www.jped.com.br
ORIGINAL
ARTICLE
Costs
of
hospitalization
in
preterm
infants:
impact
of
antenatal
steroid
therapy
夽
,
夽夽
Joice
Fabiola
Meneguel
Ogata
a,∗,
Marcelo
Cunio
Machado
Fonseca
b,
Milton
Harumi
Miyoshi
a,
Maria
Fernanda
Branco
de
Almeida
a,
Ruth
Guinsburg
aaDisciplineofNeonatalPediatrics,EscolaPaulistadeMedicina(EPM),UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,
SP,Brazil
bDisciplineofGynecology,EscolaPaulistadeMedicina(EPM),UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
Received28January2015;accepted13March2015 Availableonline29June2015
KEYWORDS Preterminfant; Costsandcost analysis; Hospitalization; Glucocorticoids
Abstract
Objective: Toestimate thecosts ofhospitalizationin prematureinfants exposed or notto
antenatalcorticosteroids(ACS).
Method: Retrospective cohort analysis of premature infants with gestational age of
26---32weekswithoutcongenitalmalformations,bornbetweenJanuaryof2006andDecemberof 2009inatertiary,publicuniversityhospital.Maternalandneonataldemographicdata, neona-talmorbidities,andhospitalinpatientservicesduringthehospitalizationwerecollected.The costswereanalyzedusingthemicrocostingtechnique.
Results: Of 220 patients that met the inclusion criteria, 211 (96%) charts were reviewed:
170newbornsreceivedatleastonedose ofantenatalcorticosteroidand41didnotreceive theantenatalmedication.Therewasa14---37%reductionofthedifferentcostcomponentsin infantsexposed toACSwhentheentire populationwasanalyzed,withoutstatistical signifi-cance.Regardingprematureinfantswhoweredischargedalive,therewasa24---47%reduction ofthecomponentsofthehospitalservicescostsfortheACSgroup,withasignificantdecrease inthelengthofstayintheneonatalintensivecareunit(NICU).Invery-lowbirthweightinfants, consideringonlythesurvivors,ACSpromoteda30---50%reductionofallelementsofthecosts, witha36%decreaseinthetotalcost(p=0.008).Thesurvivorswithgestationalage<30weeks showedadecreaseinthetotalcostof38%(p=0.008)anda49%reductionofNICUlengthof stay(p=0.011).
夽 Pleasecitethisarticleas:OgataJF,FonsecaMC,MiyoshiMH,AlmeidaMF,GuinsburgR.Costsofhospitalizationinpreterminfants:impact
ofantenatalsteroidtherapy.JPediatr(RioJ).2016;92:24---31.
夽夽
DisciplineofNeonatalPediatrics,EscolaPaulistadeMedicina(EPM),UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](J.F.M.Ogata). http://dx.doi.org/10.1016/j.jped.2015.03.004
Conclusion: ACSreducesthecostsofhospitalizationofprematureinfantswhoaredischarged alive,especiallythosewithverylowbirthweightand<30weeksofgestationalage.
©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE Prematuro;
Custoseanálise decustos; Hospitalizac¸ão; Glucocorticoides
Custosdahospitalizac¸ãoderecém-nascidospré-termo:impactodacorticoterapia antenatal
Resumo
Objetivo: Estimaroscustosdainternac¸ãohospitalardeprematuros,cujasmãesreceberamou
nãocorticoideantenatal(CEA).
Método: Coorteretrospectivadeprematurossemmalformac¸õescongênitascomidade
gesta-cionalde26a32semanas,nascidosentrejaneiro/2006edezembro/2009,emhospitalpúblico, terciárioeuniversitário brasileiro.Coletaram-sedadosdemográficosmaternosedos recém-nascidos(RN),amorbidadeneonataleutilizac¸ãoderecursosdesaúdeduranteainternac¸ão hospitalar.Oscustosforamanalisadospelatécnicademicrocosting.
Resultados: Dos220nascidos queobedeciam acritérios de inclusão,211 (96%)prontuários
foramrevisados:170receberamCEAe41nãoreceberamamedicac¸ão.Analisando-setodaa populac¸ão,houvereduc¸ãode14-37%entreosdiferentescomponentesdocustonospacientes expostosaoCEA,semsignificânciaestatística.Naanálisedeprematurosquereceberamalta hospitalarvivos,ogrupocomCEAtevereduc¸ãode24-47%nosvários componentesdos cus-toshospitalares,comdiminuic¸ãosignificantedosdiasdeinternac¸ãoemterapiaintensiva.Os nascidoscompeso<1500g,considerando-sesomenteossobreviventes,sãoaquelesquemais sebeneficiaramdaadministrac¸ãodoCEA,comreduc¸ãosignificantedetodoscomponentesdos custos em30-50%,sendotal diminuic¸ãode36%nocusto total(p=0,008).Paraogrupocom idadegestacional<30semanas,tambémsobreviventes,houvediminuic¸ãodocustototalde38% (p=0,008)ereduc¸ãode49%dosdiasdeinternac¸ãoemUTIneonatal(p=0,011).
