www.jped.com.br
ORIGINAL
ARTICLE
Characterization
of
a
group
unrelated
patients
with
arthrogryposis
multiplex
congenita
夽
Margarita
Valdés-Flores
a,1,
Leonora
Casas-Avila
a,1,
Edgar
Hernández-Zamora
a,∗,
Susana
Kofman
b,
Alberto
Hidalgo-Bravo
aaGeneticsDepartment,InstitutoNacionaldeRehabilitación(INR),MexicoCity,Mexico
bGeneticsDepartment,HospitalGeneraldeMéxico,FacultaddeMedicina,UniversidadNacionalAutónomadeMéxico(UNAM),
MexicoCity,Mexico
Received19January2015;accepted13April2015 Availableonline9October2015
KEYWORDS
Contracture; Arthrogryposis;
Amyoplasiacongenita
Abstract
Objective: Arthrogryposismultiplex congenitaisa relativelyrare neuromuscular syndrome,
withaprevalenceof1:3000---5000newborns.In thisstudy,theauthors describetheclinical featuresofagroupof50unrelatedMexicanpatientswitharthrogryposismultiplexcongenita.
Methods: Patientswerediagnosedby physicalandradiographicexaminationandthefamily
historywasevaluated.
Results: Ofthe50cases,ninepresentedotherfeatures(pectumexcavatum,cleftpalate,
men-tal retardation,ulnaragenesis, etc.).Environmentalfactors, aswellasprenatalandfamily history,wereanalyzed.Thechromosomalanomaliesandclinicalentitiesassociatedwith arthro-gryposismultiplexcongenitawerereported.Nochromosomalaberrationswerepresentinthe caseswith mentalretardation.Three unrelatedfamilialcases witharthrogryposismultiplex congenitawereobservedinwhichautosomalrecessive,autosomaldominantandX-linked inher-itancepatternsarepossible.Aliteraturereviewregardingarthrogryposismultiplexcongenita wasalsoconducted.
Conclusions: Itisimportanttoestablishpatient-specificphysicaltherapyandrehabilitation
pro-grams.Amultidisciplinaryapproachisnecessary,withmedical,surgical,rehabilitation,social andpsychologicalcare,includinggeneticcounseling.
©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:Valdés-FloresM,Casas-AvilaL,Hernández-ZamoraE,KofmanS,Hidalgo-BravoA.Characterizationofagroup
unrelatedpatientswitharthrogryposismultiplexcongenita.JPediatr(RioJ).2016;92:58---64.
∗Correspondingauthor.
E-mail:[email protected](E.Hernández-Zamora).
1Theseauthorscontributedtothepreparationofthismanuscriptinthesameway.
http://dx.doi.org/10.1016/j.jped.2015.04.008
PALAVRAS-CHAVE
Contratura; Artrogripose;
Amioplasiacongênita
Caracterizac¸ãodeumgrupodepacientesnãorelacionadoscomartrogriposemúltipla
congênita
Resumo
Objetivo: AArtrogriposemúltiplacongênitaéumasíndromeneuromuscularrelativamenterara,
comprevalênciade1:3000-5000recém-nascidos.Éporissoque,nesteestudo,descrevemosas característicasclínicasdeumgrupode50casosdepacientesmexicanosnãorelacionadoscom Artrogriposemúltiplacongênita.
Métodos: Ospacientes foram diagnosticados por exame físico e radiográfico, e o histórico
familiarfoiavaliado.
Resultados: Descrevemos50pacientesnãorelacionadoscomArtrogriposemúltiplacongênita.
Novedelesapresentaram outrascaracterísticas (pectusexcavatum,fissura palatina,retardo mental,agenesiadaulna,etc.).Foramanalisadososfatoresambientais,pré-nataiseohistórico familiar.Relatamosasanomaliascromossômicaseasentidadesclínicasassociadascoma Artro-griposemúltiplacongênita.Nãohavianenhumaaberrac¸ãocromossômicanoscasoscomretardo mental. Tambémencontramos 3 casos familiaresnão relacionadoscom Artrogripose múlti-pla congênita,emquesãopossíveispadrõesdeheranc¸aautossômicarecessiva,autossômica dominanteeligadaaocromossomoX.Tambémanalisamosapreocupac¸ãodaliteraturacoma Artrogriposemúltiplacongênita.
