BrazJOtorhinolaryngol.2015;81(1):115---116
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
www.bjorl.org
CASE
REPORT
Lemierre’s
syndrome:
a
pharyngotonsillitis
complication
夽
,
夽夽
Síndrome
de
Lemierre:
uma
complicac
¸ão
de
faringotonsilite
Pedro
Ernesto
Barbosa
Pinheiro
∗,
Priscilla
Durante
Miotto,
Natalia
Quinhone
Shigematsu,
Edwin
Tamashiro,
Fabiana
Cardoso
Pereira
Valera,
Wilma
Teresinha
Anselmo-Lima
DepartmentofOphthalmology,OtorhinolaryngologyandHeadandNeckSurgery,SchoolofMedicineofRibeirãoPreto,University ofSãoPaulo,RibeirãoPreto,SP,Brazil
Received21September2014;accepted17October2014 Availableonline21November2014
Introduction
Lemierre’ssyndrome(LS)isarareandserious pharyngoton-sillitiscomplicationthatusuallyoccursinadolescentsand youngadultscausedbyanaerobicbacteria,morespecifically attributedtoFusobacteriumnecrophorum.Firstdescribed intheearlytwentiethcentury,itwasin1936thattheFrench microbiologist,Dr.AndréLemierre,outlinedthe character-isticsofthedisease.1
Case
report
Afemalepatient(K.C.O.),12yearsold,previouslyhealthy,
presented withsore throatand fever for seven days.She
wasdiagnosedinanothercenterwithpharyngotonsillitisand
receivedintramuscularBenzathinebenzylpenicillin,
evolv-ingwithpainimprovement,butwiththeonsetofpersistent
夽 Pleasecitethisarticleas:PinheiroPE,MiottoPD,Shigematsu NQ, Tamashiro E, Valera FC, Anselmo-Lima WT. Lemierre’s syn-drome:apharyngotonsillitiscomplication.BrazJOtorhinolaryngol. 2015;81:115---6.
夽夽
Institution:FaculdadedeMedicinadeRibeirãoPretoda Uni-versidadedeSãoPaulo(USP),RibeirãoPreto,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](P.E.B.Pinheiro).
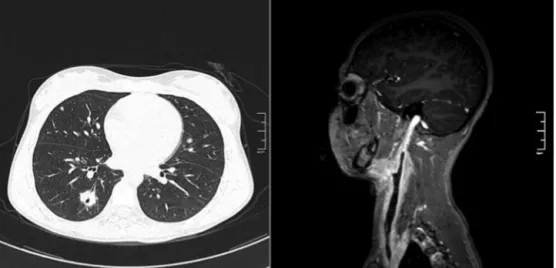
high temperature and bulging in the right anterior
cervi-calregionfor threedays.Hyperemiawasobserved inthe
oropharynxandcervicalbulgingontopographyoftheright
sternocleidomastoidmuscle,painfulonpalpation.Contrast
tomographyandangiographyshowrightperitonsillar
inflam-mation,thrombosisofrightinternaljugularvein(IJV),and
pulmonarynodulesconsistentwithmicroabscesses(Fig.1).
Initially,thediagnosisofLSwasnotconsidered,and
intra-venousantibiotictherapywasstartedwithamoxicillinand
clavulanate at a dose 90mg/kg/day, and anticoagulation
withenoxaparinandwarfarin,withgradualclinical
improve-ment.Afterthreedays,withthefinaldiagnosisestablished
andinconjunctionwiththeHospitalInfectionControl
Com-mittee,weoptedtokeeptheregimenduetoimprovement
inclinicalandlaboratoryparameters.Evenwiththepatient
being admitted on antibiotics, samples for general and
anaerobic bacteria cultures were harvested; however, no
bacterialgrowthwasobserved.Thepatientwasdischarged
after14 days of hospitalization, asymptomatic, with
pre-scribed oral antibiotics tocomplete 21 daysof treatment
andoralanticoagulationtherapy.Afterfourmonthsof
anti-coagulationtherapy,a controlresonanceangiography was
performedtomonitor thedisease, showingpersistenceof
IJV thrombosis. The patient remains on anticoagulation
medicationonregularclinicalvisitsbasis,withfollowupby
Otolaryngology,PediatricHematologyandVascularSurgery
teams.
http://dx.doi.org/10.1016/j.bjorl.2014.10.004
116 PinheiroPEetal.
Figure 1 Left, Cross-Sectional Computed Tomography showing pulmonary microabscesses. Right, Post-contrast Sagittal T1-weightedMagneticRessonanceAngiography,showingtheRightInternalJugularVeinfillingfailure.
Discussion
F. necrophorum is a Gram-negative anaerobic bacteria of
theoropharyngeal floracapable of causing primary
infec-tioninhealthyindividualswithintactanatomicalbarriers.
Thecondition begins witha sorethroatandprogresses to
impairment of peritonsillar tissue, parapharyngeal space,
IJVthrombophlebitisand,finally,septicemboliformation.2
The onset of sepsis occurs with marked fever (39---41◦C,
102---106◦F),typically4---5daysafterthestartofsorethroat
and sometimes after improvement of the symptom.2 The
appearanceofthejawanglebulging,orparalleltothe
stern-ocleidomastoidmuscle,clinicallyreflectsthrombophlebitis.
Lungsaretheprimarysiteof abscessformation secondary
to septic emboli; however, one can find multiple organ
involvement.2,3 LS diagnosis involves: (1) recent
orophar-ynx infection; (2) clinical or radiological evidence of IJV
thrombosis;(3)isolationofanaerobicpathogens;(4)atleast
one septic focus.4 There is controversy in the literature
regardingtheclassificationofcasesinwhichthepathogen
cannotbeisolated.2,3 However,considering thatthereare
negativeculturesin12%ofthecases,3facedwiththeclinical
conditionandthedifficultyofbacterialgrowthinpatients
duringantibiotictherapy,wemaintainedthediagnosisand
management in this case. Treatment includes antibiotics
for 3---6 weeks, with coverage for anaerobes.5
Anticoagu-lationtherapyiscontroversial,butitiswidelyused.Inthe
absenceof contraindications,thetherapymustbe
consid-ered, especiallyin patients withpoor clinical responsein
spiteofantibiotic.6
Final
comments
Aftertheadventofantibiotics,casesofLSpractically
dis-appeared,butthereis evidenceofitsincreasedincidence
in recent years, possibly associated with reduced use of
antibioticsforsorethroat.DescribedbyAndréLemierreas
a‘‘syndromethatissocharacteristicthatmistakeisalmost
impossible’’,1thisconditionispotentiallyasseriousasitis
potentiallytreatable.3Ahighdegreeofsuspicioniscrucial
toavoid a delayed diagnosis with potentially fatal
conse-quences.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.LemierreA.Oncertainsepticaemiasduetoanaerobicorganisms. Lancet.1936;1:701---3.
2.BaigM,RasheedJ,SubkowitzD,VieiraJ.Areviewoflemierre syndrome.InternetJInfectDis[serialonline].2005;5.Available from:http://ispub.com/IJID
3.RiordanT,WilsonM.Lemierre’ssyndrome:morethanahistorical curiosa.PostgradMedJ.2004;80:328---34.
4.AsnaniJ,JonesS.Casereview.JFamPract.2014;63:193---6. 5.KarkosPD,AsraniS,KarkosCD,LeongSC,TheochariEG,
Alex-opoulou TD, et al. Lemierre syndrome: a systematic review. Laryngoscope.2009;119:1552---9.