Conclusões: OCEAreduzocustohospitalardeprematurosquesobrevivemàinternac¸ãoapós
oparto,principalmentenaquelesabaixode1500ge30semanasdeidadegestacional. ©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
There hasbeen greatprogress in reducingchild mortality in the last twodecades.1,2 Since 1990, the global
neona-talmortalityratewasreducedby37%,from33to21deaths per1000livebirths,3andnowtheWorldHealthOrganization
(WHO),withtheEveryNewbornprogram,proposesa reduc-tionto10deathsper1000livebirthsuntiltheyear2035.For thisgoaltobeachieved,itwillbenecessarytoincreasethe useofeffectiveinterventionstoreducetheleadingcauses ofneonataldeaths,particularlyprematurity.4
Antenatal corticosteroids (ACS) participatein this con-textasoneoftheproveneffectiveinterventionstoreduce complicationsofprematurity,astheyinducefetalmaturity.5
In2010,asystematicreview6of 18randomizedcontrolled
trials involving the use of ACS was conductedin 14 high-incomecountriesthatparticipatedinthemeta-analysisof the Cochrane Library5 and in four middle-income
coun-tries, including Brazil. While the Cochrane meta-analysis suggestedthatACSreducedneonatalmortalityby31%,the newreviewshowedthatACSdecreasedneonatalmortality by 53% (RR 0.47; 95% CI: 0.35---0.64) and neonatal mor-bidityby37% (RR:0.63; 95%CI:0.49---0.81).It isbelieved that,inlow-incomecountrieswithfewneonatalintensive careresources, thebeneficialeffectsof corticosteroidsin
reducingneonatal morbidity and mortality could be even greater.6
DataontheuseofACSinBrazildemonstratethatmuch remainstobedonetoincreaseitsprescriptiontoBrazilian pregnantwomen.TheBrazilianNeonatalResearchNetwork annualreportin2012,involving20Brazilianuniversity hos-pitals, showed low use of ACS: 67% of pregnant women whogavebirthtopreterminfantsweighinglessthan1500g receivedtheantenatalmedication(rangingfrom62%to75% amongthecenters).7
Among preterm infants with birth weight <1000g, a recentstudyintheBrazilianpopulationdemonstratedthat two thirds of them received ACS.8 It is noteworthy that
the WHO considers ACS asa priorityintervention for the preventionofprematuritycomplications.9,10Itis
unaccept-ablethatcountrieswithhighratesofprematurity,suchas Brazil,donotuniversallyuseACSforriskpregnancies,which demonstratesmissedopportunities toincrease thechance ofsurvivalofpreterminfants.
IfACSusewasprevalentinBrazil,therecouldbea reduc-tioninmorbidityandmortalityassociatedwithprematurity and,consequently,inhospitalcosts.In1991,Mugfordetal.11
a14% decrease in the mean costper survivor.In another studyinvolvingACSandcosts,publishedin1995,Simpson& Lynch12 usedananalyticaldecision-makingmodeland
esti-matedareductionofthreeto17deathsandcostsavingsof 200,000to500,000dollarsper100babiesexposedtoACS.
In Brazil, there have been few studies involving costs relatedtopreterm infantswhose mothersreceivedornot ACS. Therefore, the present study aimed to analyze the hospitalcostsofhospitalizationofpreterminfantsbornin aBrazilianpublicuniversity hospitalexposed toantenatal corticosteroids,comparedtothosewhowerenot.
Methods
This was a retrospective analysis of a cohort of preterm infants born between January of 2006 and December of 2009, afterit was approved by the ResearchEthics Com-mitteeoftheinstitution.Preterminfantsbornbetween26 and32weeksGA,asdeterminedbythebestobstetric esti-mate,wereincludedintheanalysis.Infantswithcongenital malformationswereexcluded.13
DatawerecollectedfromtheneonatalunitofHospital Universitárioda EscolaPaulista deMedicina---Universidade FederaldeSãoPaulo,atertiarypublichospitalwhose neona-talunitis classifiedasLevelIIIbytheNational Registerof HealthcareFacilities(CadastroNacionalde Estabelecimen-tosdeSaúde[CNES]).14 At thetimeofthestudy,theunit
hadeightintensivecarebeds,eightconventionalneonatal intermediatecare beds,and four intermediate kangaroo-care beds. The maternity ward treated approximately 1000newbornsayear,andisspecializedinpregnantwomen with severe medical or obstetric complications and/or fetuseswithclinicaldiseasesormalformations.Ofthetotal numberof births, 30---40% were admittedto the neonatal unitannually.