Conclusões: Reiteramosaideiadequeéimportanteestabelecerprogramasdefisioterapiae
reabilitac¸ãoespecíficosparaospacientes.Énecessáriaumaabordagemmultidisciplinarcom cuidado médico, cirúrgico, de reabilitac¸ão, social e psicológico, incluindo aconselhamento genético.
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
The term arthrogryposis is derived from the Greekwords
‘‘arthron’’and‘‘gryposis’’,which mean‘‘curvedjoints’’. Multiplesynonymshavebeenusedtodescribethisclinical feature: multiple congenital articular rigidity, amyoplasia
congenital, myodystrophia fetalis deformans, congenital
arthromyodysplasia, multiple congenital contractures and
arthrogryposismultiplexcongenita(AMC).1,2AMCreferstoa
largeheterogeneousgroupofconditions,characterizedby contractedmusclesandnon-progressivecongenital limita-tionofmovementoftwoormoredifferentjointswiththick periarticularcapsules.AMCis relativelyrare, occurringin approximately1:3000---5000 newborns; males andfemales are equallyaffected. All fourextremities are involved in 50---60%ofcases;lowerlimbs,in30---40%,andupperlimbs,in 10---15%.In20%ofcases,thereisdislocationandsubluxation of hips,patellasandknees, while vertebraland temporo-mandibularjointsarerarelyinvolved.3,4Themostcommon
typeof AMC is amyoplasia,which represents one-thirdof allcases.Amyoplasiaischaracterizedbysymmetrical posi-tioning of the limbs with severe talipes equinovarus and extended elbows. A feature that often occur Sis a char-acteristicmidlinefacialhemangioma.Somepatientscould also have abdominal structure or genital abnormalities, downslopingandinternallyrotatedshoulders,andpronated forearmswithflexiondeformities ofwrists andfingers. In addition to talipes equinovarus, lower limb involvement most often includes flexed or extended knees; hips may presentasflexedandexternallyrotated,extendedand sub-luxated,ordislocated.3,5,6
AMC can be present in over 150 specific conditions, whichinclude a largegroup of myopathicand neurogenic disorders,connectivetissueanomalies,andfactorsthat pro-ducelimitationoffetalmotion(structuralabnormalitiesof the uterus, amniotic bands syndrome, twining, and oligo orpolyhydramnios).7,8Inanimalmodels,contractureshave
been induced by viruses, neuromuscular blocking, insec-ticides, anticonvulsants, neuromuscular blocking agents, ethanol,limbimmobilization,andhyperthermia.8---14 These
factors appear to interfere with the development of the limbs,resulting inloss of muscle mass withimbalance of musclepower at thejoints. The etiology of AMCincludes bothgeneticandenvironmentalfactors;amongthegenetic causes, single gene defects and chromosomal disorders have been reported.Molecular analysishas revealed that adeterminedphenotypecanbecausedbymutationsin dif-ferentgenes,evidencingthegeneticheterogeneityofthis disease.3
The present study aimed to describe the clinical fea-turesof50caseswithAMC,includingabriefreviewofthe literatureregardingthistopic.
Patient
and
methods
Aprospectiveandcross-sectionalstudywasconductedwith 50patientswithAMC.Thesepatientswerereferredtothe GeneticsDepartment of theNational Institute of
Rehabil-itation (Mexico City, Mexico) with presumptive diagnosis
of AMC, during a period of three years. All were
aboutthecharacteristicsofthestudyandagreedto partic-ipate.
The study’s protocol was approved by the Institute’s
researchandethicscommittees.ThediagnosisofAMCwas
basedontypicalclinical features,suchasnon-progressive jointcontractureslimitingextensionorflexionmovements evidentatbirth,involvingmorethanonejoint,eitherfrom theupperorlowerlimbsorboth.Inallcases,thepatients
weresubjected tophysical andradiographic examination.
