ASSOCI ATI ON BETW EEN OPERATI ONAL I NDEXES AND THE UTI LI ZATI ON RATE
OF A GENERAL SURGERY CENTER
Maria Helena Aoki Nepot e1 I lza Urbano Mont eiro2 Ellen Hardy2
Nep ot e MHA, Mon t eir o I U, Har d y E. Associat ion b et w een op er at ion al in d ex es an d t h e u t ilizat ion r at e of a general sur ger y cent er. Rev Lat ino- am Enfer m agem 2009 j ulho- agost o; 17( 4) : 529- 34.
This is a prospect ive st udy t hat focused on t he dynam ics of operat ing room s using operat ional indexes t hat m easure opt im izat ion, resist ance, overload and ut ilizat ion of t he surgical unit , and also ident ified t he fact ors m ost associat ed wit h t hese indexes. A t ot al of 1,908 surgeries were analyzed over a period of t wo m ont hs in 2007. The average rat es of ut ilizat ion, opt im izat ion and resist ance indexes were 80.41% , 65.35% and 34.65% r espect ively. The differ ence bet w een t he posit ive and negat ive over load index w as low ( 5.42% ) . Oper at ing room rescheduling and delays were the variables that contributed the m ost to the increase in these indexes. I n the linear regression statistical m odel, the utilization rate was found to be the first com m on variable selected in t he overload, resist ance and opt im izat ion indexes. I t is essent ial t o work on t hese operat ional indexes wit h a view t o obt ain sat isfact ory result s in t he m anagem ent of t he surgical cent er, wit h well- defined work processes and t eam w or k.
DESCRI PTORS: operat ing room nursing; surgical procedures, operat ive; m anagem ent indicat ors; perioperat ive nur sing
LA ASOCI ACI ÓN ENTRE LOS Í NDI CES OPERACI ONALES Y LA TASA DE OCUPACI ÓN
DE UN CENTRO QUI RÚRGI CO GENERAL
Se t r at a de u n est u dio pr ospect iv o qu e an alizó la din ám ica de las salas qu ir ú r gicas a t r av és de ín dices operacionales que m iden la opt im ización, resist encia, sobrecarga y ocupación del cent ro quirúrgico, y t am bién ident ificó los fact or es que m ás se asociar on a esos índices. Fuer on analizadas 1.908 cir ugías, dur ant e dos m eses en el año de .2007. La tasa de ocupación y los índices de optim ización y resistencia prom edios encontrados fueron 80,41, 65,35 y 34,65% , respectivam ente. La diferencia entre el índice de sobrecarga positivo y negativo fue baj o ( 5,42% ) . El cam bio de sala y el at raso, respect ivam ent e, fueron las variables que m ás cont ribuyeron par a la elev ación de esos índices. En la pr ueba est adíst ica de r egr esión linear se obser v ó que la t asa de ocu pación fu e la pr im er a v ar iable com ú n seleccion ada t an t o en los ín dices de sobr ecar ga, r esist en cia y optim ización. Es fundam ental la actuación sobre eses índices operacionales para obtener resultados satisfactorios en la adm inist ración del cent ro quirúrgico, con procesos bien definidos y t rabaj o en equipo.
DESCRI PTORES: enfer m er ía de quir ófano; pr ocedim ient os quir úr gicos oper at iv os; indicador es de gest ión; enfer m er ía per ioper at or ia
ASSOCI AÇÃO ENTRE OS Í NDI CES OPERACI ONAI S E A TAXA DE OCUPAÇÃO DE
UM CENTRO CI RÚRGI CO GERAL
Est udo prospect ivo que analisou a dinâm ica das salas cirúrgicas at ravés de índices operacionais que m edem a ot im ização, resist ência, sobrecarga e ocupação do cent ro cirúrgico, e t am bém ident ificou os fat ores que m ais se associar am a esses índices. For am analisadas 1908 cir ur gias, dur ant e dois m eses de 2007. A t ax a de ocu p ação e os ín d ices d e ot im ização e r esist ên cia m éd ios en con t r ad os f or am 8 0 , 4 1 , 6 5 , 3 5 e 3 4 , 6 5 % , r esp ect iv am en t e. A d if er en ça en t r e o ín d ice d e sob r ecar g a p osit iv o e n eg at iv o f oi b aix o ( 5 , 4 2 % ) . O rem anej am ento de sala e o atraso, respectivam ente, foram as variáveis que m ais contribuíram para a elevação desses índices. No t est e est at íst ico de regressão linear observou- se que a t axa de ocupação foi a prim eira variável com um selecionada t ant o nos índices de sobrecarga, resist ência com o ot im ização. É fundam ent al a at uação sobre esses índices operacionais para se obt er result ados sat isfat órios no gerenciam ent o do cent ro cirúrgico, com processos bem definidos e t rabalho em equipe.
