w w w . r b o . o r g . b r
Original
Article
Blood
transfusion
in
hip
arthroplasty:
a
laboratory
hematic
curve
must
be
the
single
predictor
of
the
need
for
transfusion?
夽
,
夽夽
Felipe
Roth
a,∗,
Felipe
Cunha
Birriel
a,
Daniela
Furtado
Barreto
a,
Leonardo
Carbonera
Boschin
b,
Ramiro
Zilles
Gonc¸alves
a,b,
Anthony
Kerbes
Yépez
a,
Marcelo
Faria
Silva
c,
Carlos
Roberto
Schwartsmann
aaComplexoHospitalarSantaCasadeMisericórdiadePortoAlegre,PortoAlegre,RS,Brazil
bComplexoHospitalarSantaCasadeMisericórdiadePortoAlegre,HospitalCristoRedentor,PortoAlegre,RS,Brazil
cCentroUniversitárioMetodista,UniversidadeFederaldeCiênciasdaSaúdedePortoAlegre,PortoAlegre,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received23July2012
Accepted23November2012
Keywords:
Arthroplasty,replacement,hip
Bloodtransfusion
Hemoglobin
a
b
s
t
r
a
c
t
Objective:todeterminewhetherthelaboratoryhematiccurvemustbethesinglepredictor
ofpostoperativebloodtransfusionintotalhiparthroplasty.
Methods:the laboratory blood samplesof 78 consecutive patients undergoingtotal hip
arthroplastywasanalyzedduringfivedistinctmoments:onepreoperativeandfour
postop-erative.Therewasacountofhemoglobin,hematocritandplateletsofthepatientssamples.
Othercataloguedvariablesascertainpossibleriskfactorsrelatedtotransfusionalpractice.
Theycharacterizedtheanthropometric,behavioralandcomorbiditiesdatainthis
popula-tion.Thestudysubjectsweredividedandcategorizedintotwogroups:thosewhoreceived
bloodtransfusionduringoraftersurgery(Group1,G1),andthosewhodidnotaccomplish
bloodtransfusion(Group2, G2).TransfusionruleswereleadbyguidelinesofAmerican
AcademyofAnesthesiologyandtheBritishSocietyofHematology.
Results:atotalof27(34.6%)patientsreceivedbloodtransfusions.Thecurvesofhemoglobin,
hematocritandplatelettransfusionsbetweenG1andG2weresimilar(p>0.05).Noneofthe
analyzedriskfactorsmodifiedtherateoftransfusionrateintheiranalysiswithpvalue>0.05,
excepttherace.ThesumofclinicalcomorbiditiesassociatedwithpatientsinG1wasa
medianof3(95%CI2.29–3.40),whileinG2themedianwas2(95%CI1.90–2.61)withp=0.09.
Conclusion:thecurveinredbloodcellshaslimitedreliabilitywhenusedassoleparameter.
Theexistenceoftolerantpatientshematimetriccurvevariationsassumesthattheir
assess-mentsofclinical,functionalevaluationandco-morbidities areparametersthatshould
influencethedecisiontotransfusionredbloodcells.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.Allrightsreserved.
夽Pleasecitethisarticleas:RothF,BirrielFC,BarretoDF,BoschinLC,Gonc¸alvesRZ,YépezAK,SilvaMF,SchwartsmannCR.Transfusão
sanguíneaemartroplastiadequadril:acurvalaboratorialhemáticadeveseroúnicopreditordanecessidadedetransfusão?.RevBras
Ortop.2014;49:44–50.
夽夽
StudyconductedattheDepartmentofOrthopaedics,HospitalSantaCasadePortoAlegre,PortoAlegre,RS,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](F.Roth).
2255-4971/$–seefrontmatter©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
Transfusão
sanguínea
em
artroplastia
de
quadril:
a
curva
laboratorial
hemática
deve
ser
o
único
preditor
da
necessidade
de
transfusão?
Palavras-chave:
Artroplastiadequadril
Transfusãosanguínea
Hemoglobina
r
e
s
u
m
o
Objetivo: verificarseacurvalaboratorialhemáticadeveseroúnicopreditordetransfusão
sanguíneapós-operatóriaemartroplastiatotaldequadril(ATQ).
Métodos: amostraslaboratoriaissanguíneasde78 pacientesconsecutivossubmetidosà
ATQforamanalisadasemcincoemperíodosdistintos(umpré-operatórioequatro
pós--operatórios).Verificou-seacontagem dehemoglobina,hematócritoe plaquetasdesses
pacientes.Foramanalisadascaracterísticasantropométricasecomportamentaise
comor-bidadesreferentesà amostra, paraverificac¸ãode fatoresde risco associados à prática
transfusional.Osindivíduosdoestudoforamdivididosemdoisgrupos:aquelesque
rece-beramtransfusãosanguíneaforamalocadosnoGrupo1(G1)eosquenãoareceberam,
noGrupo2 (G2).Ascondutastransfusionaisrespaldaram-sedoscritériosda Academia
AmericanadeAnestesiologiaedaSociedadeBritânicadeHematologia.