Themedicalfamilyhistoryanddeliverydatawereassessed duringmedicalconsultationinthedepartmentofGenetics. Pregnancyhistoryevaluationincludedpositionofthefetus inutero, infections,fever, useofillegalsubstances,
med-ications,and unusual events during pregnancy. Karyotype
analysis wasperformed from peripheral blood leukocytes
using G banding stain according to standard techniques.
Briefly,peripheralbloodcollectedbyvenouspuncture,using aheparinizedsyringe,wascultivatedinthepresenceof
phy-tohaemagglutinin.After 72h, cellgrowth wasstopped by
addingcolcemid.Cellcultureswereharvestedandtreated withhypotonicandfixativesolution.Sampleswereplaced onglassslidesforstaining15;25metaphaseswereanalyzed
underalightmicroscopeforeachcase.
Results
Inthepresentstudy,28(56%)patientswerefemalesand22
(44%)males; both sexes were affected. 27(54%) patients
wereaffectedinallfourlimbs;lowerandupperlimbswere affectedin18(36%)andfive(10%)casesrespectively. The distributionoflimbinvolvementisshowninFig.1A.Articular compromisecanpresentagreatvariability,evenwithinthe samepatient:onejointcanbecompletelyextendedwhile thecontralateraljointis inflexion.Fig.1Bdepictsa clin-icalinvolvement ofupper limbs: forearmpronosupination was compromised bilaterally, wrists and interphalangeal joints were fixed in a semi-flexed position and no flex-ioncreaseswere present. Fig.1Cexemplifies lowerlimbs involvement,wheretherightandleftkneeswerefixedinthe semi-flexedandextendedposition,respectively; theright ankle wasextended andthe left ankle wasin adduction,
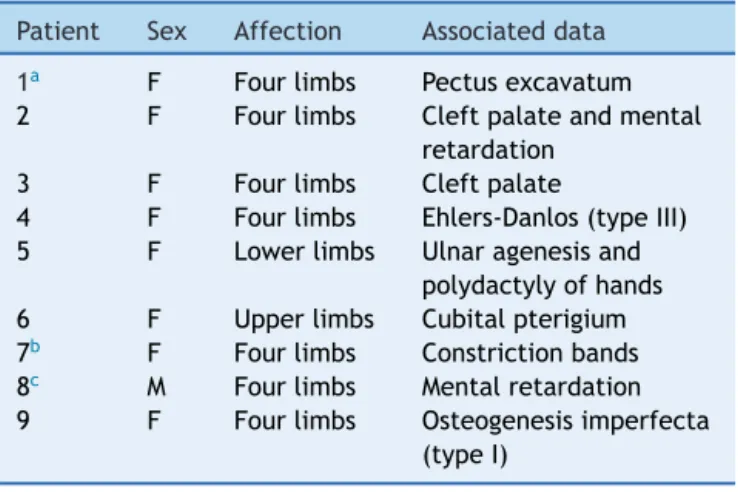
Table1 Congenitalanomaliesassociatedwith arthrogry-posismultiplecongenita.
Patient Sex Affection Associateddata
1a F Fourlimbs Pectusexcavatum
2 F Fourlimbs Cleftpalateandmental retardation
3 F Fourlimbs Cleftpalate
4 F Fourlimbs Ehlers-Danlos(typeIII) 5 F Lowerlimbs Ulnaragenesisand
polydactylyofhands 6 F Upperlimbs Cubitalpterigium 7b F Fourlimbs Constrictionbands
8c M Fourlimbs Mentalretardation
9 F Fourlimbs Osteogenesisimperfecta (typeI)
F,female;M,male.
a Consanguinitydocumented.
b Motherwithdiabetesmellitus.
c Polydactylyofhandswaspresentinthemotherand
chromo-somalstudyinthispatientwasnormal.
