OPI N I ON S OF THE STAFF AN D USERS ABOUT THE QUALI TY OF THE MEN TAL HEALTH
CARE DELI VERED AT A FAMI LY HEALTH PROGRAM
Mar ik o Koga1 Ant onia Regina Fer r eir a Fur egat o2 Jair Licio Fer r eir a Sant os3
Koga M, Fur egat o ARF, Sant os JLF. Opinions of t he st aff and user s about t he qualit y of t he m ent al healt h car e deliv er ed at a fam ily healt h pr ogr am . Rev Lat ino- am Enfer m agem 2006 m ar ço- abr il; 14( 2) : 163- 9.
Au t h or s aim ed at lear n in g abou t t h e m en t al h ealt h car e pr ov ided at a Fam ily Healt h Pr ogr am . 1 4 2 subj ect s w er e int er view ed ( 18 nur ses, 78 agent s, 17 pat ient s and 29 fam ily m em ber s) . I n or der t o collect dat a, aut hor s used t he Scale of Opinion on Ment al Healt h Car e w it h 25 st at em ent s on t he car e, or ient at ion by t he m em ber s of t he Pr ogr am of Fam ily Healt h t eam and t he benefit s of t his Pr ogr am . The t ot al scor es show ed a differ ence bet w een t he agent s and ot her gr oups. Am ong nur ses, t hey found t he shor t er dev iat ion and am ong t h e pat ien t s t h e gr eat er v ar iabilit y in t h e r espon ses. Th ey em ph asize t h e n eed for efficacy in ar r an gin g t h e appoint m ent s. Aut hor s found a lack of coher ence am ong t he opinions of t he subj ect s r egar ding t he pr ofessionals’ or ien t at ion s.
DESCRI PTORS: fam ily healt h pr ogr am ; psy chiat r ic nur sing; scales
OPI NI ONES DEL EQUI PO Y USUARI OS SOBRE LA ATENCI ÓN A LA SALUD MENTAL EN UN
PROGRAMA DE SALUD DE LA FAMÍ LI A
El pr esent e t r abaj o t uvo com o obj et ivo conocer la at ención a la salud m ent al en un Pr ogr am a de Salud de la Fam ília. Fu er on en t r ev ist ados 1 4 2 su j et os ( 1 8 en fer m er as, 7 8 agen t es, 1 7 pacien t es y 2 9 fam iliar es) . Par a la colect a de dat os se ut ilizó la Escala de Opinión sobr e At ención a la Salud Ment al con 25 afir m aciones sobr e asist encia, or ient ación del equipo del PSF y benefícios de est e Pr ogr am a. Los escor es t ot ales dem ost r ar on m ay or dif er en cia en t r e los agen t es y dem ás gr u pos. En t r e las en f er m er as se en con t r ar ó el m en or desv io y ent r e los pacient es la m ay or v ar iabilidad en las r espuest as. Dest aque m ay or par a la eficaz m aner a de m ar car las consult as. Hubier on ev idencias de incoer encia ent r e las opiniones de los suj et os cuant o a las or ient aciones de los pr of esion ales.
DESCRI PTORES: pr ogr am a salud de la fam ilia; enfer m er ía psiquiát r ica; escalas
OPI N I ÕES DA EQUI PE E USUÁRI OS SOBRE A ATEN ÇÃO À SAÚDE MEN TAL N UM
PROGRAMA DE SAÚDE DA FAMÍ LI A
Obj et iv ou - se con h ecer a at en ção à saú de m en t al n u m Pr ogr am a de Saú de da Fam ília ( PSF) . For am en t r ev ist ados 1 4 2 su j eit os ( 1 8 en fer m eir as, 7 8 agen t es, 1 7 pacien t es e 2 9 fam iliar es) . Na colet a de dados, ut ilizou- se a Escala de Opinião sobr e At enção à Saúde Ment al, com 25 afir m at ivas sobr e assist ência, or ient ação d a eq u ip e d o PSF e b en ef ícios d esse Pr og r am a. Os escor es t ot ais d em on st r ar am m aior d if er en ça en t r e os ag en t es e d em ais g r u p os. En t r e as en f er m eir as en con t r a- se o m en or d esv io e en t r e os p acien t es a m aior var iabilidade nas r espost as. Dest aca- se m aior eficácia no agendam ent o das consult as. Evidenciou- se incoer ência ent r e opiniões dos suj eit os quant o às or ient ações dos pr ofissionais.
DESCRI TORES: pr ogr am a saú de da fam ília; en fer m agem psiqu iát r ica; escalas
1
PhD, Pr ofessor, Mar ingá St at e Univer sit y - UEM, e- m ail: m ar yparana77@hot m ail.com ; 2 Full Pr ofessor, Univer sit y of São Paulo at Ribeir ão Pr et o College of Nur sing, WHO Collaborat ing Cent r e for Nur sing Resear ch Developm ent , e- m ail: fur egat o@eer p.usp.br ; 3 Full Pr ofessor, Univer sit y of São Paulo at Ribeir ão Pr et o Medical School
I NTRODUCTI ON
D
esp it e in f lu en ce f r om p sy ch iat r ic r ef or m p r in cip les, t h e asy lu m car e sy st em st ill p er sist s inBr azil.
