w w w . r b o . o r g . b r
Original
article
Measurement
of
the
tendon
of
the
biceps
brachii
after
tenotomy:
study
on
cadavers
夽
Anderson
Cunha
Machado,
Fabiano
Rebouc¸as
Ribeiro,
Samuel
Machado
Martins
∗,
Rômulo
Brasil-Filho,
Antonio
Carlos
Tenor-Junior,
Miguel
Pereira
da
Costa
HospitaldoServidorPúblicoEstadualdeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received28April2014 Accepted29July2014 Availableonline3July2015
Keywords:
Shoulderjoint Glenoidcavity Tenotomy
a
b
s
t
r
a
c
t
Objective:Toevaluatetheinfluenceofelbowandforearmrangeofmotiononthedistal excursionofthelongheadofthebiceps(LHB).
Methods:ThedistalexcursionoftheLHBaftertenotomyoftheshouldersofeightcadavers wasascertainedbymeasuringthedistancebetweenapointmarkedoutontheLHB,3cm fromtheanterolateralborderoftheacromion,anditspositionatdifferentdegreesofelbow flexion,usingadigitalpachymeter.Themeasurementsatelbowflexionof135◦,90◦,45◦and 0◦werenoted:theseangleswereestablishedusingagoniometer.Themeasurementswere madewiththeforearminneutral,supinationandpronationpositions.
Results:DifferencesbetweenthemeanmeasurementsofthedistalexcursionoftheLHB (totalsample)wereobservedbetweenthedegreesofelbowflexion(p<0.01).However,no statisticaldifferenceswereobservedbetweenthedifferentforearmpositions,betweenthe sides,gendersandagesofthecadaversstudied.
Conclusion: Progressiveextensionoftheelbowcausedprogressivedistalexcursionofthe LHB,butwithoutinterferenceintheforearmposition,gender,sideorageofthecadavers studied.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Mensurac¸ão
do
tendão
do
bíceps
braquial
após
tenotomia:
estudo
em
cadáveres
Palavras-chave:
Articulac¸ãodoombro Cavidadeglenoide Tenotomia
r
e
s
u
m
o
Objetivo:Avaliarainfluênciadaamplitudedemovimentodocotoveloedoantebrac¸ona excursãodistaldacabec¸alongadobíceps(CLB).
Métodos:Verificou-seaexcursãodistaldacabec¸alongadobíceps(CLB)apóstenotomiaem ombrosdeoitocadáveres,pormeiodaaferic¸ãodadistânciaentreumpontodemarcadona cabec¸alongadobíceps(CLB)a3cmdabordaanterolateraldoacrômioemflexãomáximae
夽
WorkperformedwithintheShoulderandElbowGroup,OrthopedicsandTraumatologyService,HospitaldoServidorPúblicoEstadual, SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](S.M.Martins).
http://dx.doi.org/10.1016/j.rboe.2015.06.012
Foramanotadasasmedidasnosgrausdeflexãodocotovelo135,90 ,45 e0,estabelecidas comousodeumgoniômetro.Asmedidasforamtomadascomoantebrac¸oemposic¸ão neutra,supinac¸ãoepronac¸ão.
Resultados:Observou-sediferenc¸aentreasmédiasdasmedidasdaexcursãodistaldacabec¸a longadobíceps(CLB)(amostratotal)entreosgrausdeflexãodocotovelo(p<0,01).Todavia, nãofoiencontradadiferenc¸aestatísticaentrediferentesposic¸õesdoantebrac¸o,entreos lados,gêneroseidadesdoscadáveresestudados.
Conclusão: Aextensãoprogressivadocotoveloocasionouaexcursãodistalprogressivada cabec¸alongadobíceps(CLB),masseminterferênciadaposic¸ãodoantebrac¸o,gênero,lado eidadedoscadáveresestudados.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Thelongheadofthetendonofthebicepsbrachiimuscle(LHB) isdevelopedataroundtheseventhtoeighthweekofgestation anditbecomesdifferentiatedstartingfromthemesoderm.It isdescribedascontinuouswiththelabrumoftheglenoidand thesupraglenoidtubercle,anditpassesanteriorlyand supe-riorlytotheheadofthehumerusbeforeenteringthebicipital groove.1,2Itisintra-articularandextrasynovialandslides pas-sivelyovertheheadofhumerusduringabductionorrotation. Itslengthis9cmanditsdiameteris5–6mm.Itinnervationis throughanetworkofsensoryfibersofthesympathetic ner-voussystem.3–5
Thebicepsextendsfromthescapulatotheforearmand hasfunctionsrelatingtotheshoulderandelbow.Itsfunction relatingtotheelbowhasbeenwellestablishedandincludes bothflexionandsupination.Ontheotherhand,inrelationto theshoulder,althoughseveralfunctionshavebeenattributed, theexactroleoftheLHBremainsamatterofcontroversy.6 ElectromyographicanalyseshaveshownthattheLHBserves asastabilizerinunstablejoints,butnotinstableshoulders.7 Biomechanical studies have demonstrated that the tendon actsasadynamicdepressoroftheheadofthehumerus,but thishasnotbeenprovenclinically.8,9 Kuhnet al.10 demon-strateditsimportanceasarestrictorofexternalrotationof theabductedarm.
