w w w . r b o . o r g . b r
Original
Article
Clinical
and
radiographic
medium-term
evaluation
on
patients
with
developmental
dysplasia
of
the
hip,
who
were
submitted
to
open
reduction,
capsuloplasty
and
Salter
osteotomy
夽
,
夽夽
Válney
Luiz
da
Rocha,
Guilherme
Lima
Marques,
Leonardo
Jorge
da
Silva,
Tiago
Augusto
di
Macedo
Bernardes,
Frederico
Barra
de
Moraes
∗DepartamentodeOrtopediaeTraumatologia,HospitaldasClínicas,UniversidadeFederaldeGoiás,Goiânia,GO,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received12October2012 Accepted22March2013
Keywords:
Congenitalhipdislocation/surgery Surgicalprocedures
Operative/methods Bonediseases Developmental
Hip/growthanddevelopment
a
b
s
t
r
a
c
t
Objective:toevaluatetheclinicalandradiographicmedium-termresultsfromsurgical treat-ment ofdevelopmentaldysplasia throughopenreduction,Salteretal.’sosteotomyand capsuloplasty.
Methods:13patientswereevaluated,13hipstreatedsurgicallybytheproposedtechnique between2004and2011.AclinicalandradiographicevaluationwasconductedbyDutoit etal.andSeverinetal.criteria,respectively.
Results:theacetabularpreoperativeindexforthe13surgicallytreatedhipsrangedfrom27◦
to50◦(averageof36),andaftersurgicalcorrectionto18.5◦(10–28◦),sothattheevaluationsof
preoperativeandpostoperativeacetabularindexesshowedupsignificantstatisticreduction (p<0.05).Regardingthepostoperativeclinicalevaluation,itwasfound:nineexcellenthips (69.2%),threegoodones(23.1%),nofairhips(0%)andapoorone(7.7%).Inradiographic evaluation,itwasfound:sixexcellenthips(46.1%),threegoodones(23.1%),nofairhips (0%)andfourpoorones(30.8%).Therefore,favorableresultswereobtained(92.3%),with groupedhipswithexcellentandgoodratingsassatisfactoryandwithfairandbadratingsas unsatisfactory.Itisalsoimportanttonoticethattherewasnosignificanceamongoccurrence ofcomplications,thepatient’sage,thetimeofsurgeryandthepreoperativeacetabularindex (p>0.05).Ascomplicationsoccurred,itwasfoundthatthreesubluxationsandasubluxation associatedwithavascularnecrosisofthefemoralhead.
Conclusion: openreduction,Salteretal.’sosteotomyandcapsuloplastyareseentobeaviable optionforthetreatmentofdevelopmentaldysplasiaofthehip,accordingtoclinicaland radiologicalmedium-termevaluations.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽Pleasecitethisarticleas:daRochaVL,MarquesGL,daSilvaLJ,diMacedoBernardesTA,deMoraesFB.Avaliac¸ãoclínicaeradiológica emmédioprazodospacientesportadoresdedisplasiadodesenvolvimentodoquadrilsubmetidosareduc¸ãoaberta,capsuloplastiae osteotomiadeSalter.RevBrasOrtop.2014;49:51–55.
夽夽
StudyconductedatPediatricOrthopediaService,DepartmentofOrthopediaandTraumatology,HospitaldasClínicas,Universidade FederaldeGoiás,Goiânia,GO,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](F.B.deMoraes).
2255-4971/$–seefrontmatter©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
capsuloplastia
e
osteotomia
de
Salter
Palavras-chave: Luxac¸ãocongênitado quadril/cirurgia
Procedimentoscirúrgicos operatórios/métodos Doenc¸asdodesenvolvimento ósseo
Quadril/crescimentoe desenvolvimento
r
e
s
u
m
o
Objetivo: avaliaroresultadoclínicoeradiológicodotratamentocirúrgicodadisplasiado desenvolvimentodoquadrilemmédioprazo,pormeiodareduc¸ãoaberta,dacapsuloplastia edaosteotomiadeSalteretal.