Resultados: receberamtransfusãodehemoderivados27(34,6%)pacientes.Asanálisesdas
curvasdehemoglobina,hematócritoeplaquetasentreoG1eoG2nascincovisitasdistintas
foramsimilares(p>0,05).Todososfatoresderiscoanalisados,comexcec¸ãodaetnia,não
apresentaramrepercussõesnosíndicedetransfusãoemsuasanálisescomvalorp>0,05.A
somadascomorbidadesclínicasassociadasaospacientesnoG1foimedianade3(IC95%
2,29–3,40),enquantonoG2amedianafoi2(IC95%1,90–2,61)comvalorp=0,09.
Conclusão: a curva hemática apresenta confiabilidade limitada quando usada como
parâmetroexclusivoeabsoluto.Aexistênciadepacientestolerantesàsvariac¸õesdacurva
hematimétricapressupõequeassuasavaliac¸õesdecaráterclínico,funcionalede
comor-bidadessejamparâmetrosquedevaminfluenciarnadecisãodousodehemoderivados.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier
EditoraLtda.Todososdireitosreservados.
Introduction
Theindicationforbloodtransfusioninprostheticorthopedic
procedures–especiallyhiparthroplasty–generates
disagree-ment amongmedicalprofessionals as the management of
post-surgicalanemia.1–4Thestandardizationoftransfusional
proceduresinthe post-operativemanagementwith
labora-torythresholdswasinitiallydonein1942,5becauseofthefear
ofcomplicationssuchasfatigueandinabilitytorecoverand
rehabilitatethepatient,togetherwiththehighcostsandwith
themorbidityand longhospitalstays. Further
understand-ingofhumanphysiologybroughtgreaterdoubtabouttheuse
ofpreset laboratory thresholdsfor transfusion.Because of
theriskofbleedingduringandaftersurgery,andofdrainage
andsecretionofthesurgicalwound,itsimpositionasroutine
practice was countered by the risks related to the
conse-quencesofitsuse.Wereportanassociationofthispractice
withhighestratesofsurgicalsiteinfection,4,6andincreaseof
post-operativepneumoniaindexandmortalityinthe short
term,and vascular events, besides autoimmune reactions,
systemicinflammatoryresponsesyndrome,andtransmission
ofcontagiousdiseases.6–8
Numerousguidelines depictthelocalexperienceof
spe-cificcenters,ordemonstratethescenarioofmedicalgroups’
proceduresinseveralcountries,9–11 but thereisnosupport
orspecific worldwidestandardizationfortheseconducts.12
Prominentstudieswarnabouttheriskfactorsassociatedwith
bloodtransfusions,beingadamantindefiningoptional
preop-erativemethodsforreducingthecostsandmorbiditiesrelated
totheuseofallogeneicbloodproducts.Theusebefore,during
andafterthesurgicalproceduresofsubstancessuchas
fer-roussulphate,erythropoietin,trenexamicacid,recombinant
factorVIIandfibringlue,andthepromotionofprotocolsof
autotransfusion,hemodilutionandrescueofredbloodcells,8
arethemainapproaches,althoughnotwithoutrisks,8tosolve
thisissue.4,6,13–17
Thegapsrelatedtotheconductsregardingtheuseofblood
productsledustodefinetheoverallfunctioningofthe
post-operatory laboratory hematiccurve ofpatients undergoing
primarytotalhiparthroplasty(THA)inthisorthopedic
refer-ral service. The objective wasto understandthe real need
forblood transfusions based ontheir laboratoryresults. In
thisstudy,possiblefactorsthatcouldinfluencethe
transfu-sionprocedureswereexamined,toexplainwhysomepatients
presentedclinicalandlaboratoryrecoverywithouttheuseof
bloodtransfusion,basedonabsolutenumbers.Thisanalysis
questionsandalertsaboutnecessaryprecautionsofroutine
bloodtransfusion.
Materials
and
methods
FromJanuary2011toJune2012thosepatientsundergoingTHA
inthe SantaCasa dePorto Alegre(HSCPOA) Hospital
Com-plex were enrolled inthis prospectivestudy.Seventy-eight
participantswererandomizedandprovidedwritteninformed
consent.ThisstudywasapprovedbytheHSCPOAinstitutional
ethicsand researchboard.Patientswithanyhematopoietic
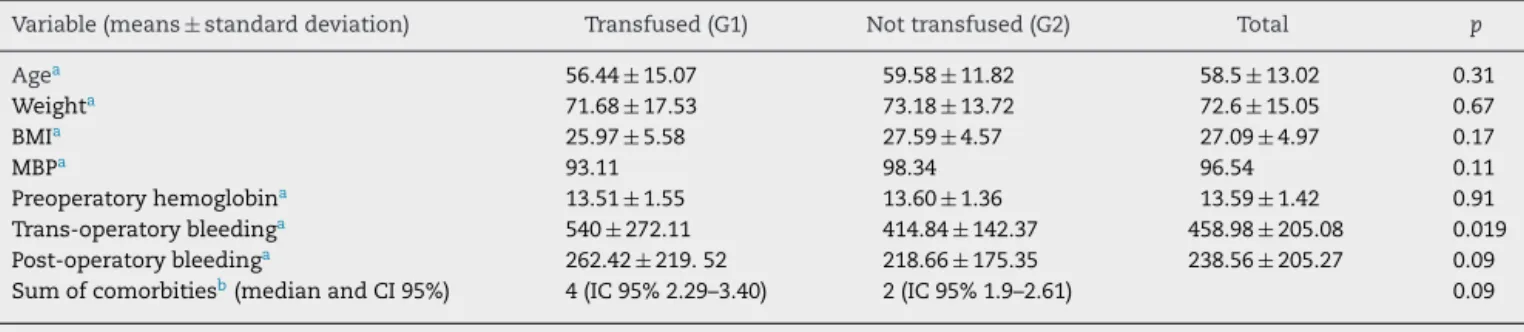
Table1–Riskfactorsamongtransfused(G1)andnottransfused(G2)patients(comparisonbetweenmeansofparametric
continuousvariablesandmedianofthenonparametricvariable).