and the patient was unable to move them. The medium
ageat presentationtotheclinicwas4.6years(agerange from0to7 years).When investigatingthe involvementof other joints,hipdislocation andsubluxationwasobserved in 14cases(28%), andjointhypermobility with hyperflex-ionwerepresentintwocases.Agreatvarietyofcongenital abnormalities(orthopedicor non-orthopedic)arereported tobeassociatedwithAMC.Inthiscohort,otherclinical fea-turessporadicpresentationwasalsoobservedinnineoutof 50cases(Table1).Inthepresentseries,maternal disease waspresent intencases:onecasewithdiabetesmellitus, fivecasespresentedurinarytractinfectionandfever(above 39◦C)inthe firstandsecond trimesterof pregnancy,four
casesofeclampsia,andsixhadvaginalbleedingduringthe first trimester. Delivery history indicated that fetal posi-tionat deliverywascephalic in25 cases,breechedin 16, andtransverseinsevencases;2caseshadotherpositions. Onemultiplebirth(dizygotictwins)andacasewithuterus abnormalitieswerealsoobserved.
B
C
54% Affectation
in all four limbs
36% Affectation
in legs
10% Affectation
in arms
A
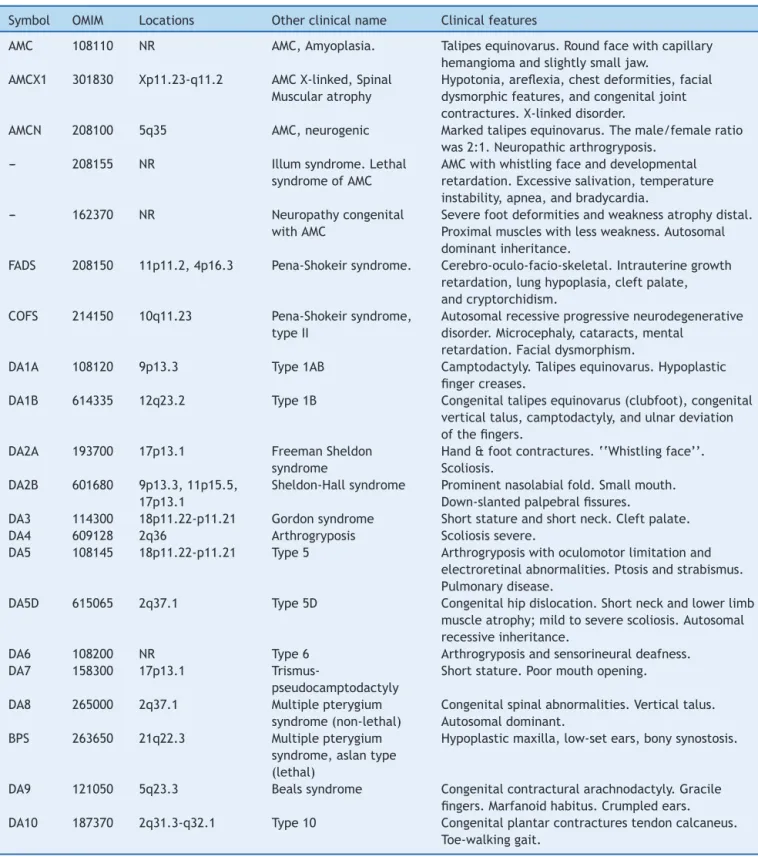
Table2 Somedifferentvariantsdescribedintheclassificationofmultiplexcongenitalanddistalarthrogryposis.
Symbol OMIM Locations Otherclinicalname Clinicalfeatures
AMC 108110 NR AMC,Amyoplasia. Talipesequinovarus.Roundfacewithcapillary hemangiomaandslightlysmalljaw.
AMCX1 301830 Xp11.23-q11.2 AMCX-linked,Spinal Muscularatrophy
Hypotonia,areflexia,chestdeformities,facial dysmorphicfeatures,andcongenitaljoint contractures.X-linkeddisorder.
AMCN 208100 5q35 AMC,neurogenic Markedtalipesequinovarus.Themale/femaleratio was2:1.Neuropathicarthrogryposis.