Métodos: foramavaliados13pacientes,13quadris,entre2004e2011,tratados cirurgica-mentepelatécnicaproposta.Umaavaliac¸ãoclínicaeradiológicafoifeitapeloscritériosde Dutoitetal.eSeverinetal.,respectivamente.
Resultados: nos13quadrisacometidosoíndiceacetabularpré-operatóriovarioude27◦a
50◦(médiade36)e,apóscorrec¸ãocirúrgica,para18,5◦emmédia,comvariac¸ãode10◦a28◦,
demodoqueasavaliac¸õesdosíndicesacetabularespréepós-operatóriosapresentaram reduc¸ãocomsignificânciaestatística(p<0,05).Quantoàavaliac¸ãoclínicapós-operatória, foramencontrados:novequadrisótimos(69,2%),trêsbons(23,1%),nenhumregular(0%)e umruim(7,7%).Naavaliac¸ãoradiológica,foramencontradosseisquadrisótimos(46,1%), trêsbons(23,1%),nenhumregular(0%)equatroruins(30,8%).Portanto,obtiveram-se result-ados favoráveis em 92,3%, pois agrupam-sequadris comavaliac¸ão ótima e boa como satisfatórioseoscomavaliac¸ãoregulareruimcomoinsatisfatórios.Atente-sequenão houvesignificânciaentreaocorrênciadecomplicac¸ões,aidadedopaciente,omomentoda cirurgiaeoíndiceacetabularpré-operatório(p>0,05).Comocomplicac¸õesocorridas, têm-setrêssubluxac¸õesisoladaseumasubluxac¸ãoassociadaànecroseavasculardacabec¸a femoral.
Conclusão:areduc¸ãoaberta,acapsuloplastiaeaosteotomiadeSalteretal.sãoconsideradas umaopc¸ãoviáveldopontodevistaclínicoeradiológicoemmédioprazoparaotratamento dadisplasiadodesenvolvimentodoquadril.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Developmentaldysplasiaofthe hip (DDH)involves a spec-trumofdevelopmentaldisordersofthehip,whichpresentin differentformsandages,fromaligamentlaxitytocomplete dislocationofthefemoralhead.Insuchcases,theacetabulum issituatedinananterosuperiorpositionasaresultof exces-siveanteversion,whichmakesitincreasinglyshallow,thick and oblique.DDHis classifiedinto two types:typical (sub-divided intodislocable, subluxated anddislocated hip)and teratologic.
Theetiology of DDH remains unknown, but ethnic and geneticfactorsareimportant.Geneticfactorsmaydetermine theacetabulardysplasia,ligamentlaxityorboth,asreported by Wynne-Davies.1 In addition to the preexisting factors, mechanicalfactorssuchasintrauterinepositionand postna-talhabitscanalsointerferewiththeprocess.
Inseveralpapers,theincidenceofDDHrangedfrom2to17 per1000.InBrazil,VolponandCarvalhoFilho2demonstrated anincidenceof2.31per1000.
The treatment depends on the patient’s age, degree of acetabularandproximalfemurdysplasia.Itisconsideredthat, afterthestartofthewalking,asurgicaloptionforthe treat-mentofDDHconsistsofopenreduction,Salter’sosteotomy, andcapsuloplasty.3Thistechniquepromotesacetabular repo-sitioning,aimingtoincreasethecoverageofthefemoralhead, whichwillbesurgicallyreducedintotheacetabulum.
The aim ofthis study was to evaluate the clinical and radiologicaloutcomeinthemediumtermsurgicaltreatment ofDDHbyopenreduction,Salter’sosteotomy,and capsulo-plasty.
Materials
and
methods
Thirteenpatients who remained withDDH aftertheystart walking,whetherbyfailureofmedicaltreatmentinthefirst yearoflifeorbyreferralofthechildwithadelayed diagno-sis,wereevaluated.Allweretreatedsurgicallybetween2004 and2011,bythetechniquesofopenreduction,capsuloplasty, andSalter’sosteotomy.ThestudywasapprovedbytheEthics andResearchCommitteeofthehospital,wheretheworkwas done.