Lesionsofthesuperiorglenoidthat involvetheLHB are called SLAP lesions (superior labrum, anterior and poste-rior).Theywerefirstdescribedatthebeginningofthe1990s by Snyder et al.11 The conservative or surgical treatment forthese lesions hasbeen well established, but there has neverbeenaconsensusregardingthepostoperative rehabili-tationtreatment.Thereareprotocolsdescribedinthecurrent literature,12,13inwhichearlymobilityoftheextendedelbowis avoidedbecauseofdoubtsregardingtheconsequent tension-ingoftheproximalLHBandsuperiorglenoidlabrum,which were reinserted during the operation. These actionscould causefailureofhealingandanewinjury.12,13
Theobjectiveofthisstudywastoevaluatetheinfluence oftherangeofmotionoftheelbowandforearmonthedistal excursionoftheLHB.
Methods
Thisstudywasapprovedbyourinstitution’sresearchethics committee (number: CAAE 19893114.6.0000.5463). Sixteen shouldersofeightcadaversobtainedfromtheDeath Verifi-cationServiceoftheUniversityofSãoPaulo(SVOC-USP)were dissected.Noneofthesecadaverspresentedanyfracturesof theupperlimbs,localdeformitiesorscarring.Thedissections wereperformedbymeansofananterolateralaccess measur-ing10cm(Fig.1A),followedbydissectionbetweentheanterior andlateraldeltoidmuscle(Fig.1B)soastoapproachand dis-secttheLHB(Fig.1C).
Usingasurgicalpen,alineperpendiculartotheLHBwas marked out,3cmdistallytotheanterolateralborderofthe acromion.TenotomyoftheLHBwasperformedatitsoriginin thesupraglenoidtubercle,withtheelbowatmaximum flex-ion.ThedistalexcursionoftheLHBwasverifiedbymeasuring the distance betweenthe linemarked out on the bicipital tendonandneedlesplacedattheedgeofthelinepreviously establishedontheLHB,usingadigitalpachymeter(LeeTools, Houston,USA)(Fig.1D),astheelbowwasextended. Measure-mentswerenotedatthefollowingdegreesofelbowflexion: 135◦,90◦,45◦and0◦,whichwereestablishedusinga
goniome-ter.Themeasurementsweremadewiththeforearminthe neutral,supinationandpronationpositions.
Statisticalanalysis
Tocomparetheresultsfromthemeasurementsonthe dis-tal excursion of the LHB, the Friedman test was used. To determinethemeasurementsbetweenwhichstatistically sig-nificantdifferencesoccurred,theWilcoxontestwasused.For allthetests,therejectionlevelforthehypothesisofnullity was0.05(significancelevelof95%).
Fig.1–Tenotomyprocedureonacadaver.(A)Markingouttheboneanatomicalparametersandaccessroute;(B)accessvia anterolateralroute;(C)dissectionoftheLHBfromitsgroovetoitsoriginintheglenoid;(D)measurementoftheexcursionof theLHBafterproximaltenotomy,withelbowflexionat135◦,90◦,45◦and0◦.
Results
Amongthe eightcadaversdissected, five were female and threeweremale.Therewereeightrightshouldersandeight leftshoulders(Table1).Themeanvalueforthedistal excur-sionoftheLHBwiththeforearmintheneutralpositionand at135◦ofelbowflexionwas1.41mm;at90◦,13.97mm;at45◦,
18.01mm;andat0◦,22.53mm(Table2).Whenthese
measure-mentsweremadewiththeforearmmovedintopronationand
supinationpositions,therewerenodifferencesinrelationto theabovemeasurements.