Th e g r a d u a l i m p l a n t a t i o n o f e t h i c a l a n d
r esponsible psychiat r y aim s t o pr om ot e m ent al healt h,
i d en t i f y a n d g i v e a d eq u a t e t r eat m en t t o ca ses o f
d i se a se a n d t a k e ca r e o f ch r o n i ca l l y - i l l p a t i e n t s’
r e h a b i l i t a t i o n , u s i n g n e w d e v i c e s ( d a y h o s p i t a l ,
hospit alizat ion in a gener al hospit al, out pat ient clinic,
Psy ch osocial Car e Cen t er - CAPS, Psy ch osocial Car e
Gr oup - NAPS, pensions) and com pet ent pr ofessionals
w ho ident ify w it h t his new pr oposal.
Th ese con t r ast s r ev eal t h at m an y d ecad es
hav e passed for t he r efor m m ov em ent t o becom e a
r ealit y and be par t of t he new healt h syst em , adopt ing
pr event ivist concept ions, subst it ut ing asylum by open
t r eat m ent , st im ulat ing t he offer ing of et hical car e in
r esp ect of p at ien t s w it h p sy ch iat r ic d isor d er s. As a
r esu lt , bu dget s of t h e Healt h Min ist r y an d Br azilian
cit ies hav e been dist r ibut ed differ ent ly.
Now aday s, t h e pr esen ce of m en t al pat ien t s
at hom e is a r ealit y, w het her due t o cr it er ia t hat m ake
r an dom h ospit alizat ion s m or e difficu lt or du e t o t h e
exist ence of out pat ient clinics, NAPS and CAPS, w hich
a l l o w f o r t r e a t m e n t w i t h o u t u n n e c e s s a r y
h o sp i t al i zat i o n s. Mo r eov er, t r eat m en t s u si n g m o r e
ef f icien t d r u g s w it h less collat er al ef f ect s f acilit at e
pat ient s’ adherence t o t reat m ent and social insert ion.
How ev er, h ow h av e r elat iv es been liv in g at
hom e w it h m ent al pat ient s w ho are no longer confined
t o m ent al inst it ut ions?
K o g a a n d Fu r e g a t o e x a m i n e d h o w
sch izop h r en ic p at ien t s liv e w it h t h eir r elat iv es an d
concluded t hat relat ives live w it h an overload in t erm s
of f in an ce as w ell as dom est ic r ou t in e an d ph y sical
and/ or em ot ional disease. This st udy w as r eplicat ed
an d f ou n d v ar iou s f act or s of ov er load t h at en t ailed
alt er at ion s in per son al lif e an d in f am ily an d social
i n t e r a c t i o n s( 1 ). A n o t h e r s t u d y( 2 ) e v i d e n c e d t h a t
r elat ives adapt and r eor ganize t hem selves t o w elcom e
t he ill per son and m inim ize dam age.
B e s i d e s t h e p o s i t i v e r e f l e x e s o f t h e
psy chiat r ic r efor m( 3), w e ar e now faced w it h anot her
f av or ab le sit u at ion , w h ich is t h e cr eat ion of Fam ily
Healt h Pr ogr am s ( FHP) .
Th e m u n icipalizat ion of h ealt h m an agem en t and social cont r ol encour ages t he ex pansion of ex t r a
h osp it al act ion s an d p r ior it izes t h e or g an izat ion of pr act ices aim ed at car e deliv er y t o f am ilies in t h eir
s o c i a l s p a c e , a s a h e a l t h c a r e f o c u s , i n c l u d i n g d i f f e r e n t i a t e d a n d g u a r a n t e ed f i n a n ci a l t r a n sf er s,
t hr ough t he adopt ion of t he Com m unit y Healt h Agent Pr ogr am – CHAP and FHP in Br azilian cit ies( 4).
Basic FHP unit s should be able t o solve 85%
o f h eal t h p r o b l em s i n t h ei r co m m u n i t y, d el i v er i n g q u a l i t y c a r e , p r e v e n t i n g d i s e a s e s , a v o i d i n g
u n n e c e s s a r y h o s p i t a l i z a t i o n s a n d i m p r o v i n g t h e populat ion’s qualit y of life.
A s t e a c h e r s , w e a r e f a c i n g v a r i o u s confront at ions w it h realit y, t hat is, once again, pract ice pr ovides us w it h plent y of t eaching m at er ial and, fr om
t eaching, w e r et ur n t o pr act ice w it h ex per ience and
cr i t i ci sm . Tr a i n i n g ce n t e r s a f f i l i a t e d w i t h co l l e g e s ou t lin e t h is obj ect iv e, w h ich st im u lat es discu ssion s. I n d i sco u r se, at t em p t s ar e m ad e t o el i m i n at e t h e
dichot om y bet w een m ind and body.
The im plant at ion of t he FHP in Mar ingá, w it h
5 7 f am ily h ealt h t eam s w or k in g at 2 4 Basic Healt h Unit s, m akes us quest ion w het her m ent al pat ient s and
t heir r elat ives have been r eceiving som e t ype of car e or guidance aft er t he im plant at ion of t his healt h care st r at eg y.
OBJECTI VE
Get t o k now and analy ze m ent al healt h car e in t he Fam ily Healt h Car e Pr ogram of Mar ingá, t hr ough
t he opinions of nurses, com m unit y agent s, psychiat ric pat ient s and t heir r elat iv es.
METHODOLOGY
St u dy con t ex t
Mar in g á is a cit y w it h 2 8 8 , 4 6 5 in h ab it an t s
locat ed in t he Nor t hw est of Par aná St at e, Br azil. The ci t y co n st i t u t e s t h e 1 5 t h Re g i o n a l He a l t h Ce n t e r,
including 30 cit ies, w hich is fully m anaged by t he SUS – Si n g l e H e a l t h Sy st e m . Th e m u n i ci p a l n e t w o r k consist s of 20 Healt h Unit s ( HU) , one Mixed Unit , one
Th e an aly sis of dif f er en ces an d w eak n esses
in m ent al healt h car e deliver ed by t he FHP t eam s w as t heor et ically suppor t ed by lit erat ur e about t he Fam ily
Healt h Pr og r am an d Psy ch iat r ic Ref or m , as w ell as
b y k n o w l e d g e o n Psy ch i a t r i c Nu r si n g a n d Me n t a l
Healt h .