Fig.1–Surgicaltechnique:openreduction,capsuloplastyandSalter’sinnominateosteotomy.
underanaverageoutpatientfollow-upof5.3years(1.4–14.1 years).
Toevaluatetheresults,radiographicandclinicalcriteria wereemployed.Theradiographswereevaluatedbythe crite-riaofSeverin,5whichtakeintoaccounttheWibergacetabular (AC)andCEangles,thesphericityofthefemoralhead,the dis-locationandsubluxationofthehip,andoccurrence(ornot) ofarthrosis.Withrespecttotheclinicalsituation,the anal-ysiswasperformed inconformity toDutoitet al.criteria,6 basedonhipstabilityandmobility,pain,lamenessandonthe Trendelenburgtest.
Thestatistical analysiswasperformeddescriptivelyand analytically, with the methods of McNemar, Friedman, Wilcoxon and Univariate Logistic Regression Analysis, in
ordertoestablishstatisticalsignificancebetweentheclinical and radiologicalparameters,withasignificancelevelof5% (p<0.05).
Results
Thehipswerepooledforanalysisregardlessoftheinvolved side.Inthe13affectedhips,thepreoperativeacetabularindex rangedfrom 27◦ to50◦ (average,36◦)and afterthesurgical
correction,theaveragewas18.5◦ (10–28◦).Forthisestimate,
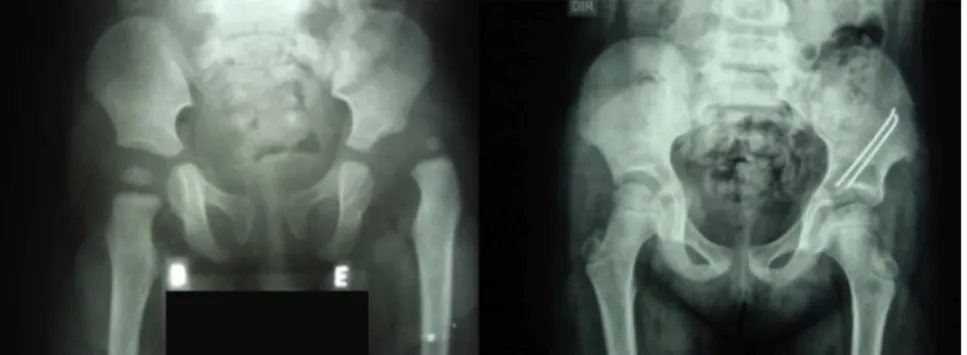
Fig.2–RadiologicalevolutionofafemalepatientwithDDHtreatedwithSalteretal.’sosteotomy.Excellentradiologicresult with53months’follow-up.
AccordingtoDutoitet al.,6 intheclinical evaluationwe couldobservenineverygood(69.2%),threegood(23.1%),0fair (0%),and1poor(7.7%)hip.Therefore,wegroupedhipswith goodandverygoodevaluationassatisfactory,andthosewith poorandfairevaluationasunsatisfactory.Hence,weobtained 92.3%satisfactoryresults(Table1).
Intheradiologicalstudy,sixverygood(46.1%)(Fig.2),three good(23.1%),0fair(0%),andfourpoor(30.8%)hipswerefound. Therefore,wegroupedhipswithgoodandverygood evalua-tionassatisfactory,andthosewithpoorandfairevaluationas unsatisfactory.Hence,weobtained69.2%offavorableresults
(Table2).
ToevaluatetheinfluenceofDutoitetal.6andofSeverin5 inrelationtopre-andpost-surgicaltreatment,consideringthe techniquesofopenreductionandcapsuloplastyandSalter’s osteotomy,McNemartestandFisheretal.’sexacttestwere applied,and noother correlationswere observed,i.e., only thesurgeryinterferedwiththeclinicalandradiological out-come.