Maternal demographic data, pregnancy complications, informationaboutdelivery,andneonataldemographicdata were collected from medical records of newborns. Data onACSadministrationwasassessed,considering infantsas belonging to the group exposed to corticosteroids if the motherhad received any dose of the medication for the purposeof fetalmaturation. Data werealso collected on neonatalmorbidityanddaysofhospitalization,dividedinto neonatalintensivecareunits(NICUs)andintermediatecare units.
Thecostanalysiswasconductedusingthemicrocosting process,15whichidentifiesandmeasureseachresourceused
byassigningthemvaluesandintegrating thisinformation. Thus, the costs were divided into respiratory, laboratory, medication, tests, hospital daily rates, and total costs, definedasfollows:
• Respiratory cost: evaluation of mechanical ventilation time, continuous positive airway pressure (CPAP), and inhaled oxygentherapy,in additiontotheneed forand numberofsurfactantdosesadministered.Theestimated respiratorycostwasbasedonthemaintenancecostsof mechanical ventilators, the CPAP circuit,gas consump-tion(oxygen)bythe mechanicalventilation equipment, andcubicmeter of oxygen.Therefore,adaily mechan-ical ventilation rate was calculated,as well as that of
CPAPandoxygeninhalation,inadditiontothecostofthe surfactantdose,usingthedrugpricelistbytheNational HealthSurveillanceAgency(AgênciaNacionalde Vigilân-ciaSanitária[ANVISA]).16
• Laboratory cost: all laboratory tests performed during hospitalization and costs were provided by the central laboratoryofthehospital.Costsoftestsperformedatthe unit,suchasglycemiaandcapillaryhematocrit,werealso estimated,takingintoaccountonlythecostofmaterials providedbythehospital’spurchasingdepartment. • Imaging test costs and others: all imaging tests
(X-rays, ultrasound, computed tomography [CT], mag-netic resonance imaging [MRI], and contrast studies), echocardiogram and electrocardiogram (ECG), fundus examination,otoacousticemissions,andneonatal screen-ingforinbornerrorsofmetabolismwereconsidered.The costswereestimatedbasedonthepaymentsystemofthe BrazilianUnifiedHealthSystem(SistemaÚnicodeSaúde [SUS]).
• Nutritionalcost:comprisedthedailyneonatalparenteral nutritioncost,whosevaluewasprovidedbythehospital pharmacy,aswellasthecostof enteralfeeding, calcu-latedwiththehelpoftheUnit’snutritionist,throughthe meanconsumption ofpretermandterminfantsformula andthemarketpriceoftheformula.
• Cost of medications: the cost of the materials used for drug administration, whether by infusion pump or direct administration, was calculated.It wasalso veri-fied,throughthenursingstaff,thedurationofantibiotics anddrugsreusedafterthebottleswereopened.Themean costofdrugswasestimatedbasedonMarch2013ANVISA’s price list16 (conformity list), considering the maximum
sellingpricetothegovernment.
• Hospitaldailyrates:consideringtheratesprovidedbythe hospitalaccountingdepartment,direct costswere veri-fied(wages)at thecostcenteroftheneonatalunitand indirectcosts(electricity,water,andsewagesystem),as wellasthecostsofcleaningandofficesuppliesand dis-tributionofcostsfromotherhospitalsectors.
Atthetimeofthestudy,theteamhad54nurses,two phys-icaltherapists, andfive attending physicianswho were included in the hospital cost sheets. As for the other members of the medical staff (assistants, professors, andresidents)andotherprofessionals(speechtherapists, nutritionists,pharmacists,andsocialworkers),theywere notincludedintheunitcostsheets,astheywere employ-ees of the university. Thus, the mean costs during the studyperiodwerecalculatedanddividedbythenumber ofpatientsadmittedtotheunitinthesameperiod, yield-ingadailycostperpatientofUSD142.00.Tocalculatethis costcomponent,thenumberofhospitalizationdayswas multipliedbytheestimatedhospitaldailyrate.
• Totalcost:comprisedtherespiratorycosts,medications, nutritionalcosts, andlaboratory tests,aswell asother costswithbloodtherapy,phototherapy,costofcatheters, surgeries,andothereventualprocedures,inadditionto thehospitalrates.