RESULTS AND DI SCUSSI ON
S t u d y p a r t i c i p a n t s w e r e 1 8 n u r s e s , 7 8
com m u n it y ag en t s, 1 7 p sy ch iat r ic p at ien t s an d 2 9
r elat iv es of pat ient s, t ot aling 142 subj ect s.
The 18 nur ses w er e bet w een 25 and 47 year s old an d m ost of t h em ( 7 2 % ) w er e g r ad u at ed f r om
Mar in gá St at e Un iv er sit y. Com m u n it y h ealt h agen t s
( 78) w er e bet w een 20 and 56 year s old. Only t w o of
t h em p ossessed a h ig h er ed u cat ion d eg r ee an d 3 4
h ad f i n i sh ed seco n d ar y ed u cat i o n . Rel at i v es’ ag es r anged fr om 20 t o 74 year s. They w er e m ost ly w om en
( 8 3 % ) a n d t h e i r e d u ca t i o n l e v e l v a r i e d b e t w e e n
illit er acy ( 3 1 % ) an d h igh er edu cat ion ( 6 % ) . Th e 1 7 pat ient s w er e bet w een 21 and 70 y ear s old. Nine of
t h e m w e r e w o m e n a n d o n l y t h r e e h a d co n t i n u e d
st udy ing aft er basic educat ion.
Gener al t est r esult s
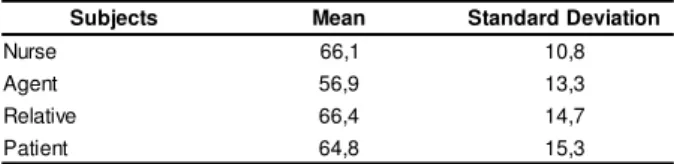
Tot al scor es for each gr oup r ev ealed gr eat er
difference bet ween agent s’ answers and ot her groups,
wit h relat ives and nurses obt aining pract ically t he sam e scor es. Nur ses’ answ er s show ed less dev iat ion, t hat
is, great er hom ogeneit y am ong answers, while pat ient s’
answ er s r ev ealed gr eat er var iabilit y ( Table 1) .
Table 1 – Mean t ot al scor es and st andar d dev iat ions
of 4 subj ect gr oups Su b j ect s
I n t h e 2 0 H e a l t h U n i t s , 1 8 FH P n u r s e s accept ed t o par t icipat e in t his st udy. The 78 com m unit y agen t s w h o par t icipat ed w er e m em ber s of t h ese 1 8 nur ses’ t eam s. The sam e nur ses indicat ed 17 m ent al pat ient s and 29 r elat iv es, t ot aling 142 subj ect s.
I n st r u m en t s
We c o n s t r u c t e d a n i n s t r u m e n t w i t h 2 5 affir m at iv e st at em ent s t hat focused on t he car e and guidance offer ed by t he FHP t eam s, as w ell as on t he benefit s of t his car e.
Th is Lik er t - t y p e in st r u m en t w as called t h e Op i n i o n Sca l e o n Me n t a l He a l t h Ca r e i n t h e FHP ( EO A S M / PS F) , i n a c c o r d a n c e w i t h s t u d i e s o n psy chom et r ic scales and quest ionnair es. Fiv e opt ions w er e of f er ed f or each st at em en t : Yes, Fr eq u en t ly, Som et im es, Rar ely an d No.
The int r oduct ion t o t he EOASM/ PSF inst r um ent c o n t a i n s q u e s t i o n s t o i d e n t i f y t h e s u b j e c t a n d cont ex t ual infor m at ion about m ent al illness.
Et h ical Aspect s
Th e p r o j e ct w a s a p p r o v e d b y t h e e t h i cs com m it t ee ( COPEP) . Each subj ect w as duly infor m ed, agr eed t o par t icipat e and signed t he consent t er m .
Dat a Collect ion
Nur ses and agent s w ho agr eed t o par t icipat e w e r e i n t e r v i e w e d a n d a n sw e r e d t h e t e st s i n t h e pr esen ce of t h e r esear ch er s.
Ag e n t s w e r e a sk e d t o i n d i ca t e a m e n t a l p at ien t w it h t y p ical b eh av ior ( an x iet y, d ep r ession , aggr essiv eness, incoher ence, st r ange at t it udes) and/ or t ak ing psy chot r opic dr ugs ( obser v ing black label) , excluding alcohol and drugs user s. They also indicat ed a r elat iv e ( pr efer ably t h e car egiv er ) .
At pat ient s’ hom es, t he r esear cher s r ead out t he quest ions and st at em ent s t o pat ient s and r elat ives and filled out t he for m s.