Withregard tocomplications, twoisolated subluxations andoneosteonecrosisofthefemoralheadwithsubluxation
Table1–ResultsofclinicalevaluationaccordingDutoit.6
Treatment Pre Post
n % % Nutrition % %
Dutoit
1–excellent 0 0.0 9 69.2 92.3
2–good 0 0.0 3 23.1
3–regular 0 0.0 100.0 0 0.0 7.7
4–poor 13 100.0 1 7.7
Table2–Resultsofradiologicalevaluationaccording Severin5
Treatment Pre Post
n % % n % %
Severin
1–excellent 0 0.0 6 46.1 69.2
2–good 0 0.0 3 23.1
3–regular 2 15.4 100.0 0 0.0 30.8
4–poor 9 69.2 4 30.8
5–poor 1 7.7 0 0.0
6–poor 1 7.7 0 0.0
anddislocationoccurred.Thiswasoneofthecasesofisolated
subluxationtreatedwithanother surgicalprocedure. There
were nocases ofinfection, fracture, significant lower limb
dysmetria,orneurovascularinjury.
Discussion
Thesurgicaltreatmentofdevelopmentaldysplasiaofthehip
isbecominganincreasinglylessfrequentchallenge,thanksto
currentmethodsforearlydiagnosisandprevention,for
exam-ple,thephysicalexaminationofthenewbornandroutineuse
ofultrasonographyforsuspectedcases.Physicalexamination
toidentifycasesofDDHshouldbedoneroutinelyonall
new-borns.
The Ortolani maneuver, described in 1948 by Marino
OrtolaniapudTachdjian,4whenpositive,allowsthediagnosis
ofDDH;however,thenegativity doesnotexcludethe diag-nosis, because some hips are unstable,but not dislocated. TheBarlowprovocativemaneuverallowsthediagnosisofhip instability.Moreover,inchildrenolderthanthreemonths,the Ortolanimaneuvermaybenegative,becauseevenifthehip remainsdislocated,itwillbenolongerpossibletoreplacethe femoralheadinto theacetabulum.Withrespecttothe Bar-lowmaneuver,itmustbeemphasizedthatmanynewborns testedpositiveinthefirsttestbecomenegativeaftertwoor threeweeks.
Inthedislocatedhipthetreatmentconsistsconcentricand atraumaticreductionoffemoralheadwithintheacetabulum. Beforethestartofwalking,thistreatmentmaybe conserva-tive,however,afterthechildbeginstowalkthereisatendency ofinterpositionofsofttissues,suchastheroundligament, labrum and capsuleofthis joint.Hence,it isnecessaryan openreduction.Onceachieved,thisreductioncanbe main-tainedbymeansofproceduresontheacetabulum,softtissue, orboth.Lindstrometal.7showedthatiftheconcentric reduc-tionisachievedandmaintained,therewillberemodelingof theacetabulumthatwillbemorepronounceduptofouryears, andmayoccuruptoeightyears.
Basedonthejointmobilityandstabilityinthepresence ofpainand/orlameness,Dutoitetal.6developedasystemof post-surgicalclinicalclassification.
of the head/neck and acetabulum, with reference to the CEangle ofWiberg and presence ofpost-surgical subluxa-tion/dislocation.
Salteretal.3 describedaninnominateosteotomyforthe treatmentofcongenitalhipdislocationandsubluxationand promoted acetabularrepositioningwiththe formationof a rooftosupportthefemoralheadafterreduction.Intheirfirst report,Salteretal.evaluated25hipsafterfollow-upofone tothreeyears,andreportedthatalltheirpatientsachieveda goodorexcellentresult.
Bohm et al.8 studied 63 hips treated with innominate osteotomy,withamedianfollow-upof30.9years;in88.8%of cases,theyachievedsatisfactoryradiologicalresults, accord-ingtoSeverinindex.
Tukenmez et al.9 evaluated 61 hips treated withSalter osteotomyand obtainedsatisfactory clinical and radiologi-calresults in 82% (Dutoit) and 94.5% (Severin) procedures, respectively,withanincidenceof21.5%ofpost-operative com-plications.
Carvalho Filho et al.10 evaluated 18 patients with DDH treatedwithSalteretal.’sosteotomyandobtained72% satis-factoryclinicalresults(Dutoit)and81%favorableradiological outcomes (Severin); 16.6% of patients had post-operative redislocationinsidethecast.