DESCRI TOES: enferm agem de cent ro cirúrgico; procedim ent os cirúrgicos operat órios; indicadores de gest ão; enfer m agem per ioper at ór ia
Faculdade de Ciências Médicas da Univ er sidade Est adual de Cam pinas, Br azil: 1RN, Mast er ’s st udent , e- m ail: ccir ur gico@cm cnet .com .br ; 2Associat e Professor, e- m ail: dudinha@hot m ail.com , hardy@unicam p.br.
I NTRODUCTI ON
T
h e su r g e r y ce n t e r ( SC) i s a p a r t i cu l a r sect or in an y h ospit al, dist in gu ish ed f or it s r esu lt s,t h e c o m p l e x i t y o f i t s p r o c e d u r e s , i t s p o w e r t o
im plem en t def in it iv e cu r es, an d f or bein g t h e m ost
cost ly facilit y in t he hospit al( 1). The use of it s m axim um
su r g i ca l ca p a ci t y i s o n e o f i t s m a i n m e a su r e s o f
efficiency, as sur gical pat ient s r epr esent t he lar gest
r ev enue in a healt hcar e inst it ut ion( 2).
Nurses are increasingly m ore involved in t he
f i n a n ci a l d e ci si o n s a n d i n i n st i t u t i o n s’ b u d g e t a r y
p l a n n i n g a n d h a v e t o m a n a g e sca r ce r e so u r ce s
( hum an, m at erial and financial) . Nurses also have an
im por t an t r ole as agen t s of ch an ge t ow ar d posit iv e
r e su l t s, a n d a l so h a v e t o se e k b a l a n ce b e t w e e n
qualit y, quant it y and cost( 3).
Th e a d o p t i o n o f s y s t e m s t h a t m e a s u r e
perform ance is an im port ant t ool t hat helps m anagers
t o achieve such balance. I t helps t hem t o im plem ent
im provem ent st rat egies and present good result s. The
f ir m s’ in t er est in m easu r in g p er f or m an ce em er g ed
from proj ect s relat ed t o qualit y, efficiency, product ivit y
and cost s( 4).
One aut hor( 5) labeled t he gain in oper at ional
c a p a c i t y a s “ o p t i m i z a t i o n ” a n d t h e f a c t o r s t h a t
r epr esent loss of oper at ional capacit y in t he SC she
lab eled “ r esist an ce”. Th ese f act or s, su ch as d elay s
and cancellat ions, should be m inim ized because t hey
h a r m p r e o p e r a t i v e p r e p a r a t i o n , w h i ch r e su l t s i n
addit ional cost s t o t he hospit al, discom fort t o pat ient s
an d t h eir f am ily m em b er s an d also d issat isf act ion
w it h in t h e su r gical t eam( 6 ). I t is r ecom m en ded t h at
n u r se s a n d m a n a g e r s o f SC u n i t s r e d e si g n t h e i r
processes relat ed t o t hese fact ors ( preoperat ive visit ,
planning of t he sur gical schedule, hum an r esour ces,
m a t e r i a l s m a n a g e m e n t , a m o n g o t h e r s) a n d u se
con t r ol m et h ods t o st an dar dize or cor r ect pr oblem s
wit h a view t o est ablish m easures t o reduce t he causes
of su r g ical can cellat ion , est ab lish in g an d p u r su in g
goals t o be achiev ed( 2).
I t i s i m p o r t a n t t o m e n t i o n t h a t t h e
developm ent of a well- dim ensioned surgical m ap aim s
t o d i m i n i s h Op e r a t i n g Ro o m ( OR) i d l e n e s s a n d
p r o m o t e ad eq u at e ad m i n i st r at i o n o f t h ese r o o m s’
in t er v als. I n t u r n , it lessen s d elay s, im p r ov es t h e
est im at ion of av ailabilit y of in st r u m en t s, equ ipm en t
and m at erial necessary for surgeries and reduces risk
s i t u a t i o n s t o w h i c h p a t i e n t s a r e u n n e c e s s a r i l y
subj ect ed( 6). Under - ut ilizat ion should be analy zed, as
s h o u l d t h e d e m a n d f o r s u r g e r i e s a n d t h e
char act er ist ics of sur gical t eam s( 7).
I n pr act ice, su r gical t eam s in sist on h av in g
m or e t im e av ailab le f or su r g er y w h ile t h ey d o n ot
ev en u se t h e qu ot a allot t ed t o t h em . On t h e ot h er
h an d, t h e h ospit al h as t o m an age ov er loads in t h e
su r g e r y sch e d u l e , t a k i n g i n t o a cco u n t d e l a y s o f
cert ain t eam s in a given OR and procedures t hat delay
daily sur gical schedules( 8- 9).
Th e ef f icien cy of t h e ser v ices d eliv er ed b y
t he SC can be charact erized by m onit oring surgeries’
p u n ct u alit y, m in im u m t im e b et w een each su r g er y,
flex ibilit y in t he ut ilizat ion of av ailable ORs, capacit y
t o at t end t o em er gencies or addit ional sur ger ies, in
addit ion t o a low r at e of sur ger y cancellat ion and a
high rat e of ut ilizat ion of ORs( 9- 10).