An aly sis Pr oced u r es
The Kruskal-Wallis t est w as used for st at ist ical t r eat m ent of dat a, w hich allow ed t he r esear cher s t o com par e t he nur ses’, agent s’, pat ient s’ and r elat ives’ op in ion s.
s t c e j b u
S Mean StandardDeviation
e s r u
N 66,1 10,8
t n e g
A 56,9 13,3
e v it a l e
R 66,4 14,7
t n e it a
P 64,8 15,3
The Kruskal- Wallis t est for independent group
com par ison s pr odu ced a Ch i- squ ar e v alu e of 1 3 . 6 4 . Wit h 3 degr ees of fr eedom , t he pr obabilit y t hat equal
or higher values w ould occur cor r esponded t o 0.0034,
concluding t hat scor es v ar ied significant ly am ong t he
Ag en t s st ood ou t in com p ar ison w it h ot h er
g r o u p s . N u r s e s ’ a n s w e r s r e v e a l e d g r e a t e r
hom ogeneit y, pr obably due t o t he specific for m at ion
t hey ar e subm it t ed t o at under gr aduat e level. Gr eat er
d isp er sion w as f ou n d am on g p at ien t s, p er h ap s d u e
t o disease sy m pt om s.
I n v iew of t h ese r esu lt s ( p< 0 . 0 0 3 4 ) , w h ich
indicat e significant variat ions in scores am ong different
gr oups, r esear cher s decided t o analy ze each subj ect
g r ou p ’s an sw er s sep ar at ely.
Com par at iv e Analy sis of Answ er s per Subj ect Gr oup
Th e su m s an d f r eq u en cies of each g r ou p ’s
answ er s t o t he 5 opt ions ( Yes, Fr equent ly, Som et im es,
Rar el y an d No ) w er e an al y zed f o r each o f t h e 2 5
st at em ent s. Next , t he m ost significant differ ences ar e
highlight ed, based on lit er at ur e.
- Car e r equest ed fr om FHP t eam
Most pr ofessionals m ent ioned t hey at t ended
t h e clien t s. I n t u r n , clien t s in d icat ed t h ey r eceiv ed
car e w hen t hey needed t he FHP t eam s’ help.
At t he Basic Healt h Unit s, w e obser ved client s’
f r ee access w h en t h ey r eq u est ed car e f r om t h ese
t eam s. Their r equest s w er e r eadily at t ended t o, w hich
r eveals t he accessibilit y of t he FHP, as ex pect ed.
- Or ient at ion on m edicat ion effect s
Nurses have num erous responsibilit ies in care
deliver y t o client s t aking psychot r opic dr ugs. The use
of t his kind of m edicat ion has radically changed m ent al
illn ess t r eat m en t , b ot h in an d ou t sid e t h e h osp it al
co n t ex t( 5 ). Th i s a l l o w e d so m e f a m i l y m e m b e r s t o
m aint ain t heir r elat ives at hom e. Mor eov er, m ent
ally-i l l p a t ally-i e n t s w e r e a b l e t o r e co v e r t h e ally-i r j o b s a n d
pr oduct ive life in t he com m unit y.
W h e n p a t i e n t s s t a r t p s y c h o t r o p i c d r u g s
t reat m ent , nurses are responsible for m onit oring t heir
ph y siological r espon ses an d ot h er r eact ion s. Hen ce,
t hey hav e t o m ast er k now ledge about indicat ions for
u sin g t h is m edicat ion an d desir ed ef f ect s, collat er al
effect s, adverse or t oxic effect s and cont r aindicat ions.
They also have t o know about adequat e behavior and
car e needed for each case.
I t is im por t ant for nur ses t o help pat ient s t o
p er cei v e t h em sel v es as act i v e p ar t i ci p an t s i n t h i s
p r ocess, assu m in g t h e r esp on sib ilit y t o accom p lish
t r eat m en t .
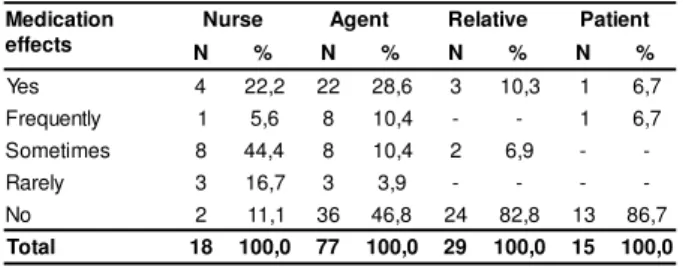
Table 2 – Answ er s about or ient at ions r elat ed t o t he
effect s of psy chiat r ic dr ugs per subj ect gr oup
n o i t a c i d e M s t c e f f e e s r u
N Agent Relative Patient
N % N % N % N %
s e
Y 4 22,2 22 28,6 3 10,3 1 6,7 y lt n e u q e r
F 1 5,6 8 10,4 - - 1 6,7
s e m it e m o
S 8 44,4 8 10,4 2 6,9 - -y
l e r a
R 3 16,7 3 3,9 - - -
-o
N 2 11,1 36 46,8 24 82,8 13 86,7
l a t o
T 18 100,0 77 100,0 29 100,0 15 100,0
No answ er = Agent 1, Pat ient 2
Tab le 2 sh ow s t h at r elat iv es, p at ien t s an d ag en t s in d icat ed t h at t h ey d id n ot ag r ee w it h t h e st a t e m e n t a b o u t r e ce i v i n g o r i e n t a t i o n s o n d r u g s ef f ect s. Th i s i s a st r o n g si g n t h at ag en t s ar e n o t pr epar ed t o pr ovide t his kind of clar ificat ions and t hat clien t s ar e n ot r eceiv in g gu idan ce abou t psy ch iat r ic m edicat ion use by FHP t eam s. Nur ses and physicians ar e som e of t he pr ofessionals pr epar ed t o offer t his car e. All t eam s in t er v iew ed in t h is st u dy in clu ded a nurse, but not all of t hem included a physician. Som e n u r ses ( 8 o u t o f 1 8 i n t er v i ew ees) an sw er ed t h at , s o m e t i m e s , t h e y p r o v i d e i n f o r m a t i o n a b o u t t h e e x p e c t e d a n d c o l l a t e r a l e f f e c t s o f p s y c h i a t r i c m ed icat ion .
