w w w . r b o . o r g . b r
Original
article
Fractures
of
the
distal
clavicle:
comparison
between
two
surgical
treatment
methods
夽
José
Carlos
Souza
Vilela
a,
Ronaldo
Percopi
de
Andrade
b,
Lucas
Braga
Jacques
Gonc¸alves
b,
Thalles
Leandro
Abreu
Machado
a,∗,
Mario
Roberto
Chaves
Correa
Filho
a,
Ivana
Duval
de
Araujo
caHospitaldaUnimeddeBeloHorizonte,BeloHorizonte,MG,Brazil
bHospitalMadreTeresa,BeloHorizonte,MG,Brazil
cUniversidadeFederaldeMinasGerais,BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received22January2014 Accepted22April2014 Availableonline30March2015
Keywords:
Bonefractures Clavicle Fracturefixation
a
b
s
t
r
a
c
t
Objective:Tocomparetheclinicalandradiographicresultsfromosteosynthesisoffractures ofthelateralthirdoftheclavicle,usingtwomethods:Tplatesoranchorstogetherwith Kirschnerwires.
Methods:Fifteenpatientsofmeanage34.3years(range:19–57)andmeanfollow-up22.7 months(range:14–32)wereevaluated.Inninecases,aTplatewasused;andinsixcases, coracoclavicularfixationwasusedwithanchorsinthecoracoidprocessandKirschnerwires throughtheacromioclavicularjoint.TheevaluationincludedtheConstantscore,personal satisfactionandradiographicassessment.
Results:Bothtypesoftreatmentachievedconsolidationinallcases.Group1presenteda higherConstantscore(83.4)thanthatofGroup2(76.4)(p=0.029).Neitherofthetechniques presentedanyseverecomplications,andmildcomplicationswereonlyobservedinGroup 2(80%),mostlyconsistingofmigrationoftheKirschnerwireandsuperficialinfection.
Conclusion:SurgicaltreatmentoffracturesofthedistalclavicleusingTplatesprovidedthe sameconsolidationrateasshownbycoracoclavicularfixationwithanchorsinthecoracoid processandKirschnerwiresthroughtheacromioclavicularjoint,andbetterclinicalresults.
Levelofevidence:LevelIIIevidencewasobtained.Comparativeretrospectivestudyand ther-apeuticstudywereperformed.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkdevelopedattheOrthopedicsandShoulderandElbowSurgeryService,UnimedHospitalofBeloHorizonte,andatHospital RisoletaTolentinoNeves,BeloHorizonte,MG,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](T.L.A.Machado).
http://dx.doi.org/10.1016/j.rboe.2015.03.006
Fraturas
da
clavícula
distal:
comparac¸ão
de
dois
métodos
de
tratamento
cirúrgico
Palavras-chave:
Fraturasósseas Clavícula Fixac¸ãodefratura
r
e
s
u
m
o
Objetivo: Compararosresultadosclínicoseradiográficosdaosteossíntesedefraturasdo terc¸olateralda clavículacomdoismétodos:placaTouâncorasassociadas aosfios de Kirschner.
Métodos: Foramavaliados15pacientescommédiadeidadede34,3anos(19–57)e segui-mentomédiode22,7meses(14–32).EmnovecasosfoiusadaaplacaTeemseiscasos afixac¸ãocoracoclavicularcomâncorasnoprocessocoracoideefiosdeKirschneratravés daarticulac¸ãoacromioclavicular(AC).Aavaliac¸ãoincluiuoescoredeConstant,satisfac¸ão pessoaleavaliac¸ãoradiográfica.
Resultados: Ambasasmodalidadesdetratamentoobtiveramconsolidac¸ãoemtodos os casos.OGrupo1apresentouescoredeConstantmaiselevado(83,4)quandocomparadocom oGrupo2(76,4)p=0,029.Nenhumadastécnicasapresentoucomplicac¸õesgraves,embora complicac¸õeslevestenhamsidoobservadasapenasnoGrupo2(80%),amaioriadelasa migrac¸ãodofiodeKirschnereinfecc¸ãosuperficial.