Variable(means±standarddeviation) Transfused(G1) Nottransfused(G2) Total p
Agea 56.44±15.07 59.58±11.82 58.5±13.02 0.31
Weighta 71.68±17.53 73.18±13.72 72.6±15.05 0.67
BMIa 25.97±5.58 27.59±4.57 27.09±4.97 0.17
MBPa 93.11 98.34 96.54 0.11
Preoperatoryhemoglobina 13.51±1.55 13.60±1.36 13.59±1.42 0.91
Trans-operatorybleedinga 540±272.11 414.84±142.37 458.98±205.08 0.019
Post-operatorybleedinga 262.42±219.52 218.66±175.35 238.56±205.27 0.09
Sumofcomorbitiesb(medianandCI95%) 4(IC95%2.29–3.40) 2(IC95%1.9–2.61) 0.09
CI,confidenceinterval.
a Studentt-test. b Mann–WhitneyU-test.
orinfectiouschronicliverdisease,andwithmalignanttumor
wereexcludedfromthestudy.
Patients rigidly followed a protocol for collecting data
through serial visits. The first visit (V1) occurred
preoper-atively (from seven to three days before surgery); in this
stage,firsthematimetriclaboratorytestsanddemographics
and physical data ofthe participants (gender, age,
ethnic-ity, weight,height, body weightindex [BMI], comorbidities,
alcoholism,smoking,and vitalsigns)were collected;inthe
secondvisit(V2),whichoccurredonthefirstpost-operative
day(6–12haftersurgery),thesecondlaboratory
hematimet-ricsampleanddataregardingsurgerywerecollected,andthe
drainageofthesuctiondrainwascalculated;thethirdvisit
(V3)occurredonthesecondpost-operativeday(24–48hafter
surgery),withthesameproceduresofV2;thefourth(V4)and
thefifth(V5)visitsoccurredinthefirst(between4and7days)
and thirdweeks (14–17 days)post-operatively, respectively,
andwerecharacterizedbylaboratorycollectionanddatafrom
latepost-operativeperiod. Inthe laboratoryevaluation, we
analyzedtheredserieshemocytometry(hemoglobin,
hemat-ocritandplatelets).Thesamplecollectionsweredoneduring
thehospitalstay(V2–V3–V4)andintheoutpatientclinic(V1
andV5).
Allpatientswereoperatedonbythesamesurgicalteam,
consistingoftwosurgeonsandtwoanesthetists.The
surgi-calroutineconsistedofcalculatingtheintraoperativebleeding
(throughthesuctionvolumeofthedrainsandbyweighingthe
pads)andofageneraldescriptionoftheprostheticprocedure.
Theanestheticroutinewassimilarinallpatients:spinal
anes-thesiafollowedbysedation.Theposteriorsurgicaltechnique
foraccessforallcasesofTHAwaschosen.Duringthe
clo-sureofthesurgicalplans,allpatientsreceivedclosedsuction
drains,whichweremaintainedfor48h.Themeanoperative
timewas98.3±4.2min(range:80–120min).Post-operatively,
all patientsusedprophylacticunfractionated heparin(5000
units 12/12h) for a minimum of seven days and vacuum
suction drain for two days. Nopatient received steroidor
anti-inflammatorymedication.Analgesicdrugswerebasedon
opioidsandnon-narcoticpirazolonicderivatives(dipyrone).
Theproceduresofintraoperativeandpost-operative
trans-fusion of the anesthetic/surgical team were obeyed, and
criteriabasedonguidelineswereusedintheirconduct.18,19
Blood products were used during surgerywhen there was
significant bleedingthat would interfere withthe patient’s
hemodynamicstatus.Theanesthetistwassolelyresponsible
fortheuse/degreeofthebloodproduct.Post-operatively,of
necessitythehealthypatientsreceivedbloodproductswith
Hb<7g/dL,whereasthosewithcerebrovasculardisease,
coro-naryarterydisease,peripheralvasculardiseaseandchronic
pulmonaryvasculardiseasereceivedbloodtransfusionswith
Hb<8g/dL.
Accordingtotransfusioncriteria,weallocatethepatients
intotwogroups:Group1(G1)–patientswhoreceivedblood
transfusion;andGroup2(G2)–patientswhodidnotreceive
blood products. In this study population, the participants
hadameanageof58.5±13(G1=56.4andG2=15±59.5±11.8
(p=0.31). Weightand BMI ofG1 and G2, respectively, were
71.6±17.5/25.9±5.5and73.1±13.7/27.5±4.5(p>0.05).
Preop-eratively,themeanarterialpressure(MAP)was96.54mmHg
(p>0.05)for G1(93.11mmHg)and G2 (98.34mmHg)groups.