Th e u se o f t h e SC ca n b e m o n i t o r e d b y
v ar iou s in dex es of oper at ion al per for m an ce su ch as
t h e op t im izat ion an d r esist an ce in d ex es m en t ion ed
a b o v e( 5 ) i n a d d i t i o n t o t h e o v er l o a d i n d ex , w h i ch
m easures t he difference bet w een t he act ual t im e t he
OR w a s i n u s e a n d t h e t i m e s c h e d u l e d b y t h e
su r geon( 5 ).
This st udy aim ed t o analyze t he dynam ics of
ORs t h r ou g h op er at ion al in d ex es t h at m easu r e t h e
opt im izat ion , r esist an ce, ov er load an d u t ilizat ion of
t he surgical unit . I t s specific obj ect ives were t o ident ify
t he fact ors m ost associat ed wit h t he st udied dependent
v a r i a b l e s ( o v e r l o a d , r e si st a n ce a n d o p t i m i za t i o n
index es) and t o ident ify t he associat ion bet w een t he
ut ilizat ion r at e and t hese index es.
METHOD
This pr ospect iv e st udy w as car r ied out in a
t ert iary and privat e hospit al in a cit y in t he int erior of
São Pau lo, Br azil. Th is h osp it al w or k s w it h q u alit y
pr ogr am s and or ganizat ional guidelines t hat est ablish
per for m ance goals and ar e m onit or ed by oper at ional
in d ex es, an aly zin g w or k p r ocesses an d m easu r in g
r e s u l t s t h a t g u i d e p r o j e c t s f o r c o n t i n u o u s
im p r ov em en t s.
Al l a n e st h e t i c- su r g i ca l p r o ce d u r e s ( 1 , 9 0 8
procedures) carried out from Monday t hrough Sat urday
bet ween Sept em ber and Oct ober 2007 were included.
We ch o se t o p er f o r m a g l o b al an al y si s o f t h e SC
because it s t en ORs ar e unifor m ly equipped, pr esent
no gr eat st r uct ur al or phy sical differ ences, and t heir
The operat ional indexes were calculat ed using
t he t im es regist ered on t he hospit al adm ission chart s,
t he pat ient s’ m edical file and on t he anest hesia chart s.
Dat a w er e r ecor ded on an Ex cel spr eadsheet .
- Ut i l i zat i o n r at e: Ef f e ct i v e u t i l i za t i o n o f t h e SC operat ional capacit y. Calculat ed by t he t ot al t im e ( in
m inut es) of ut ilizat ion of t he OR + t im e spent in it s
cleaning and preparat ion divided by t he t ot al num ber of hours during which t he SC was available ( 7 a.m .- 6
p.m . = 660 m inut es) m ult iplied by 100.
- Overload index: The ov er load index m easur es t he
excessive use ( posit ive overload index) or under- used
hours ( negat ive overload index) of t he OR operat ional
capacit y. The following variables were considered: t he
su r ger y ’s act u al du r at ion an d t h e t im e t h e su r geon
scheduled for t he pr ocedur e. I t is calculat ed by t he
difference bet ween t he act ual t im e used ( in m inut es)
an d t h e r eser v ed t im e ( in m in u t es) , div ided by t h e
r eser v ed t im e m ult iplied by 100.
- Opt im izat ion index: Gain in operat ional capacit y due
t o f act or s t h at f acilit at e pr ocedu r es in t h e OR t h at
cou n t er v ail sit u at ion s of r esist an ce. Var iab les w er e
d ef in ed as: p u n ct u alit y, h ow m u ch t im e su r g er ies
en d ed ah ead of sch ed u le, r at e of ex t r a su r g er ies,
r esch ed u lin g of su r g er ies; t im e sp en t t o clean an d
prepare t he OR ≤ 20 m inut es.
- Resistance index: Loss of operat ional capacit y caused
by obst acles t hat int erfere wit h t he capacit y of service p r o d u ct i o n . Va r i a b l e s w e r e d e f i n e d a s: d e l ay s i n
procedure st art t im e (≥ 16 m inut es) ; cancellat ions; OR
cleaning and preparat ion ≥ 21 m inut es.
Th e t u r n ov er t im e r ef er s t o t h e in t er v al of
t im e bet w een t h e en d of on e an est h et ic pr ocedu r e
and t he init iat ion of t he nex t w it hin t he sequence of p r o ced u r es i n t h e sam e OR, as r eg i st er ed o n t h e
anest hesia chart s for t hat specific room . This int erval
w as not included in t he list of independent v ar iables in t he Linear Regr ession t est because it w as alm ost
t he sam e for t he ent ir e sam ple.