Conclusão: OtratamentocirúrgicodasfraturasdaclavículadistalcomplacaTproporciona amesmataxadeconsolidac¸ãodafixac¸ãocoracoclavicularcomâncorasnocoracoideefios deKirschneratravésdaarticulac¸ãoACemelhoresresultadosclínicos.
Níveldeevidência: NívelIII,estudoretrospectivocomparativo,estudoterapêutico.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Fractures ofthe distalextremityof theclavicle are a diffi-cultandcontroversialprobleminclinicalpractice.1–5 These
injuries are not uncommon and account for 20% of all fractures ofthe clavicle.3,4,6–9 Most authors agreewith the
indicationofsurgicaltreatment,becauseofthehighrateof non-consolidation,whichmay reach 33%,withconsequent pain and functional incapacity.2,5,7,10,11 The causes of this
rateofnon-consolidationaremechanicalandanatomical.The trapeziusandsternocleidomastoidpullthemedialfragment superiorlyandposteriorlyandtheweightofthearmdisplaces thelateralfragmentdistally.Thesmallsizeofthedistal frag-mentandtheplanarshapeoftheclaviclemakebonecontact difficultandimpedeconsolidation.1–3,12
Several techniques for fixation of these fractures have been described in the literature. They include use of Kirschnerwires,use oftensionbands,coracoclavicular fix-ation using sutures or screws, acromioclavicular fixation and,lastly, costly plates that have been specifically devel-oped for these fractures, such as hook plates and locked plates.Despitethe highconsolidationratesachieved, most ofthesetechniquesare associatedwith complicationsand several ofthese routinely require removal ofthe material. Themostfrequentcomplicationsareinfection,skinirritation, degenerativeacromioclavicularalterationsandperiprosthetic fractures.4,5,12–14
Theidealfixationmethodshouldprovidestabilityforthe periodoftimeneededforconsolidation,causefewor prefer-ably no complications and should not require subsequent removalofthematerial.
The present study retrospectively reviewed the clinical resultsfromtwosurgicaltechniques:fixationusingaTplate and coracoclavicular fixation using anchors and Kirschner wiresthroughtheacromioclavicularjoint,inacutedisplaced fracturesofthedistalclavicle.Theaimwastoassessthe clin-icaland radiographicdifferences inrelationtothe fixation methodsandtheirrespectivecomplications.
Patients
and
methods
Approvalfrom theresearchethicscommitteewasobtained before beginning the study (no. 0383.0.203.000-10). Each patientsignedafreeandinformedconsentstatement,soas tobeabletoparticipateinthestudy.
Fig.1–FixationusingTplateinanatomicalmodel,infrontalview.Notetheminimalprotuberanceoftheosteosynthesis material.
Allthepatientswereoperatedbytwoshouldersurgeons. Each ofthem onlyapplied one ofthe techniques: T plate orcoracoclavicularfixationwithanchorsinassociationwith Kirschnerwiresthroughtheacromioclavicularjoint.The cri-terion for allocating each patient was dependent on the availabilityofeachsurgeonintheappointmentsdiary.
NinepatientswereoperatedusingtheTplate technique andsix usingcoracoclavicularfixation withanchors.All of themwereoperatedinthedeckchairposition,undergeneral anesthesia inassociationwith interscalenebrachial plexus blockinorder tocontrolpostoperative pain.Routine intra-venousantibioticprophylaxiswasused(cefalotin,1g).
Thefracturesingroup1werefixedusingaTplate,which isgenerallyusedforvolarfixationoffracturesofthedistal radius. Thefracture was approached bymeans of a supe-riorlongitudinalincisionstartingfromtheacromioclavicular jointandextending3cmmediallyinrelationtothefracture site,withsubperiosteal dissection,anatomicalreductionof thefragmentsandstabilizationwithaTplateandscrews, fol-lowedbyclosureofthewound,compressivesteriledressings anduseofasling(Figs.1–3).