Table1 Maternaldemographiccharacteristicsandofnewbornsexposedornottoantenatalcorticosteroids(ACS),expressed innumber(%)ormean±standarddeviation.
WithACS
n=170
WithoutACS
n=41
p
Maternalageinyears 29±6 29±8 0.870
N.ofprenatalconsultations 6±3 5±2 0.019
C-sectionbirth 138(81%) 20(48%) <0.001
Caucasianethnicity 104(61%) 19(46%) 0.084
Primigravida 64(37%) 12(29%) 0.315
Hypertensivesyndromes 50(29%) 11(26%) 0.743
Malegender 83(48%) 20(48%) 0.996
Weight(grams) 1302±360 1278±473 0.766
Gestationalage(weeks) 30±2 29±2 0.231
SGA 36(21%) 9(22%) 0.916
SGA,smallforgestationalage.
For the statistical analysis, categorical variables were expressedbythenumberandfrequencyofeacheventinthe studygroups,andcomparedbyPearson’schi-squaredtestor Fisher’sexacttest. Numericalvariableswereexpressedas meansandcomparedbyStudent’st-testorMann---Whitney test, accordingtodatanormality. Tocompare theclinical outcomesbetween the groups withand without ACS, rel-ative risksandconfidence intervalswerecalculated. SPSS (SPSSInc.Released2008.SPSSStatisticsforWindows, ver-sion17.0,IL,USA)andEPIINFO(CentersforDiseaseControl andPrevention,version7,GA,USA)wereusedforthe sta-tistical analysis. Significance level was set at 0.05 for all tests.
Results
Duringthestudyperiod,220neonates between26and 32 completedweeksofGAmettheinclusioncriteria.Ofthese, nine records were lost and 211 (96%) were reviewed, of which170 (80%)receivedatleast onedoseof ACSand 41 (20%)didnotreceivethemedication.Thedemographicdata of the groups are shown in Table 1 and those related to neonatalmorbidityareshowninTable2.
Table3showsthemeanhospitalcostssubdividedamong itsmaincomponents,andalsothemeandaysof hospitaliza-tionintheNICUandintermediatecareunitfortheentire studypopulationandforthesurvivors;thelatterwere sub-dividedbetweenthoseweighinglessthan1000gand1500g andindifferentGAranges.Thecostsofallthecomponents increased asbirth weight and GA decreased. The highest costcomponentwasthatrelatedtostaffsalary,here encom-passedbyhospitaldailyrates.
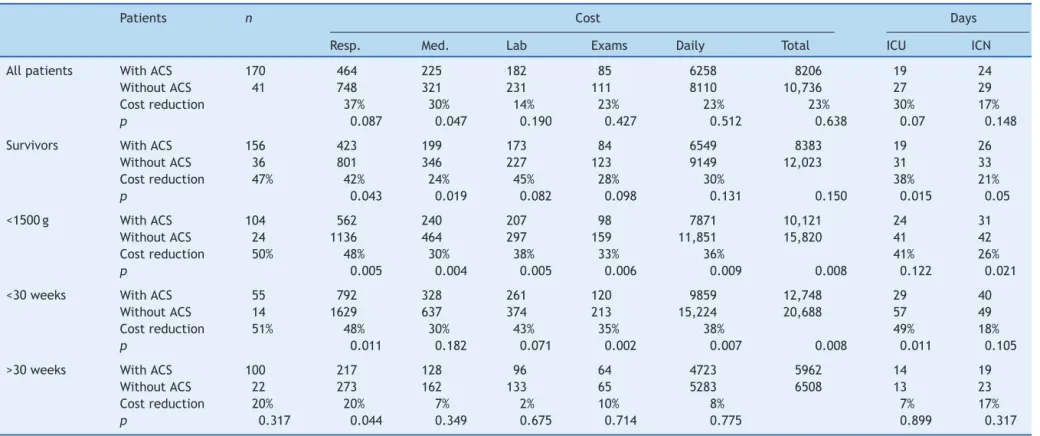
Table4shows thecostsaccordingtoseveralcategories of the analyzed sample, comparing hospital costs among newbornsexposedornottoACS.Fortheentirestudy popula-tion,therewasnocostreductionwithstatisticalsignificance between the groups, although an absolute reduction of 14---37%betweenthedifferentcostcomponentsinpatients receiving ACS was observed. At the analysis of preterm infants that were discharged alive, the group exposed to ACSshowedareductionof24---47%inthevariouscost com-ponents,withstatisticalsignificancefortherespiratoryand
drugcomponentsandsignificantdecreaseinhospitallength ofstay.