St at ist ical An aly sis
The t echnique used was t he linear regression
m odel, which allowed select ing from a set of variables
all t hose t hat independent ly cont ribut ed t o t he global variat ion in t he out com e( 11). The significance level was
d ef in ed at p < 0 . 0 5 . For t h e an aly sis of d ep en d en t
v ar iables, t h e f ollow in g in depen den t v ar iables w er e included: ut ilizat ion rat e and t he variables com prising
t he oper at ional index es ( opt im izat ion, r esist ance and
ov er load ) .
Th e n a m e s o f p a t i e n t s , c o l l a b o r a t i n g
m em bers of t he surgical unit st aff and physicians were
not included in t he dat a collect ion for m s in or der t o
ensure t heir anonym it y. Each form was ident ified only
by t h e dat e of dat a collect ion an d t h e OR n u m ber.
Th e h ospit al’s ex ecu t iv e boar d of dir ect or s an d t h e
Resear ch Et hics Com m it t ee of t he School of Medical
S c i e n c e s a t t h e S t a t e U n i v e r s i t y o f Ca m p i n a s
( U N I CA M P) a p p r o v e d t h e s t u d y ’ s e t h i c a l a n d
m et h odological aspect s. No con sen t agr eem en t w as
r equ ir ed becau se t h e st u dy did n ot dir ect ly in v olv e
h u m an bein gs.
RESULTS
I n t h e st u d y sam p le, 9 0 % of t h e p at ien t s
at t ended t he scheduled sur ger y. Of t hese, 36% w er e
o u t p a t i e n t s a n d 6 4 % r e m a i n e d h o sp i t a l i ze d p o st
su r g er y. Th e d ist r ib u t ion of su r g er ies accor d in g t o
s p e c i a l t i e s w a s : Or t h o p e d i c s ( 2 1 . 4 % ) , Ge n e r a l
S u r g e r y ( 1 4 . 9 % ) , Gy n e c o l o g y a n d Ob s t e t r i c s
( 1 1 . 9 % ) , Ot o r h i n o l a r y n g o l o g y ( 1 1 . 2 % ) , Ur o l o g y
( 8.6% ) , Neurosurgery ( 6.4% ) , Head and Neck ( 5.8% ) ,
Pr oct ology ( 5. 4% ) , Plast ic ( 3. 6% ) , Vascular ( 3. 6% ) ,
Ped iat r ics 2 . 5 % ) , Th or ax ( 1 . 7 % ) , Car d iac su r g er y
( 1. 7% ) , ot her pr ocedur es ( 1. 2% ) .
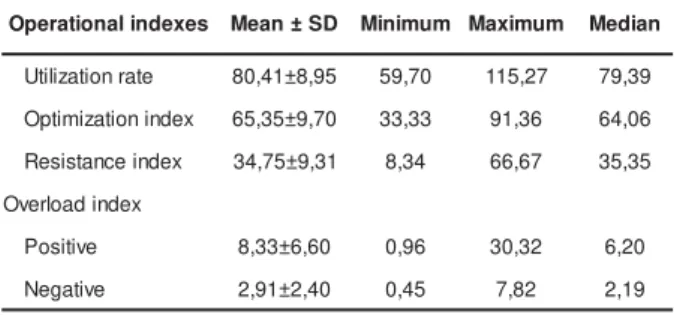
Th e u t ilizat ion r at e an d op t im izat ion in d ex
w e r e h i g h e r t h a n t h e r e s i s t a n c e i n d e x a n d
p r e s e n t e d a p o s i t i v e o v e r l o a d i n d e x t h a t w a s
r elat iv ely low ( Tab le 1 ) .
Table 1 - OR Operat ional indexes ( % )
The opt im izat ion index was m ainly det erm ined
by r escheduling of t he OR ( 41. 9% ) and by t ur nov er
t im e ≤ 20 m inut es ( 18. 1% ) . Delay w as t he v ar iable
t hat m ost cont ribut ed ( 65.10% ) t oward increasing t he
r esist ance index ( Table 2) .
s e x e d n i l a n o i t a r e p
O Mean±SD Minimum Maximum Median
e t a r n o it a z il it
U 80,41±8,95 59,70 115,27 79,39
x e d n i n o it a z i m it p
O 65,35±9,70 33,33 91,36 64,06
x e d n i e c n a t s i s e
R 34,75±9,31 8,34 66,67 35,35
x e d n i d a o l r e v O
e v it i s o
P 8,33±6,60 0,96 30,32 6,20
e v it a g e
Table 2 - St r uct ur e of t he opt im izat ion and r esist ance indexes ( % ) s e x e d n
I Variables %inrelationtotheindex %inrelationtothetotalnumberofsurgeries
) % 5 3 . 5 6 ( x e d n i n o it a z i m it p O g n il u d e h c s e R R
O 41.9 27.4
s e t u n i m 0 2 < e m it g n i n a e l
C 18.1 11.8
y t il a u t c n u
P 14 9,2
e m it f o d a e h a s e i r e g r u
S 7.1 4,6
s e i r e g r u s e v it c e l e r o f g n it t o l
S 3.1 2
s e r u d e c o r p y c n e g r u r o f g n it t o l
S 14.6 9.5
s e i r e g r u s y c n e g r e m e r o f g n it t o l
S 1.1 0.8
) % 5 6 . 4 3 ( x e d n i e c n a t s i s e R s y a l e
D 65.1 22.5
s n o it a ll e c n a
C 23.2 8.1
s e t u n i m 1 2 > e m it g n i n a e l
C 11.7 4
The overload index present ed a det erm inat ion
index of 0.0072 ( p= 0.0031) ( Table 3) . I t is im port ant
t o h i g h l i g h t t h a t t h i s co r r e l a t i o n w a s w e a k a n d
posit ive. The ut ilizat ion rat e and punct ualit y were t he
only variables associat ed wit h overload. The ut ilizat ion
r at e posit iv ely cor r elat ed w it h t he ov er load index ; it
pr esent ed an est im at ed par am et er of posit iv e v alue,
63.9% of t he part ial R2.