Preoperative hemoglobin for G1 and G2 was 13.5±1.5 and
13.6±1.3(p=0.91),respectively(Table1).
Patients were sorted and analyzed by SPSS 17.0
soft-ware(Chicago,IL,USA).Forcontinuousvariables,descriptive
statistics demonstrated performance characteristics
(cen-tral tendency and dispersion). By the adherence test of
Kolmogorov–Smirnov (K–S),withthe Lillieforscorrectionof
normality, the normality of data was tested. Analysis of
variance (ANOVA) for hematological curves was adopted.
Additional tests(post hoc)were conductedto evaluate
spe-cificdifferencesbetweenmeans,bypairs.Intheanalysisof
risk factors, the discrete variables were assessed byYates
chi-square test,whereas forparametric and nonparametric
continuousvariables theStudentttestand Mann–Whitney,
respectively,wereused.Inallinterpretations,thelevelof
sig-nificancewassetatp<0.05.
Results
Twenty-seven (34.6%)patients received blood transfusions:
19 (55.6%) during surgery and 12 (44.4%) post-operatively.
The average intraoperative blood loss was 458.9±205mL
(G1=540±272mL and G2=414.8±142.3mL [p=0.019]).
Mean post-operative bleeding was 238, 56±205.27mL
(G1=262.4±219.5mLandG2=218.6±175.3mL[p=0.09]).
Thecurvesofhemoglobin,hematocritandplateletsamong
Table2–Hemoglobin,hematocritandplateletvaluesamongtransfused(G1)andnottransfused(G2)patientsinfive visits(V1–V5).
Hb(g/dL) Hb(V1)(g/dL) Hb(V2)(g/dL) Hb(V3)(g/dL) Hb(V4)(g/dL) Hb(V5)(g/dL) pa
G1 13.57±1.55 11.44±1.73 9.6±1.64 10.8±1.53 12.55±1.58 >0.05
G2 13.6±1.36 11.45±1.76 10.2±1.52 11.1±1.45 12.48±1.29
Ht(%) Ht(V1)(%) Ht(V2)(%) Ht(V3)(%) Ht(V4)(%) Ht(V5)(%)
G1 38.81±4.48 32.85±5.04 27.88±4.69 31.78±4.62 36.79±4.4 >0.05
G2 40.08±4.05 33.79±4.75 30.04±4.58 33.03±4.07 36.93±3.65
Platelets(mm3) Platelets(V1)(mm3) Platelets(V2)(mm3) Platelets(V3)(mm3) Platelets(V4)(mm3) Platelets(V5)(mm3)
G1(mm3) 250.69±43.23 231.92±77.11 270.5±77.4 466.75±114.9 283.78±67.99 >0.05
G2(mm3) 245.22±66.39 215.14±77.11 286.93±83.73 476.4±170.48 266.97±105.89
a ConsideringthecurveanalysisbyANOVAandateachrespectivevisit(V1–V5)intheposthoctest.
47 46 51
50 26
1
5 26 26 27
27 N =
Visit 5 Visit 4 Visit 3 Visit 2 Visit 1
HB (Mean values)
15
14
13
12
11
10
9
8
Transfused
Yes
No
Fig.1–Laboratoryhemoglobincurveamongtransfused andnottransfusedpatients.
normaldistributionintheirgraphicalrepresentation.Forall
analysesofthecurvesbetweenG1andG2,p>0.05.Whilethe
hemoglobinandhematocritgraphicsdatafollowedaparabolic
normalcurve,theplateletcurvegeneratedagraphwith
nor-maloscillation,representedbyacurvepeakduringthevisit4.
TheirvaluesareshowninTable2andFigs.1–3.
Thepopulationriskfactors were separatelyverified. For
parametric data such as age, body weight and BMI, mean
arterialpressure(MAP)andpreoperativehemoglobin,p>0.05
47 46 51
50 26
1
5 26 26 27
27 N =
Visit 5 Visit 4 Visit 3 Visit 2 Visit 1
HT (Mean values)
50
40
30
20
Transfused
Yes
No
Fig.2–Laboratoryhematocritcurveamongtransfusedand nottransfusedpatients.
45 45 49
48 23
9
4 26 24 24
26 N =
Visit 5 Visit 4 Visit 3 Visit 2 Visit 1
Platelets (Mean values)
600
500
400
300
200
100
Transfused
Yes
No
Fig.3–Laboratoryplateletcurveamongtransfusedandnot transfusedpatients.
(Table1).Exceptforethnicity,nonparametricvariablessuch
assmoking,alcoholism,cementedornotcementedimplant,
hypertensionanddiabeteshadanimpactonratesof
transfu-sionintheiranalysis,withp>0.05(Tables1and3).Thesum
ofcomorbiditiesassociatedwithpatientsinG1hadamedian
of3(95%CI2.29–3.40),whileinG2themedianwas2(95%CI
1.90–2.61)(p=0.09)(Table1).
Discussion
Thestandardizationoftransfusionalconductsisstilla
chal-lengingtopic.Inthefirststudies,datingfromthe1940s,5the
hemoglobin valueadopted forpost-surgerycontrolof
ane-miawas10g/dL.Thislimitwaschangedintheearly1990s,
withtheexpansionofknowledgeaboutthebehaviorofacute
(traumatic andsurgical)shockand withdetailedstudiesof
the use ofblood products in patients withsevere disease.