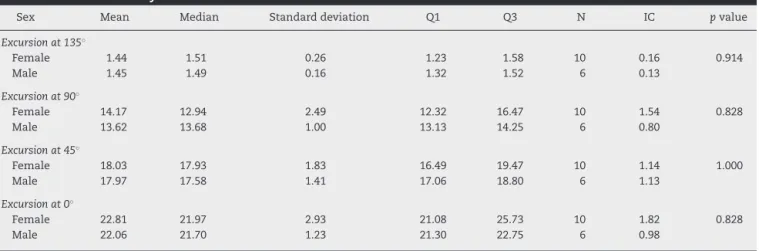
Comparisons between the measurements on the distal excursionoftheLHBshowedsignificantdifferences(p<0.001), consideringtheentiresample,atalldegreesofelbowflexion (Table2).Ontheotherhand,therewerenostatistical differ-encesbetweentherightandleftsides(Table3),betweenthe maleandfemalesexes(Table4)orbetweentheages(Table5), amongthecadaversstudied.
Table1–Measurements(inmm,usingadigitalpachymeter)ofthedistalexcursionatelbowflexionsof135◦,90◦,45◦
and0◦(anglesobtainedbymeansofagoniometer).
Cadaver Age Sex Side Excursionat135◦ Excursionat90◦ Excursionat45◦ Excursionat0◦
1 76 F R 1.51 17.59 19.08 25.62
L 1.45 15.16 21.16 25.76
2 72 F R 1.88 12.15 17.53 21.13
L 0.99 12.84 18.32 21.06
3 64 M R 1.25 13.13 19.06 23.07
L 1.66 14.25 20.15 23.99
4 75 F R 1.58 12.88 16.5 22.54
L 1.57 11.98 15.84 21.4
5 58 M L 1.48 14.85 16.41 21.63
R 1.52 14.23 17.02 20.73
6 72 F R 1.6 17.9 19.76 26.43
L 1.51 16.9 19.6 26.12
7 69 M R 1.27 12.14 17.16 21.19
L 1.5 13.13 18 21.77
8 88 F R 1.15 13 16.49 19.18
L 1.16 11.31 16.02 18.85
Table2–StatisticalanalysisonthemeasurementsofthedistalexcursionoftheLHBinrelationtothetotalsample.
Totalsample General
135◦ 90◦ 45◦ 0◦
Mean 1.44 13.97 18.01 22.53
Median 1.51 13.13 17.77 21.70
Standarddeviation 0.22 2.03 1.64 2.41
Q1 1.27 12.67 16.50 21.11
Q3 1.57 14.93 19.21 24.40
N 16 16 16 16
IC 0.11 1.00 0.80 1.18
Side Mean Median Standarddeviation Q1 Q3 N IC pvalue
Excursionat135◦
Right 1.47 1.52 0.24 1.27 1.59 8 0.16 0.495
Left 1.42 1.49 0.22 1.38 1.53 8 0.16
Excursionat90◦
Right 14.13 13.07 2.33 12.70 15.07 8 1.61 0.875
Left 13.80 13.69 1.84 12.63 14.93 8 1.27
Excursionat45◦
Right 17.83 17.35 1.29 16.89 19.07 8 0.89 0.916
Left 18.19 18.16 2.00 16.31 19.74 8 1.39
Excursionat0◦
Right 22.49 21.87 2.49 21.03 23.71 8 1.72 0.834
Left 22.57 21.70 2.50 21.32 24.43 8 1.73
Table4–StatisticalanalysisonthemeasurementsofthedistalexcursionoftheLHBinrelationtosex.
Sex Mean Median Standarddeviation Q1 Q3 N IC pvalue
Excursionat135◦
Female 1.44 1.51 0.26 1.23 1.58 10 0.16 0.914
Male 1.45 1.49 0.16 1.32 1.52 6 0.13
Excursionat90◦
Female 14.17 12.94 2.49 12.32 16.47 10 1.54 0.828
Male 13.62 13.68 1.00 13.13 14.25 6 0.80
Excursionat45◦
Female 18.03 17.93 1.83 16.49 19.47 10 1.14 1.000
Male 17.97 17.58 1.41 17.06 18.80 6 1.13
Excursionat0◦
Female 22.81 21.97 2.93 21.08 25.73 10 1.82 0.828
Male 22.06 21.70 1.23 21.30 22.75 6 0.98
Table5–Statisticalanalysisonthemeasurementsofthe distalexcursionoftheLHBinrelationtoage.