Table 3 - Var iables sign ifican t ly associat ed w it h t h e
ov er load in d ex .
t n e d n e p e d n I s e l b a i r a v d e t a m i t s E r e t e m a r a P d r a d n a t S r o r r
e P-value PartialR2
e t a r n o it a z il it
U 0.0460 0.0154 0.0031 0.0046
y t il a u t c n u
P 88.6655 39.9129 0.0264 0.0026
St at ist ical m odel: p= 0.003 R2= 0.0072
Th e r e s i s t a n c e i n d e x p r e s e n t e d a
d e t e r m i n a t i o n i n d e x o f 0 . 0 5 8 0 ( p < 0 . 0 0 0 1 ) . Th e
u t ilizat ion r at e w as t h e f ir st v ar iable select ed, w it h part ial R2 value of 0.0349, which represent ed 60.17%
of t he t ot al R2 value. Delay was t he variable t hat m ost
co n t r i b u t ed t o w ar d an i n cr eased r esi st an ce i n d ex ( Tab l e 4 ) . I t w as co m p o sed o f : 7 5 . 9 % r el at ed t o
su r g eon s’ d elay s, 8 . 6 % t o p at ien t s’ d elay s, 3 . 6 t o
hospit al’s, 3.3% t o sur gical unit and 8.6% t o ot her s f act or s.
Ca n c e l l a t i o n o f s u r g e r i e s w a s p o s i t i v e l y
associat ed w it h t he r esist ance index , w her eas 8. 1% of sur ger ies w er e canceled dur ing t he st udy per iod.
Cau ses f or can cellat ion in clu ded: pat ien t s’ per son al
r ea so n s ( 3 3 . 1 % ) ; su r g er y r esch ed u l i n g ( 1 6 . 5 % ) ; h e a l t h i n su r a n ce co m p a n i e s d i d n o t a p p r o v e t h e
pr ocedur e ( 1 2 . 0 % ) ; t he pr ocedur e w as canceled by
t he physician t he day befor e ( 11.4% ) ; pat ient s’ poor clinical condit ions ( 10. 1% ) ; no beds av ailable in t he
I nt ensive Care Unit ( I CU) ( 6.9% ) and ot hers ( 4.5% ) .
Table 4 - Var iables sign ifican t ly associat ed w it h t h e
r esist an ce in dex .
t n e d n e p e d n I s e l b a i r a v d e t a m i t s E r e t e m a r a P d r a d n a t S r o r r
e P-value R
2 e t a r n o it a z il it
U -0.1889 0.0232 <.0001 0.0349
s y a l e
D 3.0376 0.7390 <.0001 0.0130
s n o it a ll e c n a
C 2.9123 0.5086 <.0001 0.0084
St at ist ical m odel: p< 0.001 R2= 0.0563
Th e o p t i m i z a t i o n i n d e x p r e s e n t e d a
det erm inat ion index of 0.0521 ( p< 0.0001) . There was
a dir ect ly pr opor t ional cor r elat ion bet w een t his index
an d t h e u t ilizat ion r at e, w h er eas t h is v ar iab le w as
responsible for 59.96% of t he part ial R2. I n t his case,
t he delays in procedures st art ing t im e and cancellat ions
w e r e f o u n d t o b e i n v e r s e l y p r o p o r t i o n a l t o t h e
opt im izat ion index ( Table 5) .