The group of newborns with birthweight <1500g, also consideringonlythesurvivors,benefitedthemostfromACS administration,withsignificantreductioninallcost compo-nents,rangingfrom30%to50%,withadecreaseof36%in thetotalcost(p=0.008).ForthegroupofneonateswithGA <30weeksandsurvivors,asignificantreductionofsomeof thecostcomponentsanddecreaseinthetotalcostof38% (p=0.008) wereobserved,accompanied by areductionof 49%indaysofhospitalizationintheNICU(p=0.011).
Discussion
Theresults ofthisstudy showedasignificant reductionin severalcomponentsofhospitalcostsofpreterminfants sub-mittedtoACStherapyinBrazil,whicharemoreevidentin thosewhoweredischargedalive,withbirthweight<1500g, and/orGA<30weeks.Itisnoteworthythat,fromaclinical pointofview,preterminfantsexposedtoACS,when com-paredtothosewhowerenot,hadlessneedforresuscitation inthedeliveryroom,lowerSNAPPEII,18 andlessneed for
mechanical ventilation, similarto the results reported to dateforBrazilianneonates.19
Therefore, this study,a pioneer in a developing coun-trysuchasBrazil,reinforcestheWHOguidelinesinitsaim toreduceneonatalmortality,demonstratingthebenefitsof universalACSforpregnantwomenatriskforpreterm deliv-ery,nowconsideringthefinancialaspectsanddecreasein healthcarecosts.
For four decades, ACS therapy for women at risk of pretermdeliveryhasbeenrecommendedasoneofthemost effective interventions to reduce neonatal mortality and morbidity.5,10Consideringthepreviouslydemonstrated
ben-efits,notusingACSisconsideredbadpracticeindeveloped countries. Therefore, this study had to be retrospective, focusingon the use of healthcare resources and hospital costs.
Withadvancesinneonatalintensive care,preterm sur-vival is increasing, albeit accompanied by an increase in hospital costs. Petrous et al.20 retrieved 19 publications
Table2 Morbidityofnewbornsexposedtoantenatalcorticosteroids(ACS)ornot,expressedinnumbers(%)andrelativerisk with95%confidenceinterval(95%CI).
WithACS
n=170
WithoutACS
n=41
Relativerisk (95%CI)
p
Advancedresuscitationa 27(16%) 14(34%) 0.46(0.26---0.80) 0.007
SNAPPEII>40 14(8%) 8(19%) 0.42(0.18---0.93) 0.033
RDS 90(53%) 27(66%) 0.80(0.61---1.04) 0.135
Surfactantuse 72(42%) 24(58%) 0.72(0.52---0.98) 0.062
Mechanicalventilation 90(53%) 29(70%) 0.74(0.58---0.95) 0.039
Apnea 60(35%) 16(39%) 0.40(0.58---1.39) 0.655
O2at36weeks 24(14%) 9(22%) 0.64(0.32---1.27) 0.215
PDA 48(28%) 13(32%) 0.89(0.52---1.48) 0.660
SurgicalPDA 13(8%) 4(10%) 0.78(0.26---2.27) 0.656
Bloodtransfusion 52(30%) 19(46%) 0.66(0.44---0.98) 0.055
Clinicallate-onsetsepsis 38(22%) 8(19%) 1.14(0.57---2.26) 0.693
PIVHofanygrade 84(49%) 25(60%) 0.81(0.60---1.08) 0.183
PIVHIIIandIV 13(8%) 7(22%) 0.34(0.16---0.75) 0.007
Periventricularleukomalacia 3(1.8%) 2(4.9%) 0.36(0.06---2.09) 0.250
ROP 35(20%) 12(29%) 0.70(0.40---1.23) 0.230
ROPrequiringLaser 5(2.9%) 1(2.4%) 1.20(0.14---10) 0.670
Death 14(8%) 5(12%) 0.67(0.25---1.76) 0.298
SNAPPEII,ScoreforNeonatalAcutePhysiologyPerinatalExtensionII;RDS,respiratorydistresssyndrome;PDA,Patentductusarteriosus;
PIVH,peri-intraventricularhemorrhage;ROP,Retinopathyofprematurity.
aAdvancedresuscitation:needforintubationand/orcardiacmassageand/ormedicationsinthedeliveryroom.
infants and observed huge differences in cost estimates between the studies, making comparisons difficult. The authorsprovideanumberofexplanationsfor this variabil-ity, emphasizing the difference between the time when thestudieswereconductedandgeographicdiversity,which mayreflectvariationsinmedicalpracticesandhealthcare organizations. Nonetheless, there is a consistent inverse associationbetweenhospitalizationcostsandGA or birth-weight,similartotheresultsobtainedinthepresentstudy. In thatreview, theinitial costsof hospitalizationwere shown to be related to preterm mortality, being higher among the survivors. Thus, it was decided that the presentstudywouldmakeseparateanalysesfortheentire
population and for the survivors, taking into account the morbidityandresourceutilizationduringhospitalstay.