Thefractures ingroup2were fixedusing clavicular cer-clage,twoanchorsinthecoracoidprocessandtwoKirschner wires through the acromioclavicularjoint. The accesswas bymeans ofananteriorverticalincision startingfrom the fracturesiteandextendingasfarasthetipofthecoracoid
Fig.2–FixationusingTplateinanatomicalmodel,inview fromabove.
process.Two5mmmetalanchors(HexagonInd.Com. Apar-elhos Ortopédicos, Campinas, SP, Brazil) were fixed to the coracoid process. The suturing threads (which were non-absorbable,braided,sterileandmadeofpolyethylene) were passed through two holes that had been made earlier in themedialfragmentoftheclavicleandweretiedoffinthe anatomical position.In addition, twoKirschnerwires were passedthroughtheacromioclavicularjointinordertoincrease thestability;acompressivesteriledressingwasappliedand thelimbwasimmobilizedbymeansofasling(Figs.4–6).
The twogroups followedthe same postoperative proto-col.Clinicalandradiographicevaluationsweremadebythe sameshouldersurgeoninthefirst,secondandfourthweeks and monthlythereafteruntilthe sixth month.Exercisesto increasethepassiverangeofmotion(ROM)werestartedon thefirstdayaftertheoperation.Theslingwasuseduntilthe fourthweek.Ingroup2,theKirschnerwireswere removed inthesixthweek.AfterfullpassiveROMhadbeenattained, musclestrengtheningwasstarted.
Allthepatientswereassessedclinicallyand radiographi-callyateachoutpatientvisit.Avisualanalogscalewasused toevaluatetheintensityofpain(onascalefrom1to10).The radiographicevaluationincludedtheZancaandlateral axil-laryviews.TheConstant-Murleyscorewasappliedatthetime ofthefinalassessment,inthesixthmonth.
Fig.4–Fixationusinganchorinanatomicalmodel,in frontalview.
Fig.5–Fixationusinganchorinanatomicalmodel,in lateralview.
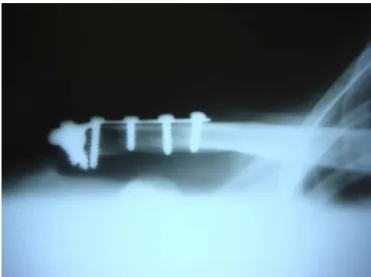
Fig.6–Finalradiographbythetechniqueusinganchors andKirschnerwires.
Table1–Physicalevaluationparametersof15patients whowereoperatedusingtheTplatetechnique(n=9)or
coracoclavicularfixation(n=6),between2008and2010.
Parameter Tplate Coracoclavicular fixation
Elevation 168.3 158
Externalrotation 61.7 58
Activitiesofdailyliving 9.6 8
Strength 5.9kg 5.7kg
Table2–Radiographic,functionalandcomplication assessmentson15patientswhowereoperateddueto fracturesofthedistalclavicle,between2008and2010.
Group1 Group2 p
Consolidation 100% 100% N.S.
Constantscore 83.4 76.4 0.029
Complications 0% 80% 0.04
TheSPSS13.0software(IBMforMac)wasusedforthe sta-tisticalanalysis. TheFishertestwas usedfordichotomous variablesandStudent’sttestwasusedforcontinuous vari-ables.Thestatisticalsignificancelevelwastakentobep<0.05.
Results
Themeanlengthoffollow-upwas26.7months(range:18–36). All ofthe fracturesbecameconsolidatedafterfourtoeight weeks. There were nodifferences between thetwo groups (p>0.05)inrelationtoage,gender,ROM,Craig’sclassification orpresenceofconsolidation(Table1).
Complicationsoccurred onlyinthe groups with coraco-clavicular fixation, with a rate of 80%. Themost frequent complicationsweresuperficialskininfectionandmigrationof theKirschnerwires.Allthecasesofinfectionwerecontrolled bymeansofremovalofthewires.Allthewiresmigratedtothe exterioroftheshoulder.ThemeanConstantscorewas83.4in group1and76.4ingroup2(p=0.029)(Table2).