Table 5 - Var iables sign ifican t ly associat ed w it h t h e
opt im izat ion index .
t n e d n e p e d n I s e l b a i r a V d e t a m i t s E r e t e m a r a P d r a d n a t S r o r r
e P-value PartialR2
e t a r n o i t a z il i t
U 0.1850 0.0243 <.0001 0.0312
s y a l e
D -3.2889 0.7716 <.0001 0.0118
n o i t a ll e c n a
C -2.9221 0.5310 <.0001 0.0091
St at ist ical m odel: p< 0.001 R2= 0.0521
DI SCUSSI ON
We found t he dynam ics of t he surgical cent er
sat isfact or y because t he over load index w as low , t he
op t im izat ion in d ex w as h ig h er t h an t h e r esist an ce
index and t he ut ilizat ion rat e reached t he m anagerial
goal ( 80 t o 85% ) . I n t he int ernat ional lit erat ure( 8), t he
u t ilizat ion r at e h as been ar ou n d 8 5 - 9 5 % . How ev er,
t h e ch ar act er ist ics of t h e su r g ical cen t er s in t h ese
an d ch ar ged per h ou r. I n w h ich case, r oom s bein g
over- ut ilized or under- ut ilized incur a financial loss( 8).
I n t h e Br azilian lit er at u r e, an av er age of 6 6 % w as
regist ered in a universit y hospit al( 12) and 76.21% was
t he av er age ut ilizat ion r at e found in a hospit al w it h
t h e sa m e ch a r a ct e r i st i cs o f t h e st u d i e d su r g i ca l
cent er( 13).
Result s reveal t hat over 40% of t he surgeries
were included in t he opt im izat ion index because t hey
h ad t h eir r oom s t r an sf er r ed . Wh en su r g er ies w er e
t r an sfer r ed or ar r an ged in t o em pt y r oom s, idlen ess
w a s a v o i d e d , p h y si ci a n s’ w a i t i n g t i m e f r o m o n e
su r g er y t o t h e n ex t d ecr eased an d t h e n u m b er of
sur ger ies incr eased, w hich consequent ly r educed t he
hospit al’s cost s( 6,10).
The low ov er load index did not significant ly
affect t he surgery schedule. For t hat , a good balance
bet w een t he under - ut ilizat ion and ov er - ut ilizat ion of
t he oper at ing r oom s w as achiev ed( 8, 9). For t hat , t he
professional responsible for planning t he OR schedule
has t o have a broad view of t he process, t hat is, t his
professional has t o reschedule or slot surgeries so t o
g ain t im e w h en p r oced u r es last m or e or less t im e
t han ex pect ed( 8,10).
Ut ilizat ion rat e and punct ualit y were t he only
v a r i a b l e s a sso ci a t e d w i t h o v e r l o a d , w h e r e a s t h e
ut ilizat ion rat e was direct ly proport ional t o t his index.
The associat ion bet ween punct ualit y and overload can
be ex plained by t he fact t hat punct ual sur ger ies had
a higher average durat ion in relat ion t o t he rem aining
st udied sur ger ies. Few er delay s w er e found t o occur
i n l o n g er p r o ced u r es ( su r g er i es t h a t ex ceed f o u r
hour s, t he st andar d est ablished in t his ser v ice) , and
even when surgeries were punct ual, over- ut ilizat ion( 8)
occu r r ed d u e t o t h e f act t h at t h e d u r at i on of t h e
surgery exceeded t he t im e scheduled by t he surgeon.
The resist ance index present ed an associat ion
inv er sely pr opor t ional t o t he ut ilizat ion r at e, t hat is,
t h e g r e a t e r t h e r e si st a n ce i n d e x , t h e l o w e r t h e
ut ilizat ion rat e. I n regard t o delays and cancellat ions,
t her e w as a dir ect and posit iv e associat ion.
Th e sa m e v a r i a b l e s w e r e se l e ct e d i n t h e
opt im izat ion index analy sis, t hough, w it h a differ ent
in t er p r et at ion : t h e h ig h er t h e u t ilizat ion r at e, t h e
great er was t he opt im izat ion index; and m any delays
an d can cellat ion s occu r r ed , ad v er sely af f ect in g t h e
o p t i m i z a t i o n i n d e x . Th i s r e s u l t s e e m s o b v i o u s ,
however, it is now verified in a st at ist ical t est .
I t i s k n o w n t h at d el ay s an d can cel l at i o n s
cause operat ing room idleness( 2,8- 10). I n t his st udy, t he
m ain cause of delay was t he surgeon. However, get t ing
phy sicians engaged in t he pr ocess is a difficult t ask
because, as client s of t he hospit al, t hey m ak e m any
dem ands and are not w illing t o invest in proj ect s for
im pr ov ing qualit y( 14).
The surgical unit nurse coordinat or has t o be
a t t e n t i v e t o t h e i n d i v i d u a l ch a r a ct e r i st i cs o f t h e
different professionals w orking in t he unit . The nurse
has t o know how each one act s and react s in t he face
of sit uat ions of conflict , t o bet t er lead his/ her t eam
an d gu ide t h e n u r sin g t eam ’s r elat ion sh ip w it h t h e
m e d i c a l t e a m( 1 5 ). Co n f l i c t i s i n h e r e n t i n h u m a n
r elat ionships, and should not be seen as som et hing
n eg at iv e. Th er e is a p er cep t ion t h at m an y con f lict
sit uat ions t hat occur in t he surgical unit are im port ant
an d n ecessar y becau se t h ese in dicat e ch an ges an d
g i v e o p p o r t u n i t i e s t o r e t h i n k si t u a t i o n s so a s t o
gener at e changes w it h a posit ive im pact on pat ient s’
car e( 15).