Theguidelines then began toorient the newtransfusional
conducts,18,19eveninspecificareassuchasorthopedia.20The
hemoglobinthresholdsweremodified,from10g/dLto7g/dL
inhealthypatientsandto8g/dLinpatientswithacomorbidity
(age>65years,withrespiratorydiseaseandocclusive
vascu-lardisease).4Fromthesenumbers,anotherargument,namely,
thepossiblesubjectivecriteriathatcouldguidetheconductof
every professional,regardlessoflaboratorynumerical
anal-ysis, emerged. This can be seen in studies that generally
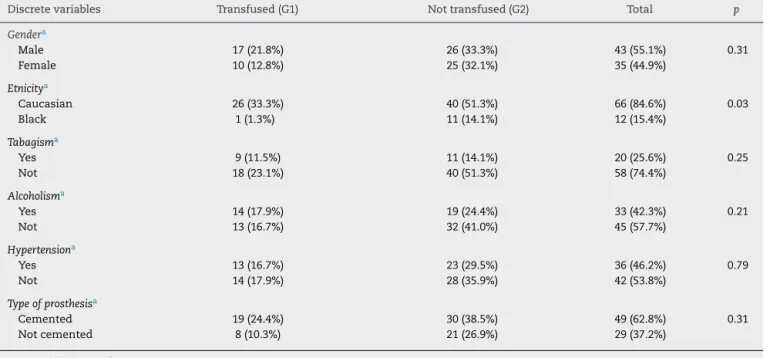
Table3–Riskfactorsamongtransfused(G1)andnottransfused(G2)patients(associationbetweendiscretequalitative variables).
Discretevariables Transfused(G1) Nottransfused(G2) Total p
Gendera
Male 17(21.8%) 26(33.3%) 43(55.1%) 0.31
Female 10(12.8%) 25(32.1%) 35(44.9%)
Etnicitya
Caucasian 26(33.3%) 40(51.3%) 66(84.6%) 0.03
Black 1(1.3%) 11(14.1%) 12(15.4%)
Tabagisma
Yes 9(11.5%) 11(14.1%) 20(25.6%) 0.25
Not 18(23.1%) 40(51.3%) 58(74.4%)
Alcoholisma
Yes 14(17.9%) 19(24.4%) 33(42.3%) 0.21
Not 13(16.7%) 32(41.0%) 45(57.7%)
Hypertensiona
Yes 13(16.7%) 23(29.5%) 36(46.2%) 0.79
Not 14(17.9%) 28(35.9%) 42(53.8%)
Typeofprosthesisa
Cemented 19(24.4%) 30(38.5%) 49(62.8%) 0.31
Notcemented 8(10.3%) 21(26.9%) 29(37.2%)
a Yateschi-squaredtest.
conducts.2,12,20 Thosestudies portrayed divergent attitudes
towardtransfusionmeasuresamongdifferentcenters,2,21and
evenamongmedicalprofessionalsofdifferentsubspecialties.
Youngetal.1demonstratedthatsurgeonshaveamore
aggres-sivetransfusionconduct,especiallywhenhemoglobinvalues
rangedfrom7g/dLto10g/dL.Inthisstudy,fromatotalof44
patientswho hadhemoglobinlevelsbetween10and7g/dL,
27werenottransfusedwithbloodproducts.Thisimpliesthat
perhapsmorerestricttransfusionalmeasuresareadoptedin
thepost-surgicalarea.Webelievethatobjectivecriteriamay
loseitspowertoinfluencethepost-operativeperiod,by
subdi-vidingtheresponsibilityfortherecoveryofthehematimetric
curvewiththeclinicofthepatientsandtheirpotentialrisk
factors.However,thissituationdoesnotoccurduring
intra-operativetransfusions,which,althoughreliablyquantifythe
necessityofbloodreplacement,18,19represented55%of
trans-fusionsinthisstudy.Thisaggressivetransfusionalattitude
isexplainedbythesituationalanddynamicmedicalconduct
determinedbyintraoperativeacuteevents.Themainreasons
fortransfusionselected bythe anesthetistswere:transient
hypotensionunresponsivetocrystalloidsandtrans-operatory
disturbances ofcardiac and respiratory rhythm caused by
transitoryshock. Itisimportantto considerthat the main
guidelines are categoricalin theirconclusions. Theydefine
thattheabsolutenumbersarenottheonlydecisivefactors
exclusivelyfortakingperioperativedecisions,18,19despitethe
tendencyofmosthealthprofessionals,towardkeepingtheir
conductbasedsolelyonlaboratoryvalues.22
Itisestimatedthatintheareaofhipreplacementsurgery
theratesofbloodtransfusionscanvarybetween33and74%of
patients.4,8Thesenumbersreinforcethefindingsofthisstudy,
inwhich34.6%ofpatientsreceivedbloodproducts,despite
theoptionforthemorerestrictivetransfusionbehaviors.This
demonstratesthattheneedforimprovementoftheseindices
remainsachallengethatisawaitingforbettersolutions.