- Clar ificat ions t o r elat iv es of m ent al pat ient s Most of t h e FHP clien t s an sw er ed t h at t h ey did not r eceiv e clar ificat ions about liv ing w it h m ent al i l l n e ss. An sw e r s r e v e a l e d d i sp a r i t i e s. Fe w n u r se s indicat ed t hat t hey offer guidance alw ays ( 11.1% ) or f r eq u en t ly ( 2 7 . 8 % ) . Th ese r at es in cr eased t o 5 0 % am on g ag en t s. Th is d ef icien cy in car e is p er ceiv ed by r elat ives ( 72.4% ) , as show n in Table 3.
Tab le 3 – An sw er s ab ou t FHP t eam or ien t at ion s t o r elat iv es per subj ect gr oup
o t s n o i t a t n e i r O s e v i t a l e r e s r u
N Agent Relative Patient
N % N % N % N %
s e
Y 2 11,1 33 42,3 5 17,2 5 31,3 y lt n e u q e r
F 5 27,8 6 7,7 2 6,9 - -s e m it e m o
S 4 22,2 19 24,4 - - 1 6,3 y
l e r a
R 6 33,3 4 5,1 1 3,5 - -o
N 1 5,6 16 20,5 21 72,4 10 62,5
l a t o
T 18 100,0 78 100,0 29 100,0 16 100,0
No answ er = Pat ient 1
a n d a ct i v e p a r t i ci p a t i o n . Li t e r a t u r e m e n t i o n s t h e cont inuat ion of high ( m edicat ion and psy chot her apy ) t reat m ent abandonm ent and rehospit alizat ion rat es( 6- 7). - Tr eat m ent concept for m ent al healt h - hospit alizat ion
Psy ch iat r ic h ospit als st ill ex ist s t o absor b a p o p u l a t i o n o f n o n - ci t i ze n s, u si n g t e ch n i q u e s t h a t “ sh ou ld ” lead t o h ealt h r ecov er y an d socializat ion . Mor eover, t hey ser ve t o pr ot ect societ y and safeguar d u n p r od u ct iv e p er son s.
I n ou r en v ir on m en t , t h e op en d oor of t h e p sy ch i a t r i c h o sp i t a l i s n o t a i m l e ss. Th i s h a p p e n s because, t he higher t he num ber of pat ient s, t he gr eat er t h e q u a n t i t y o f d a i l y a l l o w a n ce s ( h o sp i t a l i za t i o n aut hor izat ions - AI Hs) . This ent ails higher pr ofit s for t h e in st it u t ion an d f or cer t ain p r of ession als, w h ose r em unerat ion st ill depends on t he num ber of pat ient s t hey at t end. This sy st em st r uct ur e im pair s r efor m ist in t en t ion s an d access t o h ospit alizat ion ser v ices by pat ient s w it h acut e m anifest at ions of illness.
I n Br azil, ev en befor e Law No 10. 216/ 2001, t h e d e i n st i t u t i o n a l i za t i o n o f m e n t a l p a t i e n t s w a s alr eady u n der discu ssion . Not con st r u ct in g h ospit als and decr easing t he num ber of psychiat r ic beds m eans ch oosin g ot h er f or m s of t r eat m en t f or t h e m en t ally i l l . Th u s , t h e a i m o f h o s p i t a l i z a t i o n b e c o m e s specialized, specific and shor t - t er m t r eat m ent( 8).
Th e d e co n st r u ct i o n o f m e n t a l i n st i t u t i o n infr ast r uct ur e and of w ay s of t hink ing and act ing in p sy ch i a t r y su g g e st t h e co n st r u ct i o n o f i d e a s a n d innov at ions in m ent al healt h car e. They also suggest t h e decon st r u ct ion of t h e in t er n al m en t al in st it u t ion infrast ruct ure, t hat is, w hat is inside each professional, like in t he case of nurses w ho learned t o t ake care of m ent al pat ient s only inside closed inst it ut ions( 9).
I n v iew of det er m inat ions by t he Minist r y of Healt h t o at t end m ent al pat ient s not only in sanat oria, b u t a l so i n CAPS, o u t p a t i e n t cl i n i cs a n d g e n e r a l h ospit als, t h e r esear ch er s ex pect ed in t er v iew ees t o in dicat e t h at t r eat m en t of m en t al illn ess can n ot be r est r ict ed t o hospit alizat ion. How ev er, r esult s show ed t h at abou t 7 0 % of n u r ses st ill do n ot h av e a clear opinion on t he im por t ance of ot her t r eat m ent s.
Alt er nat iv e com m unit y ser v ices t o subst it ut e f o r h o s p i t a l i z a t i o n , a l t h o u g h e s s e n t i a l f o r t h e d e h o s p i t a l i z a t i o n p r o c e s s a n d t o l e g i t i m i z e t h e d ein st it u t ion alizat ion m od el, ar e slow ly b ecom in g a r ealit y. Cases of r ev olv in g d oor s, in w h ich p at ien t s ar e dischar ged but successiv ely r ehospit alized in t he sam e or in ot her hospit als st ill exist , as w ell as a lack o f p r e p a r a t i o n f o r p a t i e n t s , f a m i l i e s a n d h e a l t h p r of ession als.