I n regard t o surgery cancellat ions, t he nurse
should also use st rat egies t o m inim ize t hem , analyzing
t h e cau ses g en er at i n g t h e p r o b l em( 2 ). A st u d y o n
surgical cancellat ions revealed t hat m ost cancellat ions
w er e p ot en t ially ev it ab le. Ad m in ist r at iv e p lan n in g ,
redesign of work processes, m easures t o educat e t he
st a f f a n d p r e o p e r a t i v e e v a l u a t i o n a r e st r a t e g i e s
r ecom m ended t o m inim ize t his k ind of ev ent( 2).
Alt hou gh t he cleaning and pr epar at ion t im e
was not an independent variable included in t he linear
r eg r ession m od el ( it w as alm ost a con st an t in t h e
st at ist ical t est ) , it should be not ed t hat som e surgical
t eam s at t ribut e delays t o t he t im e t aken t o clean t he
r o o m s, w h e r e a s i t m i g h t a l so b e r e l a t e d t o t h e
anest hesia and sur ger y t eam s and t o pat ient s( 16).
Acco r d i n g t o t h e l i t e r a t u r e , cl e a n i n g a n d
pr epar at ion begins aft er t he aux iliar y w ho t ak es t he
pat ient t o t he post anest het ic recovery room or t o t he
I CU( 1 ) r et u r n s, an d accor d in g t o som e au t h or s t h e
a v e r a g e t i m e s p e n t i n c l e a n i n g e x c e e d e d 3 0
m inut es( 1 , 5 , 1 6 ). How ev er, at t he st udied hospit al, t he
cleaning pr ocedur e begins as soon as t he anest het ic
procedure ends, regardless of whet her t he pat ient has
left t he OR or not . The hospit al’s goal is t o ensure t hat
t h e i n t e r v a l b e t w e e n t h e e n d o f o n e a n e st h e t i c
p r oced u r e an d t h e b eg in n in g of t h e n ex t d oes n ot
exceed 20 m inut es, w hich w as achieved in 88.3% of
t h e st u d ied su r g er ies. Th is is com p at ib le w it h t h e
t urnover t im e m ent ioned by one int ernat ional aut hor( 8),
in which one surgery was scheduled t o st art 20 m inut es
Th e t h r ee st u d ied in d ex es w er e associat ed
w it h t he ut ilizat ion r at e, since t his r at e w as t he fir st
v a r i a b l e sel ect ed i n t h e o v er l o a d , r esi st a n ce a n d
opt im izat ion in dex es. Th u s, pr o- act iv ely in t er v en in g
in t h ese in d ex es m ig h t r esu lt in b et t er op er at ion al
m anagem ent of t he surgical unit . I nt ervent ions require
c o n f r o n t i n g i n g r a i n e d a t t i t u d e s , e m p h a s i z i n g
t eam w o r k an d ef f ect i v e m et h o d s o f i n t er p er so n al
com m u n icat ion , an d en cou r agin g all t h ose in v olv ed
in t he operat ion of ORs t o get involved( 17).
FI NAL CONSI DERATI ONS
Nurses who occupy m anagem ent posit ions in
healt h inst it ut ions hav e t o hav e scient ific k now ledge
and t echnical expert ise, especially in a surgical cent er,
w h e r e t h e r e i s a c o n s i d e r a b l e d i v e r s i t y o f
professionals. Plans of act ion need t o be adequat e t o
client s’ profiles and m anagem ent has t o be based on
f act s an d p r oced u r es p r ev iou sly d ef in ed , ef f ect iv e
pract ices should be em phasized, and proact ive act ions
and ongoing t r aining encour aged.
Th e st u dy ’s r esu lt s can be t h e basis of t h e
d ev elop m en t of op er at ion al scor es t o ev alu at e t h e
ser v ices of t h e su r gical u n it becau se t h ey per m it a
crit ical analysis of a surgical unit ’s global perform ance.
Op er at ion al scor es also en ab le a cr it ical r ev iew of
t h e m a i n p r o ce sse s a n d r o u t i n e s i n v o l v e d i n t h e
surgical product ion, w hich can have great er or lesser
i m p a ct d e p e n d i n g o n h o w m a n y p r o f e ssi o n a l s o f
dif f er en t cat egor ies becom e in v olv ed.
REFERENCES
1. Possar i JF. Cent r o cir úr gico: planej am ent o, or ganização e gest ão. São Paulo ( SP) : I át r ia; 2004.
2 . Per r oca MG, Jer icó MC, Facundin SD. Sur ger y cancelling at a t each in g h osp it al: im p licat ion s f or cost m an ag em en t . Re v La t i n o - a m En f e r m a g e m 2 0 0 7 s e t e m b r o - o u t u b r o ; 1 5 ( 5 ) : 1 0 1 8 - 2 4 .