Regarding the difference between the several hospi-tal cost components, it was observed that wages and indirectcostsaccountedfor76%ofthetotalcosts,andthe directcosts,for24%;thelatterweredividedintorespiratory costs, 25%; pharmacy, 12%; radiology, 5%; laboratory, 9%; andothers(nutrition,procedures,bloodtherapy,etc.),49%. These results are similarto those obtained when analyz-ing25unitsoftheVermontOxfordnetwork,whichcollects data onpreterminfants whose birth weightislower than 1500g: accommodation costs, which include salaries and costs onequipmentanddaily rates,accounted for 72% of
Table3 AveragecostinUSdollars,subdividedamongitsfivecomponents,daysofintensivecareunit(ICU)stayandmedium risk,withdailycostsfortheentirestudypopulation,forthosethatweredischargedaliveandaccordingtodifferentweightand gestationalageranges.
Patients n Cost(USD) Days Dailycost
Resp. Med. Lab. Exams Dailyhospitalrate Total ICU MR
Entirepopulation 211 520 244 188 90 6618 8698 21 25 188
Survivors 192 494 226 183 92 7036 9065 21 17 238
Birthweight
<1000g 33 1237 409 328 169 12,960 17,076 42 48 189 <1500g 128 670 282 224 109 8618 11,189 27 33 186
GA
26---27weeks 22 1609 612 427 196 14,855 20,150 59 45 193 28---29weeks 48 735 362 236 117 9479 12,369 28 38 187
30weeks 69 292 149 145 72 5596 7075 17 22 181
32weeks 53 142 115 101 55 3819 4739 10 17 175
GA,gestationalage;Resp,respiratorycosts;Med,medicationcosts;Lab,laboratorycosts;Exams,examinationcosts,exceptlaboratory;
corticosteroids
and
cost
of
prematurity
29
Table4 AveragecostinUSdollars,subdividedamongitsfivecomponents,daysofintensivecareunit(ICU)stayandmediumriskforallpatients,forthosethatweredischarged alive,accordingtodifferentweightandgestationalageranges,classifiedaccordingtoexposuretoantenatalcorticosteroids(ACS)ornot.
Patients n Cost Days
Resp. Med. Lab Exams Daily Total ICU ICN
Allpatients WithACS 170 464 225 182 85 6258 8206 19 24
WithoutACS 41 748 321 231 111 8110 10,736 27 29
Costreduction 37% 30% 14% 23% 23% 23% 30% 17%
p 0.087 0.047 0.190 0.427 0.512 0.638 0.07 0.148
Survivors WithACS 156 423 199 173 84 6549 8383 19 26
WithoutACS 36 801 346 227 123 9149 12,023 31 33
Costreduction 47% 42% 24% 45% 28% 30% 38% 21%
p 0.043 0.019 0.082 0.098 0.131 0.150 0.015 0.05
<1500g WithACS 104 562 240 207 98 7871 10,121 24 31
WithoutACS 24 1136 464 297 159 11,851 15,820 41 42
Costreduction 50% 48% 30% 38% 33% 36% 41% 26%
p 0.005 0.004 0.005 0.006 0.009 0.008 0.122 0.021
<30weeks WithACS 55 792 328 261 120 9859 12,748 29 40
WithoutACS 14 1629 637 374 213 15,224 20,688 57 49
Costreduction 51% 48% 30% 43% 35% 38% 49% 18%
p 0.011 0.182 0.071 0.002 0.007 0.008 0.011 0.105
>30weeks WithACS 100 217 128 96 64 4723 5962 14 19
WithoutACS 22 273 162 133 65 5283 6508 13 23
Costreduction 20% 20% 7% 2% 10% 8% 7% 17%
p 0.317 0.044 0.349 0.675 0.714 0.775 0.899 0.317
Resp,respiratorycosts;Med,medicationcosts;Lab,laboratorycosts;Exams,examinationcosts,exceptlaboratory;Daily,dailyhospitalrate;ICUdays,daysofhospitalizationinintensive
thetotalcost,whilethedirectcostsamountedto28% (res-piratory,22%;laboratory,24%;radiology,7%;pharmacy,16%; andothers,31%).21
Some Brazilian publications have analyzed the cost of treatingpreterminfants. In2011,Desgualdoetal.22
eval-uatedhospitalcostsfornewborns with22 to36weeksGA whowereborn in a referral hospitalin SãoPaulo, Brazil. Theauthorsshowedthatthemeancostperdayforpreterm infantswhoseweightwas<1000gwasUSD115.00.
