SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Case
Report
Posterior
dislocation
of
the
sternoclavicular
joint:
report
of
two
cases
夽
Pedro
José
Labronici
a,b,∗,
Fabrício
Cardoso
de
Souza
c,d,
Robinson
Esteves
Santos
Pires
e,
Fernando
Claudino
dos
Santos
Filho
b,
Vinicius
Schott
Gameiro
a,
Gustavo
José
Labronici
baUniversidadeFederalFluminense,Niterói,RJ,Brazil
bHospitalSantaTeresa,Petrópolis,RJ,Brazil
cFaculdadedeMedicinadeCampos,Campos,RJ,Brazil
dBeneficênciaPortuguesadeCampos,Campos,RJ,Brazil
eUniversidadeFederaldeMinasGerais,BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received31October2015 Accepted10November2015 Availableonline30August2016
Keywords:
Sternoclavicularjoint
Injuriesofthesternoclavicularjoint Closedreduction
Surgicaltreatment
a
b
s
t
r
a
c
t
Theauthorsreportthecasesoftwoyoungpatientswhohadsufferedasportingaccident withposteriortraumaticdislocationofsternoclavicularjoint.Inoneofthepatientsclosed reductionwasaccomplishedbykeepingthelimbinasling.Thesecondpatient,after reduc-tionwasdone,presentedrecurrenceofthedislocation,thusrequiringsurgicaltreatment.It isimportanttoobservetherelevanceofcomputedtomographytohelpdiagnosing,aswellas monitoringthereductionprocedure.Theobjectiveofthisstudywastodemonstratetwo dif-ferenttypesoftreatmentinarareinjurysuchastheposteriordislocationofsternoclavicular joint.
©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Luxac¸ão
posterior
da
articulac¸ão
esternoclavicular:
relato
de
dois
casos
Palavras-chave:
Articulac¸ãoesternoclavicular Lesõesdaarticulac¸ão esternoclavicular Reduc¸ãoincruenta Tratamentocirúrgico
r
e
s
u
m
o
Relato de casode doisjovensqueseacidentaramno esportee apresentaramluxac¸ão traumáticaposteriordaarticulac¸ãoesternoclavicular.Emumpacientefoifeitaareduc¸ão incruenta e manutenc¸ão comtipoia. Osegundo paciente, após a reduc¸ão, apresentou recidiva da luxac¸ão,foinecessário otratamento cirúrgico.Valesalientar a importância datomografiacomputadorizadanoauxíliododiagnóstico,assimcomoparamonitorara
夽
StudyconductedatHospitalSantaTeresa,Petrópolis,RJ,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](P.J.Labronici). http://dx.doi.org/10.1016/j.rboe.2016.08.019
Traumaticposteriordislocationofthesternoclavicularjoint isarareinjurywithless than1%incidenceamongall dis-locations, but which is potentially serious.1 This injury is
mostfrequentlyobservedinyoungadultsafterhigh-energy traumaandcanbedifficulttodiagnose, bothclinicallyand radiographically.2 Although rare, posterior sternoclavicular
dislocationisassociatedwithseveralcomplicationsduetothe proximitytomediastinalstructures. These injuriesinclude respiratorysystemandbrachialplexusimpairment,vascular injury,pneumothorax,anddysphagia,andmayevenleadto death.3–5
Accordingtotheliterature,traumaticposteriordislocation ofthesternoclavicularjointisoftenassociatedwithdelayed diagnosisandmayinitiallybeclinicallyinsignificant.Itcan be treated with joint stabilization through closed or open reduction.3–7
Thisreportaimedtopresenttwocasesoftraumatic poste-riordislocationofthesternoclavicularjointthatweretreated differentways,andtodrawattentiontothevalueofCTscan inconfirmingthediagnosisandmonitoringofthereduction.
Case
report
Case1
Eighteen-year-oldmalepatientreported alever-typesoccer fall,havingfallenonhisleftshoulder,hisnon-dominantside. Hearrivedatthehospitalemergencyroom45minafterthe accident,withpainintheleft shouldergirdle,especiallyin thesternoclavicularjoint,witharmmovementdifficulty.He deniedparesthesiaortinglinginthelimb,difficultybreathing, orpaininthecervicalregion.