3- Francisco I MF, Cast ilho V. A enferm agem e o gerenciam ent o de cu st os. Rev Esc En f er m USP 2 0 0 2 ; 3 6 ( 3 ) : 2 4 0 - 4 . 4. Buosi T. Sist em a de m edição de desem penho: um a análise e pr oposição de um r ot eir o par a sist em at ização do pr ocesso d e d ef in ição d e r eq u isit os. [ d isser t ação] . São Car los ( SP) : Escola de En gen h ar ia de São Car los/ USP; 2 0 0 4 .
5 . Ga t t o M A F. A n á l i s e d a u t i l i z a ç ã o d a s s a l a s d e oper ações.[ t ese] . São Paulo ( SP) : Escola de Enfer m agem de Rib eir ão Pr et o/ USP; 1 9 9 5 .
6. St rofaro JR. Est udo da t axa de ocupação do cent ro cirúrgico at ravés da m odelagem e sim ulação de sist em as.[ dissert ação] . Cu r it ib a ( PR) : Pon t if ícia Un iv er sid ad e Cat ólica d o Par an á/ PUCPR; 2 0 0 5 .
7 . Macar io A, Dex t er F, Trau b RD. Hospit al pr ofit abilit y per hour of operat ing room t im e can vary am ong surgeons. Anest h An al g 2 0 0 1 ; 9 3 ( 1 ) : 6 6 9 - 7 5 .
8. Tyler DC, Pasquariello CA, Chen CH. Det erm ining opt im um operat ing room ut ilizat ion. Anest h Analg 2003; 96( 3) : 1114- 21. 9 . Dex t er F, Macar io A. Ch an g in g allocat ion s of op er at in g room t im e from a syst em based on a hist orical ut ilizat ion t o one w here t he aim is t o schedule as m any surgical cases as p ossib le. An est h An alg 2 0 0 2 ; 9 4 ( 2 ) : 1 2 7 2 - 9 .
1 0 . Kopr iv a CJ. Ef f icien cy in oper at ion r oom m an agem en t . Annual refresher course lect ures and clinical updat e program 1 9 9 4 ; 5 ( 2 ) : 3 0 - 1 .
1 1 . Fl e t ch e r RH, Fl e t ch e r SW. Ep i d e m i o l o g i a cl ín i ca . I n Flet ch er RH, Flet ch er SW. Pr og n óst ico. Por t o Aleg r e ( RS) : Ar t m ed; 2 0 0 6 . p. 1 3 1 - 5 3 .
12. Joaquim ED. Análise de um novo cent ro cirúrgico para o h osp it al u n iv er sit ár io Caj u r u : est u d o d e caso b asead o em s i m u l a ç ã o c o m p u t a c i o n a l . [ d i s s e r t a ç ã o ] . Cu r i t i b a ( PR) : Pon t if ícia Un iv er sid ad e Cat ólica d o Par an á/ PUCPR; 2 0 0 5 . 13. Nepot e MHA. Análise do desem penho das at iv idades no ce n t r o ci r ú r g i co a t r a v é s d e i n d i ca d o r e s q u a n t i t a t i v o s e q u a l i t a t i v o s. Re v Ad m Sa ú d e 2 0 0 3 o u t u b r o - d e z e m b r o ; 5 ( 2 1 ) : 2 1 - 3 0 .
1 4 . B e r w i c k D M , Go d f r e y A B , Ro e s s n e r J. D e z l i ç õ e s fundam ent ais para a m elhoria da qualidade. I n: Berw ick DM, Godfrey AB, Roessner J. Melhorando a qualidade dos serviços m édicos, h ospit alar es e da saú de. São Pau lo ( SP) : Mak r on Book s; 1 9 9 4 . p . 1 4 7 - 6 2 .
1 5 . St u m m EMF, Ma ça l a i RT, Ki r ch n e r RM. D i f i cu l d a d e s enfr ent adas por enfer m eir os em um cent r o cir úr gico. Tex t o Con t ex t o En f er m 2 0 0 6 j u lh o- set em b r o; 1 5 ( 3 ) : 4 6 4 - 7 1 . 16. Cologna MHYT, Dallora MEL, Hayashida M, Riul S, Sawada NO. Análise da ut ilização de sala de cir ur gia com apoio da i n f o r m á t i c a . Re v La t i n o - a m En f e r m a g e m 1 9 9 6 a b r i l ; 4 ( sp e ) : 7 1 - 8 2 .
1 7 . O v e r d y k FJ, H a r v e y S C, Fi s h m a n RL , S h i p p e y F. S u c c e s s f u l s t r a t e g i e s f o r i m p r o v i n g o p e r a t i n g r o o m e f f i ci e n cy a t a ca d e m i c i n st i t u t i o n s. An e st h An a l g 1 9 9 8 ; 8 6 ( 9 8 ) : 8 9 6 - 9 0 6 .