Morerecently,Mwamakambaetal.23estimatedthedirect
hospitalcostsof84preterminfantswith22---36weeksGA, borntoadolescent mothersinatertiarypublichospitalin São Paulo, Brazil. In that study, the highest cost compo-nentwashospitalservices (72%);themean costfor those weighing less than 1000gwas USD 8930.00, witha mean dailycostof USD 157.00.Despite thedifferent methodol-ogy,thedailycostvalue forpreterminfants weighingless than 1000g found in the present study wasestimated at USD189.00,avaluecomparabletothatdescribedby Mwa-makambaetal.,23especiallywhenconsideringthefactthat
thoseauthorsdidnotconsiderindirecthospitalcosts,which maycorrespondto16%ofthetotalcost.
Thereareafewpublicationsintheliteratureshowingthe impactofACSoncostreduction.Thefirstmeta-analysis con-ductedbyCrowleyetal.24 in1990mentionsadecreaseof
USD17,300.00inmeanhospitalcostsassociatedwith ante-natalcorticosteroidtherapy,basedonthefindingsofasingle study.In 1991, Mugford estimated a decrease in hospital costsofpatientswithACS,takingasreferencethecostof careforpatientswithandwithoutrespiratorydistress syn-drome.TheuseofACSforpregnantwomenunder35weeks gestationwouldreducethemeancostperinfantby10%and themeancostpersurvivorby14%.10
The study by Carlan et al.25 estimated a reduction of
resources associated with ACS, with a decrease of seven daysinhospitallengthofstayandofUSD5000.00incosts. Basedonthe studybySimpson &Lynch,12 thecost
reduc-tionestimatepromotedbyACSwas19%.Theresultsofthe present study showed a reduction in hospital costs asso-ciatedwithantenatal corticosteroids ranging from23% to 38%, depending onthe weightand GA, which are consid-erable values that must be considered in an attempt to expandtheprescriptionofACStoBrazilianpregnantwomen at risk of premature birth. Considering the national sce-nario, where approximately 40,000 preterm infants with birth weight <1500g are born annually,26 and basedon a
cost difference of USD 6000 found in this study among very-low birth weight neonates exposed or not to ACS, a decrease in costs of approximately 230 million dollars ayear canbeestimated, iftheantenatalmedication was administered to95% of pregnantwomen withthreatened labor.
It is worth mentioning the study’s limitations regard-ing cost estimates, highlighting the fact that these data are from a single tertiary and teaching hospital, which makesitdifficulttocompareitwithnon-universityand/or smaller hospitals; the lack of a single cost estimate sys-temamongBrazilianpublichospitals;andthesmallsample ofpatients, particularlythelowerGA groups thatdidnot receiveACS.
However,regardingcosts,itcanbestatedthatthereisa hugevariationinthedataanalysismethodsreportedinthe
literature20 andtheobjectivewastoattainan
approxima-tionofhospitalcoststocomparethenewbornsexposedto ACSor tothosewhowerenotexposed.Despitethese lim-itations,itwasapioneeringstudyinBrazil,comparingthe economicimpactofantenatalmedicationaccordingtoWHO guidelinesthat encouragethe useof simpleandeffective technologiesin lowandmiddle-incomecountriestoreach theglobal aimof reducingneonatalmortalitybythe year 2035.
ItcanbeconcludedthattheuseofACSisasimple mea-sure thatcontributestoreduce prematuritycomplications andtheuseofhealthresources,reducinghospitalcostsfor preterminfantswithGAbetween26and32weeksinBrazil. This effectis predominant among thoseweighing <1500g and/or under30 weeks GAwhosurvive until hospital dis-charge.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.BryceJ,VictoraCG,BlackRE.Theunfinishedagendainchild survival.Lancet.2013;382:1049---59.
2.JamisonDT,SummersLH,AlleyneG,ArrowKJ,BerkleyS, Binag-wahoA,etal.Globalhealth2035:aworldconvergingwithina generation.Lancet.2013;382:1898---955.
3.UnitedNationsChildren’sFund(UNICEF),WorldHealth Orga-nization (WHO), The World Bank, UnitedNations Population Division.TheInter-agencyGroupforChildMortalityEstimation (UNIGME).Levelsandtrendsinchildmortality.Report2013. NewYork,USA:UNICEF;2013.