Ofthe13hips includedinthisstudy,weobtained satis-factoryclinicalandradiologicalresultsin92.3%(Dutoit)and 69.2%(Severin),respectively.Thus,ourfindingsagreewiththe resultsofotherseries.
Salehetal.11havedemonstratedabsenceofpelvic remod-elingafter innominateosteotomyin patients withskeletal maturity. In this study, the osteotomy was performed in patientsbetween1.9and6years(agepost-march),yetthere wasnoinfluenceontheclinicalandradiographicresultsin themediumterm,accordingtothatdescribedbyCarvalhoand VolponFilho.2
Frequency,degreeofdisability,durationofsymptomsand morbidityweretakenintoaccount.However,osteonecrosisis themostfearedcomplicationoftreatmentofDDH,andoccurs onlyinpatientswhoreceivedsomeformofbloodyorbloodless treatment,being regardedasa commoncause ofhip posi-tioninginabduction>70◦ orinforcedmedialrotation. This
canoccureveninthenormalhipoppositetothatwhichis beingtreated.Therefore,hipimmobilizationsinanadequate positionandacarefulbloodlessorbloodyreductionin accor-dancewiththebasicprinciples,maydecreasetheriskofthis seriouscomplication.Itshouldbeborneinmindthat,inthis study,therewerecomplications,suchastwocasesofisolated
subluxation,acaseofosteonecrosisassociatedwith subluxa-tion,andonedislocation.
Conclusion
TheassociationofSalter’sosteotomywithopenreductionand capsuloplastybecomesaviableoptionforthetreatmentof DDHafterthechildbeginstowalk,withsatisfactoryclinical andradiologicalresults.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.Wynne-DaviesR.Acetabulardysplasiaandfamilialjoint
laxity:twoetiologicalfactorsincongenitaldislocationofthe
hip.Areviewof589patientsandtheirfamilies.JBoneJoint
SurgBr.1970;52(4):704–16.
2.VolponJB,CarvalhoFilhoG.Luxac¸ãocongênitadoquadrilno
recém-nascido.RevBrasOrtop.1985;20(7):317–20.
3.SalterRB.Innominateosteotomyintreatmentofcongenital
dislocationofthehip.JBoneJointSurg.1961;43:72–80.
4.TachdjianMO.Dysplasiacongenitalofthehip.In:Pediatric
orthopaedics.2nded.Philadelphia:Saunders;1990.
5.SeverinE.Contributiontoknowledgeofcongenital
dislocationofhipjoint:lateresultsofclosedreductionand
arthrographicstudiesofrecentcases.ActaChirScand.
1941;84:1–142.
6.DutoitM,MoulinP,MorscherE.Salter’sinnominate
osteotomy.20yearslater.ChirPediatr.1989;30(6):277–83.
7.LindstromJR,PonsetiIV,WengerDR.Acetabulardevelopment
afterreductionincongenitaldislocationofthehip.JBone
JointSurgAm.1979;61(1):112–8.
8.BöhmP,BrzuskeA.Salterinnominateosteotomyforthe
treatmentofdevelopmentaldysplasiaofthehipinchildren:
resultsofseventy-threeconsecutiveosteotomiesafter
twenty-sixtothirty-fiveyearsoffollow-up.JBoneJointSurg
Am.2002;84(2):178–86.
9.TukenmezM,TezerenG.Salterinnominateosteotomyfor
treatmentofdevelopmentaldysplasiaofthehip.JOrthop
Surg(HongKong).2007;15(3):286–90.
10.CarvalhoFilhoG,ChueireAG,HelencarI,CarneiroMO,
FranceseNetoJ,CarnesinAC.Tratamentocirúrgicoda
luxac¸ãocongênitadoquadrilpós-marcha:reduc¸ãoabertae
osteotomiadeSalter.ActaOrtopBras.2003;11(1):42–7.
11.SalehJM,O’SullivanME,O’BrienTM.Pelvicremodelingafter