--- 208155 NR Illumsyndrome.Lethal syndromeofAMC
AMCwithwhistlingfaceanddevelopmental retardation.Excessivesalivation,temperature instability,apnea,andbradycardia.
--- 162370 NR Neuropathycongenital withAMC
Severefootdeformitiesandweaknessatrophydistal. Proximalmuscleswithlessweakness.Autosomal dominantinheritance.
FADS 208150 11p11.2,4p16.3 Pena-Shokeirsyndrome. Cerebro-oculo-facio-skeletal.Intrauterinegrowth retardation,lunghypoplasia,cleftpalate, andcryptorchidism.
COFS 214150 10q11.23 Pena-Shokeirsyndrome, typeII
Autosomalrecessiveprogressiveneurodegenerative disorder.Microcephaly,cataracts,mental
retardation.Facialdysmorphism.
DA1A 108120 9p13.3 Type1AB Camptodactyly.Talipesequinovarus.Hypoplastic fingercreases.
DA1B 614335 12q23.2 Type1B Congenitaltalipesequinovarus(clubfoot),congenital verticaltalus,camptodactyly,andulnardeviation ofthefingers.
DA2A 193700 17p13.1 FreemanSheldon syndrome
Hand&footcontractures.‘‘Whistlingface’’. Scoliosis.
DA2B 601680 9p13.3,11p15.5, 17p13.1
Sheldon-Hallsyndrome Prominentnasolabialfold.Smallmouth. Down-slantedpalpebralfissures.
DA3 114300 18p11.22-p11.21 Gordonsyndrome Shortstatureandshortneck.Cleftpalate. DA4 609128 2q36 Arthrogryposis Scoliosissevere.
DA5 108145 18p11.22-p11.21 Type5 Arthrogryposiswithoculomotorlimitationand electroretinalabnormalities.Ptosisandstrabismus. Pulmonarydisease.
DA5D 615065 2q37.1 Type5D Congenitalhipdislocation.Shortneckandlowerlimb muscleatrophy;mildtoseverescoliosis.Autosomal recessiveinheritance.
DA6 108200 NR Type6 Arthrogryposisandsensorineuraldeafness. DA7 158300 17p13.1
Trismus-pseudocamptodactyly
Shortstature.Poormouthopening.
DA8 265000 2q37.1 Multiplepterygium syndrome(non-lethal)
Congenitalspinalabnormalities.Verticaltalus. Autosomaldominant.
BPS 263650 21q22.3 Multiplepterygium syndrome,aslantype (lethal)
Hypoplasticmaxilla,low-setears,bonysynostosis.
DA9 121050 5q23.3 Bealssyndrome Congenitalcontracturalarachnodactyly.Gracile fingers.Marfanoidhabitus.Crumpledears. DA10 187370 2q31.3-q32.1 Type10 Congenitalplantarcontracturestendoncalcaneus.
Toe-walkinggait.
AMC,arthrogryposismultiplexcongenital;DA,distalarthrogryposis;FADS,fetalakinesiadeformationsequence;COFS,
cerebrooculo-facio-skeletalsyndrome;BPS,Bartsocas-Papassyndrome;OMIM,OnlineMendelianInheritanceinMan;NR,notreported.
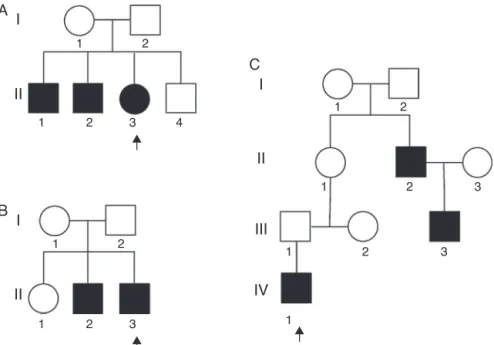
Table 2presents abrief review ofthe literatureabout differentvariantsof AMCanddistalarthrogryposis. In the presentseries,thereweretwounrelatednon-familialcases whereconsanguinitywasobserved.Inaddition,three famil-ial cases with no evidence of consanguinity were also observed(Fig.2).