4.LawnJE,BlencoweH,OzaS,YouD,LeeAC,WaiswaP,etal. Everynewborn:progress,priorities,andpotentialbeyond sur-vival.Lancet.2014;384:189---205.
5.RobertsD,Dalziel S.Antenatal corticosteroidsfor accelerat-ingfetallungmaturationforwomenatriskofpretermbirth. CochraneDatabaseSystRev.2006;(3):CD004454.
6.Mwansa-KambafwileJ,CousensS,HansenT,LawnJE. Antena-talsteroidsinpretermlabourfor thepreventionofneonatal deathsduetocomplicationsofpretermbirth.IntJEpidemiol. 2010;39:i122---33.
7.RedeBrasileiradePesquisasNeonatais.Relatórioanual2012.
Brasil;2012. Available from: http://redeneonatal.fiocruz.br/
images/stories/relatorio/rbpn2012.pdf[accessed10.03.2014]. 8.SadeckLS,LeoneCR,ProcianoyRS,GuinsburgR,MarbaST, Mar-tinezFE,etal.Effectsoftherapeuticapproachontheneonatal evolutionofverylowbirthweightinfantswithpatentductus arteriosus.JPediatr(RioJ).2014;90:616---23.
9.BhuttaZA,DasJK,BahlR,LawnJE,SalamRA,PaulVK,etal. Canavailableinterventionsendpreventable deathsin moth-ers,newbornbabies,andstillbirths,andatwhatcost?Lancet. 2014;384:347---70.
10.MarchofDimes,PMNCH,Savethechildren,WHO.Borntoosoon: theglobalactionreportonpretermbirth.Geneva:WHO;2012. 11.MugfordM,PiercyJ,ChalmersI.Costimplicationsofdifferent approachestothepreventionofrespiratorydistresssyndrome. ArchDisChild.1991;66:757---64.
13.ChungCS,MyrianthopoulosNC.Congenitalanomalies: mortal-ityandmorbidity,burdenandclassification.AmJMedGenet. 1987;27:505---23.
14.Brasil.Ministério da Saúde. Secretariade Atenc¸ãoda Saúde (CNESNet).Brasil:Ministério daSaúde;2013.Available from: http://cnes.datasus.gov.br[accessed07.08.14].
15.XuX,GrossettaNardiniHK,RugerJP.Micro-costingstudiesinthe healthandmedicalliterature:protocolforasystematicreview. SystRev.2014;3:47.
16.Brasil.MinistériodaSaúde.AgênciaNacionaldeVigilância San-itária.Pediatria:prevenc¸ãoecontroledainfecc¸ãohospitalar. Brasília:MinistériodaSaúde;2005.
17.Internal Revenue Service of the USA (IRS). Yearly aver-age exchange rates for converting foreign currencies into U.S. dollars. Available from: http://www.irs.gov/business/ small/international/article[accessed07.08.14].
18.RichardsonDK,CorcoranJD,EscobarGJ,LeeSK.SNAP-IIand SNAPPE-II:simplifiednewbornillnessseverityandmortalityrisk scores.JPediatr.2001;138:92---100.
19.RedeBrasileiradePesquisasNeonatais.Usoantenatalde cor-ticosteróideeevoluc¸ãoclínicaderecém-nascidospré-termo.J Pediatr(RioJ).2004;80:277---84.
20.PetrouS,EddamaO, ManghamL.Astructuredreviewofthe recent literatureon theeconomic consequences ofpreterm birth.ArchDisChildFetalNeonatalEd.2011;96:F225---32. 21.RogowskiJ.Measuringthecostofneonatalandperinatalcare.
Pediatrics.1999;103:329---35.
22.DesgualdoCM,RieraR,ZucchiP.Costestimateofhospitalstays forprematurenewbornsinapublictertiaryhospitalinBrazil. Clinics(SaoPaulo).2011;66:1773---7.
23.MwamakambaLW,ZucchiP.Costestimateofhospitalstaysfor prematurenewbornsofadolescentmothersinaBrazilianpublic hospital.Einstein(SaoPaulo).2014;12:223---9.
24.Crowley P, Chalmers I, Keirse MJ. The effects of corticos-teroid administration before preterm delivery: an overview oftheevidencefromcontrolledtrials.BrJObstetGynaecol. 1990;97:11---25.
25.CarlanSJ,ParsonsM,O’Brien WF,KrammerJ.Pharmacologic pulmonarmaturationinpretermprematurerupture of mem-branes.AmJObstetGynecol.1991;164:371---80.