- The FHP facilit at es appoint m ent scheduling
Alt hough gr oup answ er s v ar ied, m ost agent s ( 60.9% ) , r elat ives ( 75% ) and pat ient s ( 70.6% ) agr eed t h at t h e im plan t at ion of t h e Fam ily Healt h Pr ogr am
f acilit at ed ap p oin t m en t sch ed u lin g at Basic Healt h Unit s. On t he ot her hand, only 44.4% of nur ses agr eed w i t h t h i s st a t e m e n t . So m e r e l a t i v e s co n f i r m e d a
sign if ican t im pr ov em en t in t h is r espect , as t h ey n o longer had t o go t o t he Basic Healt h Unit early in t he m or ning t o schedule an appoint m ent . This aspect has
been considered as one of t he m ost visible effect s of FHP im plant at ion in Mar ingá.
- The need for hospit alizat ion and it s relat ion w it h t he
FHP
Clien t s w er e accu st om ed t o h ospit alizat ion s i n ca se o f e p i so d e s o f m e n t a l d i se a se a n d o t h e r
sit uat ions of dist ur bance or aggr essiv eness. I n ot her w or ds, t he door of t he psychiat r ic hospit al w as alw ays open for h ospit alizat ion . As a r esu lt of Decr ee 2 2 4 /
92, t he num ber of beds and hospit alizat ion t im es have been gr adually decr easing. This condit ion is r eflect ed b y t h e a n s w e r s s h o w n i n Ta b l e 4 . Th i s k i n d o f
r esolut ions gained st r engt h w hen Law No 10.216/ 2001 w as appr ov ed, w hich pr oposes a gr adual decr ease in beds and t he cr eat ion of ot her t r eat m ent alt er nat ives,
st im ulat ing j udicious hospit alizat ions.
Table 4 – Answ er s about ot her help r esour ces in t he
FHP per subj ect gr oup
No answ er = Agent 6, Pat ient 1
As t o t he num ber of hospit alizat ions, 43.8% of nur ses affir m ed t hat t her e w as no decr ease, 40.6% of agent s indicat ed an act ual decr ease and t he sam e q u an t i t y sai d t h at t h er e w as n o d ecr ease. Men t al pat ien t s an d fam ily m em ber s con fir m ed a r edu ct ion in hospit alizat ions ( 88. 9% and 73. 7% , r espect iv ely ) . Th e r esear ch er s qu est ion w h et h er t h is dif f er en ce in opinions is a sign of professionals’ lack of know ledge. Legislation on m ental disorder treatm ents is going t h r o u g h g r ea t t r a n sf o r m a t i o n s, w h i ch a r e sl o w l y introduced in Brazil. This has given rise to a 25% decrease in the num ber of psychiatric hospitals since 1981(10).
p l e H
s e c r u o s e R
e s r u
N Agent Relative Patient
N % N % N % N %
s e
Y 3 16,7 38 52,8 6 20,7 3 18,8
y l t n e u q e r
F 2 11,1 2 2,8 1 3,4 -
-s e m i t e m o
S 5 27,8 12 16,7 3 10,3 -
-y l e r a
R 2 11,1 2 2,8 - - -
-o
N 6 33,3 18 25,0 19 65,5 13 81,3
l a t o
Th e r ed u ct ion in t h e n u m b er of p sy ch iat r ic beds poin t s t ow ar ds t h e n eed t o con solidat e a n ew int erdisciplinary approach in m ent al healt h care. St at e an d Mu n icipal Men t al Healt h Coor din at ion Un it s ar e im plant ing t his k ind of appr oach at t he NAPS, CAPS an d ou t p at ien t clin ics cr eat ed in t h e Sin g le Healt h Syst em ( SUS) , pr oposing t he pr ogr essive subst it ut ion of t r eat m ent in m ent al inst it ut ions by m or e effect iv e alt er nat iv es at a low er social cost .
Anot her fr equent st r at egy is t he inclusion of b ed s i n g en er al h o sp i t al s an d t h e cr eat i o n o f d ay h ospit als, besides em er gen cy ser v ices in t egr at ed in t h e h e a l t h sy st e m i n d i f f e r e n t p l a ce s a cr o ss t h e cou n t r y.
Pr o g r e ssi v e r e so ci a l i z a t i o n p r o g r a m s a r e bein g offer ed t o ch r on ic pat ien t s w h o can n ot r et u r n t o t h ei r f a m i l i es o f o r i g i n , w i t h d i f f er en t o p t i o n s, including shelt er s and pr ot ect ed pensions( 11).
Psy ch i a t r i c h o sp i t a l i za t i o n i s r e st r i ct e d t o ser iou s cases, n eed in g t em p or ar y com m it m en t an d i n t en se m ed i cat i o n i n t er v en t i o n f o r r ev er si o n an d con t r ol. Th is r equ ir es m oder n an d ef f icien t ser v ices w it h sp ecialized t eam s, con v in ced of t h e ef f icien cy ideal t o allow indiv iduals t o r et ur n hom e as soon as p o s s i b l e a n d c o n t i n u e p a r t i c i p a t i n g a c t i v e l y i n com m u n it y lif e.
- Religious suppor t
An sw e r s r e v e a l a b a l a n ce b e t w e e n t h o se ag r eei n g an d d i sag r eei n g w i t h t h e st at em en t t h at h o sp i t al i zat i o n w as u sed as t h e o n l y r eso u r ce f o r m ent al t r eat m ent befor e t he FHP. I t should be ask ed w hat t hese ot her resources include, and w het her t hey could be r elat ed t o r eligiosit y.