Inordertoascertainthepossiblevariablesthatinfluence
the transfusion rates, specific studies ofblood transfusion
in elective orthopedic procedures preferred tostick to the
main transfusion criteria, risk factors and use of optional
methods,4,6,12,14–16failingtoemphasizetheimportanceofthe
behavior ofthe laboratorycurve.In thisstudy, we
demon-stratedanobjectiveapproachtothebehaviorofthecurvesof
hemoglobin,hematocritandplatelets.Asaresult,wefound
behavioralsimilaritybetweenthetwoanalyzedgroups,and
this finding answered the question of the study: patients
generally have similar recoveryspeed of the hematimetric
values, regardlessof blood transfusion.From this premise,
someassumptionsareevident.Thereisasignificantnumber
ofindividualstoleranttosurgicalbloodlossbelowthe
pre-determinedthresholdsandthesepeoplepresentasatisfactory
functionalrecoverywithoutusingbloodproducts.22
Inordertoascertainthepossiblevariablesinfluencingthe
transfusionrates,specificstudiesofbloodtransfusionin
elec-tive orthopedic procedures has been either complied with
major transfusion criteria, risk factors and use ofoptional
methods,4,6,12,14–16 and did not emphasize the importance
of the behavior of the laboratory curve. In this study, we
demonstrated anobjective approachtothe behaviorofthe
curvesofhemoglobin,hematocritandplatelets.Asaresult,
weobservedbehavioralsimilaritybetweenthetwoanalyzed
groups,andthisansweredthequestionofthestudy:patients
generallyhavesimilarrateofrecoveryfromhematimetric
val-ues,regardlessofbloodtransfusion.Fromthispremise,some
assumptionsareevident.Thereisasignificantnumberof
indi-viduals toleranttosurgicalbloodlossbelowpredetermined
thresholdsandthatpresentasatisfactoryfunctionalrecovery
withoutusingbloodproducts.22
Inelectiveorthopedicsurgeries,thereisaneedfora
min-imum level of preoperative Hb, with the variant value of
limitingrequirements.Carsonetal.23,24foundthattherewas
nobenefitinfunctionalrecoverywithmaintainingHblevels
above10g/dL,eveninsymptomaticpatients(besidesvascular
disease),comparedwiththosewhomaintainedthebasallevel
below8g/dLafterhiporthopedicsurgeries.23Hebertetal.25
foundthatearlymortalityhasnotchangedin838critically
illpatientswhoreceivedaggressivetransfusion(Hb<10g/dL),
compared with those who had more restrict transfusions
(Hb<7g/dL). Viele et al.26 analyzed patients (all of them
Jehovah’sWitnesses)whotoleratedHblevelsbelow8g/dL,26
withadequaterecoveryandpresentedpreliminarydemands
onlywhenthelevelsreachedlessthan5g/dL(inassociation
withincreasedriskofmorbidityandmortality).Theindices
of hematocrit follow a tolerance threshold for transfusion
betweenvaluesof18–25%,18 andcanreach15–20%without
myocardial damage caused by lactic acid production.
Car-diacfailureoccurswhenthethresholdsarecloseto10%.3,18
Regardingplatelets,preoperativeminimumindicesare
rele-vantwhentheyarebelow50,000mm3,acircumstanceremote
frommostpatientsundergoingelectiveTHA–whichexplains
thenullratespecificforplatelettransfusions.
Thebehavior ofhemoglobin and hematocritcurves
fol-lowedaparabolicpathwithnormaldistributionofdataanda
downwardpeakwasobservedduringthevisit3;regardlessof
transfusion,thepeakhadreturnedtothebaselinethreshold
atvisit5.Thegraphicalrepresentationofplateletswas
pecu-liar,duetothecharacteristicoscillationbetweenvisits2and
4,andrepresentedanormalizedpeakfromthevisit5,not
cor-roboratedbyanyrelevantclinicalalteration.Withrespectto
thischaracteristicbehavior,wefoundnocomparative
analy-seswithotherarthroplastystudies.
Theassessmentofriskfactorsfortransfusionisofutmost
importance,sinceitpresupposesananalysisofeach
individ-ualthat, possibly,beapredictorofnormalvariationofthe
hematimetriccurve.Consistentwiththeliterature,thisstudy
suggeststhattheriskfactorsaresynergisticandcumulative.27
Thatis,theincreaseinthenumberofcomorbiditiesofpatients
wouldprobablybethevariablewiththegreatestimpactonthe
individual’spropensitytousebloodproducts.27
Riskfactors areinvariablydiscussed perse.Preoperatory
hemoglobin(Hb),27,28<12g/dLisapredictor thatinfluenced
theAderintoandBrenke,18seriesinupto70%oftransfused
patients. In our analysis, we did not give much
consider-ationtothisimportantpredictorofrisk,because theblood
transfusionsoccurredinequalproportionsinpatientswith
Hb<12g/dL(36.4%)versusHb>12g/dL(34.3%).Itis
notewor-thy that, at randomization, anemic patients (Hb<11g/dL)
wereexcluded.ManyofthesepatientsmentionedinAderinto
andBrenkelseries,8Salidoet al.28andPola etal.27showed
hemoglobinvaluesbelow11g/dL,implyingthatpreoperative
anemiaisthedecisivefactorintheriskoftransfusion.