Discussion
I
A
B
C
II
1 2
1 2
1 2
1 2
1 2
1
1
2
3
3 4
3
1 2 3
I
II
I
II
III
IV
Figure2 Pedigreesofthethreefamilialcases(A---C)withthesametypeofArthrogryposismultiplexcongenital.Arrowsindicate theaffectedpatients.Squaresrepresentmalesandcircles,females;filledsquares/circlesrepresentaffectedindividuals.
the fetal growth, which is associated with the
develop-ment of extraconnective tissue aroundthe joints. These
deformities are usually symmetric, non-progressive, and
involvemorethanonebodyarea.3AMCisveryevident at
birth, and diagnosis is possible prenatally with real-time ultrasound.16,17
In AMC, all four extremitiesare involved in 50---60% of cases;lowerlimbs,in30---40%,andupperlimbs,in10---15%.7
Inthis series,54% of the patients showedinvolvement of all extremities, 36% of the lower limbs, while the upper limbswereinvolvedin10%;nodifferencesbetweenmales andfemales were observed.These data agreewith those reportedintheinternationalliterature(Fig.1).3,7,13,14,18
Atleast150specificclinicalentitieshavebeendescribed withAMC.Itisapparentthatmultipleetiologicfactors con-vergeupononecommonresponse,whichresultsinlossof movement ofthe joints. AMCis alsoknowntooccur asa componentof a large group ofheterogeneous myopathic, neurogenic,andvasculardisorders,aswellasother anoma-liessuchasskeletaldysplasia.3,7Table2depictsanupdated
summary of different variants described in the classifica-tionofAMCanddistalarthrogryposis.Abnormalconnective tissue,specificallycollagen,mayinterferewiththenormal developmentofbone,cartilage,andtendons;thiscanresult injointcontracturesandfibrosis.Inthisseries,onepatient hadEhlers---Danlostype3andonehadosteogenesis imper-fectatypeI(patients4and9,Table1).
Prenatalhistory isvery importantinthe studyof AMC. In this cohort, maternal diseases such as diabetes melli-tus,urinarytractinfectionwithfever andeclampsiawere observed. There was also one event of vaginal bleeding duringthe first trimester of pregnancy. The identification oftheseenvironmentalandsporadicnon-geneticfactorsis importanttoestablish specifictypesof AMC.It ispossible thatenvironmentalfactorshavecontributedintheetiology ofAMCinthesecases.
Ithasbeendescribedthatabnormalfetalpositions, mul-tiplegestation,andstructural abnormalitiesof theuterus can produce limitation of the joint movements and con-sequently promote AMC. Halfof the present patients had cephalic presentation while the other half showedone of theconsideredriskpresentations(breeched,transverse,or otherposition).Onemultiplebirthandonecasewithuterus abnormalities, which are also considered as risk factors, werealsoobserved.
SpecificinheritancemodesofAMCaredescribedfor par-ticular forms of contractures. Sometimes AMC is caused by a defect in a single gene; in these cases, autosomal dominant,autosomalrecessiveandX-linked inheritanceis possible. At the moment, several loci related with dif-ferent types of AMC have been reported, for example: contractural arachnodactyly(5q23-31), diastrophic dyspla-sia (5q31), lethal spinal muscular atrophy (5q13.3), distal arthrogryposis typeI(9q21.2), symphalangism(9q), lethal X-linkedarthrogryposis (Xp11.3-q11.2),and ophthalmople-gia (12p11.2-q12) (Table2).10---13,19---24 There arealso some
reportswhereapatientwhitAMCcarriesaduplicationina chromosomeandadeletioninanotherchromosome.23
inheritance.The factthat patientII-1 is notaffected can beexplainedduetoincompletepenetrance.