Ev en in t h e 2 1st cen t u r y, inv olv em en t w it h m y st icism per sist s in t r eat m ent of m ent al pat ient s.
Th e l a r g e n u m b e r o f p sy ch i a t r i c p a t i e n t s seeking religious help in a FHP in a cit y locat ed in t he int er ior of São Paulo St at e show s t hat difficult ies t o co p e w i t h t h e su f f er i n g cau sed b y m en t al i l l n ess, d i f f i cu l t i e s i n v o l v i n g h e a l t h se r v i ce s, h o p e s f o r a m iracle solut ion and t he environm ent in w hich religious ser v ices ar e of f er ed ar e p ar t of t h is p ict u r e. I n an at t em pt t o r ebalance t hem selv es and t heir gr oup of or igin, subj ect s w alk bet w een differ ent dom ains and pow er s: m edicine and r eligion( 12).
This is a w ay of t r ansfer r ing r esponsibilit ies and finding suppor t in som et hing st r onger t han hum an n at u r e. I n t h is sen se, h ealt h an d r eligiou s ser v ices, t h r o u g h t h ei r sp eci f i c w ay s o f b eh a v i o r, o f f er t h e elem en t s each p er son n eed s t o r esp on d t o h is/ h er an x iet ies.
Healt h t eam s should also pay at t ent ion t o t his f r a g i l i t y, a s t h e se a r ch f o r a m i r a cu l o u s r e l i e f o f
su f f er in g an d t h e p r esen ce of m y st ical d elir ia can con f ou n d in st ead of h elp m en t al p at ien t s an d t h eir
r elat iv es.
- Fam ily ov er load and need for suppor t and guidance
Ev en w it hout specify ing any t y pe, all gr oups a g r e e d t h a t m e n t a l i l l n e s s p u t s a n o v e r l o a d o n r elat iv es.
Th r ee m ain t y p es of ov er load ar e im p osed on t h e fam ily w h en t h ey liv e w it h a r elat iv e w h o is
m en t al l y i l l f o r m o r e t h an f i v e y ear s: 1 ) f i n an ci al o v e r l o a d , 2 ) o v e r l o a d i n f a m i l y r o u t i n e s a n d 3 )
ov er load t ak in g t h e f or m of p h y sical or em ot ion al diseases( 1 ).
Helping r elat ives t o int er act and m anage daily
lif e w it h t h eir p at ien t allev iat es b u r d en s, f acilit at es
t he est ablishm ent of a cooper at ion pr ocess, decr eases st r e ss f a ct o r s t h a t a ct i v a t e cr i si s si t u a t i o n s a n d st im u lat es t h e cr eat ion of par t icipat ion possibilit ies,
im pr ov ing t he qualit y of life of all st ak eholder s( 13). Th is is a t im e t o h ear st or ies of su f f er in g ,
needs, desir es possibilit ies and know ledge about w hat p eop le ex p ect f r om p r of ession als an d t h e sy st em .
Now adays, car e is needed t o avoid psychiat r ist s fr om b e i n g s t a n d a r d i z e r s , r e g u l a t o r s , s e p a r a t o r s o f m adness ( a r ole t hey have played ver y w ell since t he
b i r t h o f p sy ch i a t r y ) . Th e “ d e co n st r u ct i o n ” o f t h e concept of m adness and t r eat m ent s is in cour se( 14).
The Fam ily Healt h Pr ogram – FHP ( 2001) has played an im por t ant r ole in t he cont ext of t he cur r ent
h e a l t h s y s t e m . I t i s d e f i n e d a s a s t r a t e g y t h a t pr iv ileges healt h pr om ot ion, pr ot ect ion and r ecov er y
for indiv iduals and fam ilies, deliv er ing com pr ehensiv e an d con t in u ou s car e t o n ew bor n s as w ell as elder ly
people and t o healt hy and ill persons alike. The focus of care is t he fam ily, w hich is considered in it s physical an d social en v ir on m en t .
One of t he bot t lenecks t o expand t he Pr ogr am is t he idea t hat prim ary car e is a synonym of sim plified
t echnology. How ever, t he pr ogr am can be am plified, est ab lish in g a g ood lev el of in t eg r at ion w it h ot h er
pr ogr am s, including m ent al healt h.
Mo r eo v er, t o co n so l i d a t e t h e FHP, v a r i o u s
d i f f i c u l t i e s h a v e t o b e o v e r c o m e , i n c l u d i n g t h e com posit ion an d m ain t en an ce of pr of ession al t eam s a n d t h e c h a n g e i n r e f e r e n c e f r a m e w o r k s .
FI NAL CONSI DERATI ONS
These result s reveal t hat t he m ain differ ence in opinions on m ent al healt h care in t he FHP is bet w een com m unit y healt h agent s and t he ot her gr oups, w hile n u r s e s a n d f a m i l y m e m b e r s o b t a i n v e r y s i m i l a r s c o r e s . Pa t i e n t s ’ a n s w e r s d e m o n s t r a t e m o r e v a r i a b i l i t y, w h i l e n u r s e s ’ a n s w e r s a r e m o r e h o m o g en eo u s.
Th e i n c r e a s e d e f f i c a c y i n m a k i n g ap p o i n t m en t s an d t h e al m o st u n an i m o u s o p i n i o n s about t he im por t ance of FHP deser ve special at t ent ion.
Th i s r e s e a r c h e v i d e n c e s i n c o h e r e n c e i n
opin ion s abou t pr of ession al gu idan ce on m edicat ion
t r eat m ent and how pat ient s w it h m ent al disor der s use
t his infor m at ion.