Thevalueof12g/dLwouldbeasafetynumberfor
perform-ingarthroplastieswithlessriskofuseofblood products.28
Otherriskfactors alreadymentioned intheliteraturewere
notcorrelatedwiththeresultsofthepresentstudy,
includ-ingadvanced age,which isassociatedwith43%ofanemia
ofchronicdisease,4 females,4,6 comorbidities (e.g., diabetes
mellitusandsystemicarterialhypertension),lowbodymass
index – lean patients (risk near 40% in patients<70kg),
shortstature,typeofanesthesiaandsurgicaltechnique.8,27
Parker et al.29 statethat post-operativeanemia shouldnot
be toleratedin elderlypatients’ recovery,giving priorityto
aggressivetransfusionconducts(inassociationwithahigher
rate offalls, cognitiveimpairment,cardiovascularrisk, and
decreased qualityoflife).Somepeculiarcharacteristicsare
relatedtomalepatientswholosemorebloodinprosthetic
pro-cedures.Women,however,toleratelessbloodlossandhavea
higherriskoftransfusion.27Theuseofpost-operativeclosed
suction,29presentsfurtherevidenceoftransfusionriskin
elec-tivearthroplasties,aswellasdemonstratinglittlebenefitin
controllinginfectionsandhematomata.29Untilnow,nostudy
discussedalcoholismandsmokingaspossibleriskfactors,as
wellasethnicity.Inourstudy,blackpeoplehadalower
ten-dencytobloodtransfusion.Belletal.6associatedprophylaxis
fordeepvenousthrombosis(DVT)withunfractionated
hep-arintoincreasedchancesoftransfusion,butwithnoreason
established.
Interestingly,Carsonetal.24andPolaetal.27were
remark-ableintheestablishmentoftransfusionalconductsinpatients
undergoingorthopedicprocedures.23,30Theseauthors
deter-mined that, initially, the use of blood products should
precede objective parameters (laboratory indices), but that
thesubjectiveparameters(clinicalandcomorbidities’
analy-sis)rationalizethepracticeoftransfusion.Withthisobjective,
theyobservedadecrease inthe percentageandamountof
transfusionwithoutadditionalrisksofmortalityand
myocar-dial infarct.30 We support this transfusion practice and,
throughourstudy,weconfirmtoothepossibilityof
improv-ing the use of blood products. Other optional methods to
avoidtransfusionmeasureswithsignificancelevelstillhave
high costs (such as recombinant erythropoietin,4), or gaps
regardingtheirpracticity.4,11,13,15
Conclusions
Therateofbloodtransfusionamongpatientstreatedwithhip
arthroplastywas34.6%.
There is a pattern of behavior of the post-operatory
hemoglobinandhematocritcurvethatfollowsaparabolawith
normaldistribution. However,theplatelet curve followsan
oscillatorypathofthenormalcurve.
Thehematimetriccurvehaslimitedreliabilitywhenused
asthesoleandabsoluteparameter.
Theclinicalandfunctionalanalysisofthepatientandofits
comorbiditiesconstitutesthebestparametertoinfluencethe
decisiontousebloodproducts,inassociationwithlaboratory
evaluation.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
2. RosencherN,KerkkampHE,MacherasG,MunueraLM, MenichellaG,BartonDM,etal.OrthopedicSurgery
TransfusionHemoglobinEuropeanOverview(OSTHEO)study: bloodmanagementinelectivekneeandhiparthroplastyin Europe.Transfusion.2003;43(4):459–69.
3. NuttallGA,StehlingLC,BeighleyCM,FaustRJ.Current transfusionpracticesofmembersoftheAmericanSocietyof Anesthesiologists:asurvey.Anesthesiology.
2003;99(6):1433–43.
4. MunozM,Garcia-ErceJA,VillarI,ThomasD.Blood
conservationstrategiesinmajororthopaedicsurgery:efficacy, safety,andEuropeanregulations.VoxSang.2009;96(1):1–13.
5. AdamsRC,LundyJS.Anesthesiaincasesofpoorsurgicalrisk: somesuggestionsfordecreasingtherisk.SurgGynecol Obstet.1942;74:1011–9.
6. BellTH,BertaD,RalleyF,MacdonaldSJ,McCaldenRW,Bourne RB,etal.Factorsaffectingperioperativebloodlossand transfusionratesinprimarytotaljointarthroplasty:a prospectiveanalysisof1642patients.CanJSurg. 2009;52(4):295–301.
7. PedersenAB,MehnertF,OvergaardS,JohnsenSP.Allogeneic bloodtransfusionandprognosisfollowingtotalhip replacement:apopulation-basedfollowupstudy.BMC MusculoskeletDisord.2009;10:167.
8. AderintoJ,BrenkelIJ.Pre-operativepredictorsofthe requirementforbloodtransfusionfollowingtotalhip replacement.JBoneJointSurgBr.2004;86(7):970–3.
9. SturdeeSW,BeardDJ.Astrategyforreducing
blood-transfusionrequirementsinelectiveorthopaedic surgery.JBoneJointSurgBr.2004;86(3):464.
10.BoothD,KothmannE,TidmarshM.Astrategyforreducing blood-transfusionrequirementsinelectiveorthopaedic surgery.JBoneJointSurgBr.2004;86(2):309–10.