AMCmayalsobecausedbynumericalorstructural chro-mosomalaberrations.Theseabnormalitiesareparticularly frequent in casesof AMCassociatedwithmental retarda-tion.Mostofthesechromosomeabnormalities arepresent as de novo events, which means that the risk of recur-renceforrelativesisverylow.25,26Inthisstudy,chromosomal
abnormalitieswerepresentintwooutof50cases,onewith 47,XY,+21andanotheronewith47,XXY.Nevertheless,these chromosomalanomalies arenot associatedwithAMC. The twopatientswithmentalretardationinthisseries(2and8) didnotpresentchromosomalanomalies,asshowedby kar-yotypeanalysisperformed inperipheral blood leukocytes. However,thepossibilityof achromosomal mosaicismin a smallproportion cannotbe discarded,as noother tissue, suchasskin(fibroblast),wasusedforkaryotypeanalysis.25
ChromosomalstudiesinpatientswithAMCandmental retar-dationormultisystemicdisordersareveryimportantforthe recognitionofclinical syndromeswithchromosomal impli-cation.
The postnatal diagnosis of AMC requires a compila-tionof medical records,familyhistory (i.e., other family membersaffected,hyperextensibility,hypotonia,andother signs related to the disease), laboratory data (serum enzymes),radiographicanalysis,electrophysiological stud-ies, and pathologic studies (including muscle and nerve biopsy). For cases considered to be sporadic, where no relevantmedicalhistoryisfound andnomendelian inher-itance pattern can be observed, the empiric risk of recurrenceis around3---5%. The appropriatetreatment in AMCshould bemultidisciplinary,withthe participationof a pediatrician with specialty in orthopedics, a physical therapist, a geneticist, and a neurologist, among others. The primary objective of the treatment is to improve the function of the affected limbs. The management of potentially preventable complications (joint dislocation, osteoarthritis, andscoliosis)is fundamental toensure the quality of life of the patients. Conversely, rehabilita-tionprogramsfacilitateandpromoteindependentfunction in everyday activities. And finally, as has been exposed above, this condition involves genetic and environmen-tal factors;therefore, geneticcounselingshould betaken into consideration if the family plans to have another child.27,28
In this article, the classification of AMC was updated according to the literature. Only a few reports on AMC in Mexican population were retrieved. In 1976, a report described 83 cases29; 46 cases were reported in 1991,30
and amanuscript related todistal arthrogryposis type IIB waspublishedin 1999.22 Inthis study,50newcases were
included, withvariabledegree ofseverity. Some of these caseswereassociatedwithothermedicalproblems,which resultedinseverelimitationsinthesepatients.Therefore, it is important to establish patient-specific physical ther-apyandrehabilitationprograms,accordingtotheparticular characteristics and evolutionof each case. As in previous studies,theauthorsreiteratethatitisnecessarya multidis-ciplinary approach, withmedical, surgical, rehabilitation, social, and psychological care, including genetic counsel-ing,inordertoachieveasuccessfulmanagementofthese patients.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Hall JG. Arthrogryposis (multiple congenital contractures): diagnostic approach to etiology, classification, genetics, and generalprinciples.EurJMedGenet.2014;57:464---72.
2.StilliS,AntonioliD,LampasiM,DonzelliO.Managementofhip contracturesanddislocationsinarthrogryposis.Musculoskelet Surg.2012;96:17---21.
3.Bevan WP, Hall JG, Bamshad M, Staheli LT, Jaffe KM, Song K. Arthrogryposis multiplexcongenita (amyoplasia):an orthopaedicperspective.JPediatrOrthop.2007;27:594---600.
4.HodgsonP,WeinbergS,ConskyC.Arthrogryposismultiplex con-genitaofthetemporomandibularjoint.OralSurgOralMedOral Pathol.1988;65:289---91.
5.HallJG,ReedSD,DriscollEP,PartI.Amyoplasia:acommon, spo-radicconditionwithcongenitalcontractures.AmJMedGenet. 1983;15:571---90.
6.SarwarkJF,MacEwenGD,ScottCIJr.Amyoplasia(acommon formofarthrogryposis).JBoneJointSurgAm.1990;72:465---9.
7.Swinyard CA, Bleck EE. The etiology of arthrogryposis (multiple congenital contracture). Clin Orthop Relat Res. 1985;194:15---29.
8.BørlumKG.Amnioticbandsyndromeinsecondtrimester asso-ciatedwithfetalmalformations.PrenatDiagn.1984;4:311---4.