Th ese r esu l t s su g g est t h e n eed f o r b et t er
pr of ession al pr epar at ion , in v iew of t h e im por t an ce
o f t h e Fam i l y Heal t h Pr o g r am an d t h e p sy ch i at r i c
r efor m , em phasizing t he r ealit y of j oint w or k , w hich
cov er s t h e ch ar act er ist ic dy n am ics of t h e academ ic
realit y as w ell as t he associat ion bet w een relat ives of
m ent al pat ient s and fam ily healt h t eam s.
REFERENCES
1 . K o g a M , Fu r e g a t o A RF. Co n v i v ê n c i a c o m a p e s s o a esquizofr ênica: sobr ecar ga fam iliar. Ciência, Cuidado e Saúde/ UEM 2 0 0 2 ; 1 ( 1 ) : 7 5 - 9 .
2. Fur egat o ARF, Sant os OS, Nievas AF, Silva EC. O far do e as est r at égias da fam ília na conv iv ência com o por t ador de d o e n ç a m e n t a l . Te x t o & Co n t e x t o En f e r m a g e m 2 0 0 2 ; 1 1 ( 3 ) : 5 1 - 6 .
3 . Mor gado A, Lim a LA. Desin st it u cion alização: su as bases e a e x p e r i ê n c i a i n t e r n a c i o n a l . J B r a s Ps i q u i a t r. 1 9 9 4 ; 4 3 ( 1 ) : 1 9 - 2 8 .
4 . Min ist ér io da Saú de ( BR) . Fu n dação Nacion al da Saú de. Pr ogr am a de Saúde da Fam ília: saúde dent r o de casa. Br asília ( DF) : Minist ér io da Saúde; 1 9 9 4 .
5 . Rolim MA. Os cu id ad os d e en f er m ag em n o t r at am en t o f a r m a c o l ó g i c o d o s t r a n s t o r n o s m e n t a i s n o B r a s i l . I n : O r g a n i z a ç ã o M u n d i a l d a S a ú d e . O U s o Ra c i o n a l d e Medicam ent os Psiquiát r icos. Rio de Janeir o ( RJ) : OMS; 1997. p . 9 3 - 1 0 0 .
6 . Or g a n i za ci ó n Pa n a m e r i ca n a d e l a Sa l u d / Or g a n i za ci ó n Mundial de la Salud - OPAS/ OMS. Pr ogr am a de Salud Ment al, Div isión de Pr om oción de Salud. Modelo par a la capacit ación d e la en f er m er a g en er al en id en t if icación y m an ej o d e los t r ast or nos afect iv os. Gener alist a I ; Washingt on ( DC) : 1999. 7 . Pit t a AMF. Qualidade de v ida: um a ut opia opor t una. Rev Ciên Saú d e Colet iv a 2 0 0 0 ; 5 ( 1 ) : 2 4 - 7 .
8 . Min ist ér io da Saú de ( BR) . Legislação em Saú de Men t al: 1 9 9 0 - 2 0 0 4 . Po r t a r i a GM n º 1 0 6 . D i sp õ e so b r e se r v i ço s r esidenciais t er apêut icos. Br asília ( DF) : Minist ér io da Saúde; 2 0 0 4 .
9. Fur egat o ARF. A condut a hum ana e a t r aj et ór ia do ser e fazer da enfer m agem psiquiát r ica. I n: Jor ge MSB, Silva MV, O l i v e i r a FB , o r g a n i z a d o r a s . S a ú d e M e n t a l : d a p r á t i c a psiquiát r ica asilar ao t er ceir o m ilênio. São Paulo ( SP) : Lem os; 2 0 0 0 . p . 9 3 - 1 1 6 .
1 0 . St in gel A, Len gr u ber V. A in t er ação dos psicof ár m acos com out r as for m as de t r at am ent o dos t r anst or nos m ent ais no Br asil. I n: Or ganização Mundial da Saúde - O Uso Racional d e Med icam en t os Psiq u iát r icos. Rio d e Jan eir o ( RJ) : OMS; 1 9 9 7 . p . 7 1 - 8 6 .
1 1 . S c a t e n a M CM . Re a b i l i t a ç ã o p s i c o s s o c i a l : l a r e s abr igados. I n: Cont el JBO, or ganizador VI I I Ciclo de Est udos em Saú de Men t al. Mu lt idisciplin ar idade e r ef or m a - t em as, pr át icas e polít icas em saú de m en t al. Ribeir ão Pr et o ( SP) : São Fr an cisco; 2 0 0 0 .
12. Danese MCF, Fur egat o ARF. O usuár io de psicofár m acos n u m p r og r am a d e saú d e d a f am ília e su as r ep r esen t ações s o b r e o s s e r v i ç o s r e l i g i o s o s . S a ú d e e m D e b a t e 2 0 0 1 ; 2 5 ( 5 8 ) : 7 0 - 6 .
13. Melm an J. Fam ília e doença m ent al: r epensando a r elação en t r e p r of ission ais d e saú d e e f am iliar es. São Pau lo ( SP) : Escr i t u r a s; 2 0 0 1 .
14. Basaglia F, coor denador. A inst it uição negada: r elat o de um hospit al psiquiát r ico. Rio de Janeir o ( RJ) : Gr aal; 1985. 1 5 . S t a r f i e l d B . A t e n ç ã o p r i m á r i a : e q u i l íb r i o e n t r e necessidades de saúde, ser v iços e t ecnologia. Br asília ( DF) : UNESCO/ Min ist ér io d a Saú d e; 2 0 0 2 .