11.HelmAT,KarskiMT,ParsonsSJ,SampathJS,BaleRS.A strategyforreducingblood-transfusionrequirementsin electiveorthopaedicsurgery.Auditofanalgorithmfor arthroplastyofthelowerlimbJBoneJointSurgBr. 2003;85(4):484–9.
12.CarlessPA,HenryDA,CarsonJL,HebertPP,McClellandB,Ker K.Transfusionthresholdsandotherstrategiesforguiding allogeneicredbloodcelltransfusion.CochraneDatabaseSyst Rev.2010;10:CD002042.
13.CouvretC,TricocheS,BaudA,DaboB,BuchetS,PaludM, etal.Thereductionofpreoperativeautologousblood donationforprimarytotalhiporkneearthroplasty:theeffect onsubsequenttransfusionrates.AnesthAnalg.
2002;94(4):815–23.
14.FeaganBG,WongCJ,KirkleyA,JohnstonDW,SmithFC, WhitsittP,etal.Erythropoietinwithironsupplementationto preventallogeneicbloodtransfusionintotalhipjoint arthroplasty.Arandomized,controlledtrial.AnnInternMed. 2000;133(11):845–54.
15.Gonzalez-PorrasJR,ColadoE,CondeMP,LopezT,NietoMJ, CorralM.Anindividualizedpre-operativebloodsaving protocolcanincreasepre-operativehaemoglobinlevelsand reducetheneedfortransfusioninelectivetotalhiporknee arthroplasty.TransfusMed.2009;19(1):35–42.
16.HoKM,IsmailH.Useofintravenoustranexamicacidto reduceallogeneicbloodtransfusionintotalhipandknee arthroplasty:ameta-analysis.AnaesthIntensiveCare. 2003;31(5):529–37.
17.YamamotoK,ImakiireA,MasaokaT,ShinmuraK.Autologous bloodtransfusionintotalhiparthroplasty.JOrthopSurg (HongKong).2004;12(2):145–52.
18.Practiceguidelinesforbloodcomponenttherapy:areportby theAmericanSocietyofAnesthesiologistsTaskForceon BloodComponentTherapy.Anesthesiology.1996;84(3):732–47.
19.MurphyMF,WallingtonTB,KelseyP,BoultonF,BruceM, CohenH,etal.Guidelinesfortheclinicaluseofredcell transfusions.BrJHaematol.2001;113(1):24–31.
20.FeaganBG,WongCJ,LauCY,WheelerSL,SueAQG,KirkleyA. Transfusionpracticeinelectiveorthopaedicsurgery.Transfus Med.2001;11(2):87–95.
21.BoralessaH,GoldhillDR,TuckerK,MortimerAJ,Grant-Casey J.Nationalcomparativeauditofblooduseinelectiveprimary unilateraltotalhipreplacementsurgeryintheUK.AnnRColl SurgEngl.2009;91(7):599–605.
22.Vuille-LessardE,BoudreaultD,GirardF,RuelM,ChagnonM, HardyJF.Redbloodcelltransfusionpracticeinelective orthopedicsurgery:amulticentercohortstudy.Transfusion. 2010;50(10):2117–24.
23.CarsonJL,TerrinML,BartonFB,AaronR,GreenburgAG,Heck DA,etal.Apilotrandomizedtrialcomparingsymptomaticvs. hemoglobin-level-drivenredbloodcelltransfusionsfollowing hipfracture.Transfusion.1998;38(6):522–9.
24.CarsonJL,TerrinML,NoveckH,SandersDW,ChaitmanBR, RhoadsGG,etal.Liberalorrestrictivetransfusioninhigh-risk patientsafterhipsurgery.NEnglJMed.2011;365(26):2453–62.
25.HebertPC,WellsG,BlajchmanMA,MarshallJ,MartinC, PagliarelloG,etal.Amulticenter,randomized,controlled clinicaltrialoftransfusionrequirementsincriticalcare. TransfusionRequirementsinCriticalCareInvestigators, CanadianCriticalCareTrialsGroup.NEnglJMed. 1999;340(6):409–17.
26.VieleMK,WeiskopfRB.Whatcanwelearnabouttheneedfor transfusionfrompatientswhorefuseblood?Theexperience withJehovah’sWitnesses.Transfusion.1994;34(5):396–401.
27.PolaE,PapaleoP,SantoliquidoA,GaspariniG,AulisaL,De SantisE.Clinicalfactorsassociatedwithanincreasedriskof perioperativebloodtransfusioninnonanemicpatients undergoingtotalhiparthroplasty.JBoneJointSurgAm. 2004;86-A(1):57–61.
28.SalidoJA,MarinLA,GomezLA,ZorrillaP,MartinezC. Preoperativehemoglobinlevelsandtheneedfortransfusion afterprosthetichipandkneesurgery:analysisofpredictive factors.JBoneJointSurgAm.2002;84-A(2):216–20.
29.ParkerMJ,RobertsCP,HayD.Closedsuctiondrainageforhip andkneearthroplasty.Ameta-analysis.JBoneJointSurgAm. 2004;86(6):1146–52.
30.GroverM,TalwalkarS,CasbardA,BoralessaH,ContrerasM, BrettS,etal.Silentmyocardialischaemiaandhaemoglobin concentration:arandomizedcontrolledtrialoftransfusion strategyinlowerlimbarthroplasty.VoxSang.