Inrelationtopersonalsatisfaction,allthepatientsexcept foroneineachgroupweresatisfiedandsaidthattheywould undergotheprocedureagain,ifnecessary.
Discussion
Theclavicleperformsakeyroleincoordinatingthe biome-chanicsoftheshoulder.Itistheonlyboneconnectionbetween theaxialandappendicularskeletonsandsupportstheweight ofthe upperlimbs.These functionsemphasize the impor-tance ofachievinganatomical consolidationoffracturesof the clavicle,inorder topreservethe functionoftheupper limbs.1,7,10Thereisaconsensusintheliteraturethatdisplaced
fracturesofthedistalclavicleinyoungpatientsarean indica-tion forsurgicalfixation, giventhatconservativetreatment may lead to non-consolidation, pain, functional incapacity andpersonaldissatisfaction.11,14
propertiesofthedistalfragmentoftheclavicle(narrow,less dense and often comminutive) make fixation with screws difficult.Thesubcutaneouspositiongivesrisetoskin irrita-tioncausedbytheimplantsandfrequentlyrequiresimplant removal.Allofthishasledtodevelopmentofcostlyexclusive anatomicalplatesforfixationofthispatternoffractures.4,7,14
Therearemorethan30surgicaltechniquesavailablefor stabilizing these fractures.The majority present high con-solidationrates.Thefactorsthatdifferentiatethemaretheir costsandcomplicationrates(infections,skinirritation,nerve injuries,needforimplantremoval,periprosthetic fractures, etc.).3,4,12
Inthepresentstudy,consolidationwasachievedinallthe patientsand mostofthemwere personally satisfied, inde-pendentofthetechniqueused.Ingroup2(coracoclavicular fixationand Kirschnerwiresthroughthe acromioclavicular joint),higherratesofcomplications,infectionandmigration of Kirschner wires were observed. All the infections were superficialandwereproperlytreatedthroughremovalofthe Kirschnerwires.Althoughtherehavebeenreportsof migra-tionofthesewirestotheheart,eyesandother organs,the wiresthatmigratedinthepresentstudywereexpelledoutof theshoulder.15Anothercomplicationassociatedwithtyingoff
thethread(whichwasnotobservedinthepresentstudy) com-prisesfracturingduetoerosionoftheclavicleorcoracoid.15,16
Probablybecauseoftheshortfollow-upperiod,no degen-erative osteoarthrosis in the acromioclavicular joint was observed,despiteusingKirschnerwiresthatpassedthrough thisjoint.8,15,16Themethodsthatusefixationwithaplateto
stabilizefracturesoftheclaviclefrequentlyrequireremovalof theimplant,probablybecauseofthesubcutaneouspositionof theplate,especiallyincasesinwhichtheacromioclavicular jointispenetrated(hookplates).Thesecasesmayalsopresent periprostheticfractures.4
Inthepresentstudy,therewerenoperiprostheticfractures. Itwasalsonotnecessarytoremoveanyplatebecausetheone usedherehadathicknessofonly2mm,whereasthethickness ofDCPandhookplatesis3.5mm.17Specialcarewastakento
maketheincisionanteriorlytotheclavicle,soastofurnish agoodflapofsofttissueovertheplatesuchthatthewound wouldnotbeabovetheplate.4,7,12
Othercomplicationsofhookplates includeosteolysisof the acromionand erosionofthe rotator cuff.17 Oneofthe
advantagesofbothofthemethodsusedinthisstudywasthat therewasnorigidfixationabovethecoracoidprocessorthe acromion,forexampleusingBosworthscrews,whichmight havedelayed the rehabilitation or promoted periprosthetic fractures,becauseofthesmallbutfinitemovementbetween theclavicleandthescapula.4,5,11,18
Inthepresentstudy,whichhadhomogenoussamplesin bothgroups,betterclinical-functionalresultsandConstant scoreswereobservedintheplategroup.Althoughtherewere nodifferencesintheconsolidationrate,webelievethatthe grouptreatedwithplatesbegantoexpandthephysiological rangeofmotionearlierandalsoachievedthefullrangeearlier. The limitations of the present study were that it was retrospective andnon-randomized, withasmall sampleof patients.Ontheotherhand,theresultspresentedare con-clusiveandprovidesufficientevidenceforcomparingthetwo techniquesandtheirresults.