9.DelTortoU,BianchiO,PoneG,SantéG.Experimentalstudyon theetiologyofcongenitalmultiplearthrogryposis.ItalJOrthop Traumatol.1983;9:91---9.
10.Hall JG, Reed SD. Teratogens associated with congeni-tal contractures in humans and in animals. Teratology. 1982;25:173---91.
11.HallJG,ReedSD,GreeneG.Thedistalarthrogryposes: delin-eationofnewentities---reviewandnosologicdiscussion.AmJ MedGenet.1982;11:185---239.
12.HallJG,ReedSD,ScottCI,RogersJG,JonesKL,CamaranoA. ThreedistincttypesofX-linkedarthrogryposisseenin6 fami-lies.ClinGenet.1982;21:81---97.
13.HallJG.Inuteromovementanduseoflimbsarenecessaryfor normalgrowth:astudyofindividualswitharthrogryposis.Prog ClinBiolRes.1985;200:155---62.
14.HallJG.Geneticaspectsofarthrogryposis.ClinOrthopRelat Res.1985;194:44---53.
15.Babu A, Verma RS. Anatomy of human genome by restric-tion endonucleases Alul, Ddel, Haelll, Hinfl, Mobol and Rsal,and theirapplicationinclinicalcytogenetics.Cytobios. 1990;62:7---19.
16.BendonR,DignanP,SiddiqiT.Prenataldiagnosisof arthrogry-posismultiplexcongenita.JPediatr.1987;111:942---7.
17.BuiTH,LindholmH,DemirN,ThomassenP.Prenataldiagnosis ofdistalarthrogryposistypeIbyultrasonography.PrenatDiagn. 1992;12:1047---53.
18.Robin NH,Franklin J,PruckaS, RyanAB, Grant JH.Clefting amnioticbands,andpolydactyly:adistinctphenotypethat sup-portsanintrinsicmechanismforamnioticbandsequence.AmJ MedGenetA.2005;137A:298---301.
19.LaiMM, TettenbornMA,Hall JG, SmithLJ, Berry AC.Anew form of autosomal dominant arthrogryposis. J Med Genet. 1991;28:701---3.
20.McCormackMK, Coppola-McCormack PJ,Lee ML. Autosomal-dominantinheritanceofdistalarthrogryposis.AmJMedGenet. 1980;6:163---9.
22.Rivera MR, Avila CA, Kofman-Alfaro S. Distal arthrogryposis typeIIB:probableautosomalrecessiveinheritance.ClinGenet. 1999;56:95---7.
23.Emy DorfmanL, LeiteJC, Giugliani R, RiegelM. Microarray-basedcomparativegenomichybridizationanalysisinneonates withcongenitalanomalies: detection ofchromosomal imbal-ances.JPediatr(RioJ).2015;91:59---67.
24.GeniniS,MalekM,SpilarS,NguyenTT,MénétreyF,GebertS, etal.Arthrogryposismultiplexcongenita (AMC),ahereditary diseaseinswine,mapstochromosome5 bylinkageanalysis. MammGenome.2004;15:935---41.
25.ReedSD,HallJG,RiccardiVM,AylsworthA,TimmonsC. Chro-mosomalabnormalitiesassociatedwithcongenitalcontractures (arthrogryposis).ClinGenet.1985;27:353---72.
26.Serville F, Dufau-Casanabe J, Fontan D. Arthrogryposis and 46,XY,t(1;16) chromosome constitution. Clin Genet. 1986;29:453---5.
27.Hahn G. Arthrogryposis. Pediatric review and habilitative aspects.ClinOrthopRelatRes.1985;194:104---14.
28.WilliamsPF.Managementofupperlimbproblemsin arthrogry-posis.ClinOrthopRelatRes.1985;194:60---7.
29.GilbertoSorianoJ,Ruiz-FigueroaF.Multiplecongenital arthro-gryposisasacauseoflearningandcommunicatingproblems. BolMedHospInfantMex.1976;33:179---88.