Age
Corr pvalue
Excursionat135◦ −21.6% 0.422
Excursionat90◦ −19.7% 0.466
Excursionat45◦ −12.2% 0.653
Excursionat0◦
−8.9% 0.742
Discussion
Thisstudyisinagreementwiththestudyconductedby Gram-stadetal.,14withevidenceofincreasingdistalexcursionofthe LHBastheelbowisextended.Ontheotherhand,accordingto thoseauthors,notonlyelbowextensionbutalsopronationof theforearmwasassociatedwithincreasedtensionontheLHB, andonthesuperiorlabrumoftheglenoid.Inourobservations, nodifferencesindistalexcursionoftheLHBwereseenwith regardtothepositioningoftheforearm(pronationor supina-tion).Thisdifferenceinresultscanpossiblybeexplainedby thefactthatthoseauthors madetheirmeasurementswith theshoulderabductedat60◦,whereasinourstudy,the
mea-surementsweremadewiththeshoulderadductedagainstthe body.
AccordingtoWilketal.,13inpostoperativetreatmentfor SLAPlesions,activeandpassiveelbowextensionexercisesare indicatedstartinginthefirsttendaysaftertheoperation,only forpatientswhounderwentsimpledebridement(typesIand IIIofSnyder’sclassification).However,amongpatientswho underwentrepairstoSLAPlesions(typesIIandIVofSnyder’s classification),earlycompleteextensionoftheelbowandthe consequentproximalbicipitaltensioningshouldbeavoided. Thisguidanceisconcordantwiththefindingsfromourstudy, sincegreater distalexcursionoftheLHB aftertenotomyat itsorigin wasdemonstratedastheelbowwasprogressively extended.
Conclusions
AftertenotomyattheoriginoftheLHB,progressiveextension oftheelbowcausedprogressivedistalexcursionoftheLHB, butwithoutinterferencefromthepositionoftheforearmor fromthesex,sideorageofthecadaversstudied.
Conflicts
of
interest
Acknowledgements
TheauthorsthanktheorthopedicsteamatHospitaldo Servi-dorPúblico Estadual,SãoPaulo,andthe teamoftheDeath VerificationServicefortheirsupportincarryingoutthisstudy.
r
e
f
e
r
e
n
c
e
s
1. GardnerE,GrayDJ.Prenataldevelopmentofthehuman shoulderandacromioclavicularjoints.AmJAnat. 1953;92(2):219–76.
2. JobeC.Grossanatomyoftheshoulder.In:RockwoodC,editor. Theshoulder.Philadelphia:Elsevier;2009.
3. HitchcockHH,BechtolCO.Painfulshoulder:observationson theroleofthetendonofthelongheadofthebicepsbrachiiin itscausation.JBoneJointSurgAm.1948;30(2):263–73.
4. AlpantakiK,McLaughlinD,KaragogeosD,HadjipavlouA, KontakisG.Sympatheticandsensoryneuralelementsinthe tendonofthelongheadofthebiceps.JBoneJointSurgAm. 2005;87(7):1580–3.
5. BeyMJ,EldersGJ,HustonLJ,KuhnJE,BlasierRB,SoslowskyLJ. Themechanismofcreationofsuperiorlabrum,anterior,and posteriorlesionsinadynamicbiomechanicalmodelofthe shoulder:theroleofinferiorsubluxation.JShoulderElbow Surg.1998;7(4):397–401.
6.SethiN,WrightR,YamaguchiK.Disordersofthelongheadof thebicepstendon.JShoulderElbowSurg.1999;8(6):644–54.
7.KimSH,HaKI,KimHS,KimSW.Electromyographicactivityof thebicepsbrachiimuscleinshoulderswithanterior
instability.Arthroscopy.2001;17(8):864–8.
8.KumarVP,SatkuK,BalasubramaniamP.Theroleofthelong headofbicepsbrachiiinthestabilizationoftheheadofthe humerus.ClinOrthopRelatRes.1989;244:172–5.
9.WarnerJJ,McMahonPJ.Theroleofthelongheadofthebiceps brachiiinsuperiorstabilityoftheglenohumeraljoint.JBone JointSurgAm.1995;77(3):366–72.
10.KuhnJE,HustonLJ,SoslowskyLJ,ShyrY,BlasierRB.External rotationoftheglenohumeraljoint:ligamentrestraintsand muscleeffectsintheneutralandabductedpositions.J ShoulderElbowSurg.2005;141SupplS:39S–48S.
11.SnyderSJ,KarzelRP,DelPizzoW,FerkelRD,FriedmanMJ. SLAPlesionsoftheshoulder.Arthroscopy.1990;6(4):274–9.
12.AndrewsJR,CarsonWG,McLeodWD.Glenoidlabrumtears relatedtothelongheadofthebiceps.AmJSportsMed. 1985;13(5):337–41.
13.WilkKE,ReinoldMM,DugasJR,ArrigoCA,MoserMW, AndrewsJR.Currentconceptsintherecognitionand treatmentofsuperiorlabral(SLAP)lesions.JOrthopSports PhysTher.2005;35(5):273–91.