Conclusion
ThefracturefixationtechniqueusingTplateswassuperior tothetechniqueusinganchorswithKirschnerwiresbecause itshowedbetterfunctionalresultsandfewercomplications, whilepresentingthesameconsolidationrate.Thisstudy posi-tionstheuseofTplatesasanoptionforsurgicaltreatmentof displacedfracturesofthedistalclavicle.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.ChecchiaSL,DoneuxP,MiyazakiAN,CarvalhoLA,CanecaOA Jr.Fraturasdaclavículadistal:tratamentoeresultados.Rev BrasOrtop.1996;31(10):838–42.
2.ChecchiaSL,DoneuxPS,MiyazakiAN,FregonezeM,SilvaLA. Treatmentofdistalclaviclefracturesusinganarthroscopic technique.JShoulderElbowSurg.2008;17(3):395–8.
3.KhanLAK,BradnockTJ,ScottC,RobinsonCM.Fracturesof theclavicle.JBoneJointSurgAm.2009;91(2):447–60.
4.KleinSM,BadmanBL,KeatingCJ,DevinneyDS,FrankleMA, MighellMA.Resultsofsurgicaltreatmentforunstabledistal clavicularfractures.JShoulderElbowSurg.2010;19(7):1049–55.
5.ShinS-J,RohKJ,KimJO,SohnH-S.Treatmentofunstable distalclaviclefracturesusingtwosutureanchorsandsuture tensionbands.Injury.2009;40(12):1308–12.
6.AllmanFLJr.Fracturesandligamentousinjuriesofthe clavicleanditsarticulation.JBoneJointSurgAm. 1967;49(4):774–84.
7.FlinkkiläT,RistiniemiJ,HyvönenP,HämäläinenM.Surgical treatmentofunstablefracturesofthedistalclavicle:a comparativestudyofKirschnerwireandclavicularhook platefixation.ActaOrthopScand.2002;73(1):50–3.
8.NordqvistA,PeterssonC,Redlund-JohnellI.Thenatural courseoflateralclaviclefracture.15(11–21)yearfollow-upof 110cases.ActaOrthopScand.1993;64(1):87–91.
9.RobinsonCM.Fracturesoftheclavicleintheadult. Epidemiologyandclassification.JBoneJointSurgBr. 1998;80(3):476–84.
10.PostacchiniF,GuminaS,DeSantisP,AlboF.Epidemiologyof claviclefractures.JShoulderElbowSurg.2002;11(5): 452–6.
11.RobinsonCM,AkhtarMA,JenkinsPJ,SharpeT,RayA,OlabiB. Openreductionandendobuttonfixationofdisplaced fracturesofthelateralendoftheclavicleinyoungerpatients. JBoneJointSurgBr.2010;92(6):811–6.
12.KalamarasM,CutbushK,RobinsonM.Amethodforinternal fixationofunstabledistalclaviclefractures:early
observationsusinganewtechnique.JShoulderElbowSurg. 2008;17(1):60–2.
13.RobinsonCM,CairnsDA.Primarynonoperativetreatmentof displacedlateralfracturesoftheclavicle.JBoneJointSurg Am.2004;86(4):778–82.
14.YooJH,ChangJD,SeoYJ,ShinJH.Stablefixationofdistal claviclefracturewithcomminutedsuperiorcortexusing obliqueT-plateandcerclagewiring.Injury.2009;40(4):455–7.
16.PeterssonCJ.Resectionofthelateralendoftheclavicle.A3to 30-yearfollow-up.ActaOrthopScand.1983;54(6):
904–7.
17.LinHY,WongPK,HoWP,ChuangTY,LiaoYS,WongCC. Clavicularhookplatemayinducesubacromialshoulder
impingementandrotatorcufflesion–dynamicsonographic evaluation.JOrthopSurgRes.2014;9:6.