevant signsor symptoms. Thepatienthad nofamily orpersonal historyworthyofnote.Plainradiographsofthekneeshowed reducedmedialjointspace,subchondralsclerosis,and reac-tionalosteophytes(Fig.2).
MRI demonstrated a large joint effusion, thickening of synovial membranes with enhancement after contrast mediumwithfinger-like aspectandlipomatous contenton the lateral aspect of the joint, besides degenerative chon-dralcompartmentalchangesanddegenerationinthebodyof themedialmeniscus(Fig.3).Afterevaluationofthe physi-calexaminationandlaboratorytests,thepatientunderwent videoarthroscopywithuseofanterior-inferiorand anterior-superiorportalstoresectthelesion andtoobtain material foranatomopathologicalexamination,withconfirmationof
Fig.2–RadiographsoftheleftkneeinAP(A)andlateral viewsshowingdegenerativechanges(B).
thediagnosisoflipomaarborescens.Besidescompartmental degenerativelesions,thearthroscopicexaminationrevealed synovitisofpedunculatedappearanceandareddish,diffuse color,withpredominanceinthelateralgutter(Fig.4).
Adrainsuctionwasappliedfor24h,collectingavolumeof approximately350mLofblood.Thepatientwasdischarged without complaintsthe next day after the procedure. The physicaltherapywasinitiatedimmediately afterdischarge, aimingtomaintaintherangeofmotionandmusclecontrol, andthepatientwasallowedtosupporttheweightastolerated. Thirtydaysaftersurgery,thepatientwasallowedtoreturn toherusualactivities. Inherlatestrevision(approximately threemonthspostoperatively),thepatientwasasymptomatic withminimaljointeffusion. Inthefirstyear,the follow-up willbesemiannual;subsequently,thepatientwillbeannually accompaniedfortwoyears.
Discussion
76
rev bras ortop.2014;49(1):74–77Fig.3–Magneticresonanceimaginginsagittal(A),coronal (B)andaxial(C)slices,depictingthevillousandlipomatous appearanceofthesynovialmembrane.
prominentvilloustransformation.4 Itsetiology isunknown,
althoughinsomecasesthisproblemisassociatedwithcertain conditions,suchasdegenerativejointdisease,diabetes melli-tus,rheumatoid arthritis,andpsoriaticarthritis,suggesting the possibility of a reaction process.1 Popliteal cysts were
notedinapproximately20%ofreportedcases.4Althoughthe
knee is the most commonly affected joint, there are also reportsofinvolvementinthe wrist,4,5 elbow,4,6 shoulder,4,7
ankle,4,8 and hip.4,9 The differential diagnosis of
arbores-cent lipoma of the knee includes pigmented villonodular synovitis,intra-articularlipomaoftheknee,synovial chondro-matosis,synovialhemangioma,andrheumatoidarthritis.1,4
Itsinsidiousclinicalcourse,supplementedbytestssuchas radiographyandmainlyMRI,virtuallyconfirmsthediagnosis. A synovialmass of villousarchitecture depicting isointen-sity with subcutaneous fat (hyperintense on T1, which is abolishedinthesequenceswithfatsaturation)canbeseen on MRI. There is no contrast uptakeby the lesion,which
Fig.4–Intraoperativemacroscopicappearanceofthe lesion(AandB):diffusevillousprojectionswithreddish color,locatedpredominantlyinthelateralgutter.
excludesotherinflammatoryorneoplasticprocessesofthe synovia.However,someintra-articulardiffusionofthe con-trastintothejointfluid,withinsinuationbetweenthesinovial lipomatous villous projections, can be seen, giving rise to smallareasofuptake.1Nowadays,withthemorewidespread
use of MRI, it has become more easier to diagnose this pathology.
Theopenorarthroscopicsynovectomyisconsidered cura-tivebymostauthors.Althoughtherearefewpublishedcases of arthroscopic synovectomy, these showed good progress during a follow-up period ofup to two years,2 with lower
morbiditywhencomparedtocaseswhereopenconventional treatmentwasdone.1Wefoundnomajortechnicaldifficulties
forthearthroscopicprocedure,perhapsbecausethespecific localizationofthepathologyintheanterioraspectoftheknee. The use ofthe anterior- superioraccessory portals greatly facilitatedtheprocedure,withlittleincreaseinmorbidityfor thepatient.Adrainsuctionshouldbeappliedforaperiodof approximately24hafterthesurgery,inviewofthebleeding thatoccursaftertheprocedure.
rev bras ortop.2014;49(1):74–77
77
Conflicts
of
interest
Theauthordeclaresnoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BernardoA,BernardesM,BritoI,VieiraA,VenturaF.Lipoma arborescentedasinovial.ActaMedPort.2004;17:325–8.
2.SailhanF,HautefortP,CoulombA,MaryP,DamsinJP.Bilateral lipomaarborescensoftheknee:acasereport.JBoneJointSurg Am.2011;93(2):195–8.
3.SumathiS,KhanDM,AnnamV,MrinaliniVR.Secondary unilateralmonoarticularlipomaarborescensoftheknee.A casereportwithreviewofliterature.IntJBiolMedRes. 2012;3(1):1456–8.
4.KloenP,KeelSB,ChandlerHP,GeigerRH,ZarinsB,Rosenberg AE.Lipomaarborescensoftheknee.JBoneJointSurgBr. 1998;80(2):298–301.
5.GaedeEA.Einfallvonsynovitischronicavillosageneralisata. ArchOrthopUnfallchir.1961;53:315–9.
6.LevadouxM,GadeaJ,FlandrinP,CarlosE,AswadR,PanuelM. Lipomaarborescensoftheelbow:acasereport.JHandSurg Am.2000;25(3):580–4.
7.LaorrA,PeterfyCG,TirmanPF,RabassaAE.Lipoma arborescensoftheshoulder:magneticresonanceimaging findings.CanAssocRadiolJ.1995;46(4):311–3.
8.NapolitanoA.Lipomaarborescensofthesynovialfluid; clinicalcontributiontoacaselocatedatthesynoviaofthe wrist.ProgMed(Napoli).1957;13(4):
109–18.