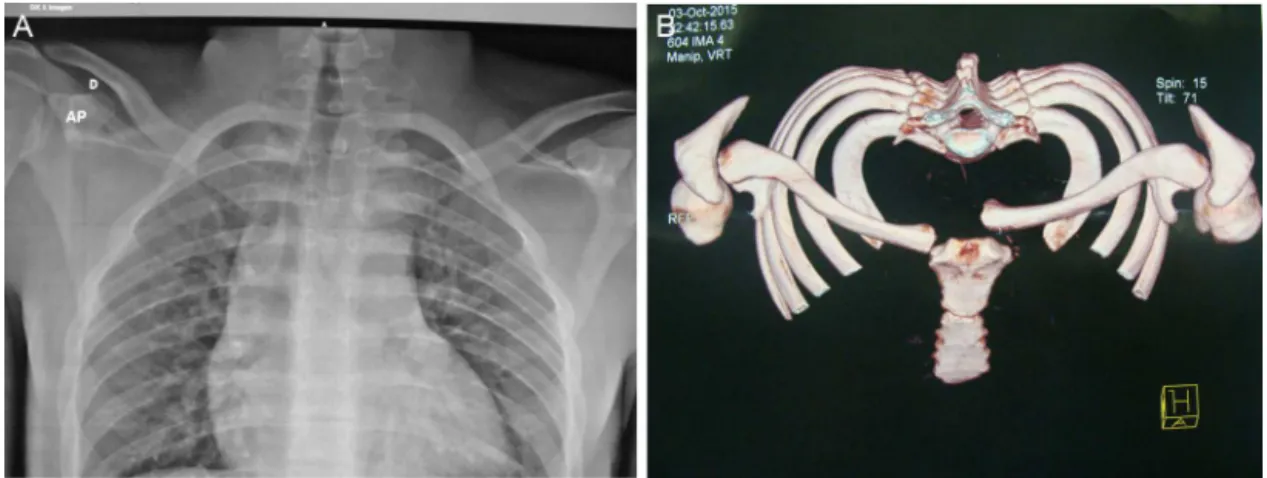
Upon physicalexamination, the skin was normal, with a slight asymmetrical swelling on the left side. Function andstrengthwere limitedbypain.Thepatienthadpainat palpationon the left sternoclavicularjoint.Neuromuscular examinationoftheupperleftlimbwasnormal.Radiographic examinationshowedasymmetryoftheleftsternoclavicular jointandthepatientwastakenimmediatelytotheCTscan (Fig.1AandB).
Thepatientwasexaminedtwodaysaftertheinjurybythe traumateam,whodecidedtotreatthedislocationwithclosed reduction.Hewastaken totheoperatingroom and under-went generalanesthesia.He waspositioned supinewith a cushioninthedorsalregion,betweentheshoulders,andthe reductionmanouverwasmadewiththeaidofatowelclamp insertedpercutaneously.Atthetimeofreduction,a“clunk” wasfelt;atboththeclinicalexaminationandfluoroscopy,the
CTscan.Theresultshowedthatthereductionhadbeenlost, andthetreatmentwasrescheduledwithopenreductionand fixation(Fig.2AandB).
Surgicalprocedure
Thepatientwaspositionedsupinewithacushionbetween his shoulders. Under generalanesthesia and following the administration of 2g of EV cephaloridine, an incision of approximately8cmfromthemanubriumtothemiddlethird oftheclaviclewasmade.Throughcarefuldissection,itwas noted that the sternoclavicular ligaments of the anterior regionwereintact,butafterincisingtheligament,damageto theposteriorligamentsofthejointandextensiveperiosteal avulsionofthemiddlethirdoftheclavicle,whichwas infer-iorly deviated, wereobserved. Themeniscus wasidentified andrepaired.Subsequently,twoholesweremadewitha2mm drillbitinthemanubrium,throughwhichanEthibondExel M46® No.5wire waspassed.Two holes were made inthe clavicle,usingadrillbitofthesamethickness,andthewire waspassed.Thedislocationwasreducedandfixedwiththe wireinacerclagemanner.Anadditionalwirewasusedinthe upperregionbetweenthemanubriumandclavicletosecure thereduction.Theshoulderwastestedandjointstabilitywas observed.Thewoundwasclosedwithsutureoftheanterior sternoclavicularligamentandsubsequenttissues.Thepatient wasimmobilizedwithasling(Fig.3AandB)
Case2
Thirtysixyearoldmalepatient,aged36years,sufferedadirect traumaonhisleftclavicle(nondominantside)duringa soc-cergame(playingasgoalkeeper,whenhegotdowntomake a defense,hetooka knee strikedirectly ontohisclavicle). On emergency care,hepresentedsevere pain inthe clavi-cleregion,butwithoutmajordeformitiesvisibleonphysical examination.Hedidnotshowarmmovementdifficulty,limb numbnessortingling,difficultybreathing,orpaininthe cer-vicalregion.Functionandstrengthwerelimitedbypain.The patienthadpainatpalpationontheleftsternoclavicularjoint andwasimmediatelytakentotheCTscan(Fig.4AandB).
Fig.1–(A)Radiographyshowingthesternoclaviculardislocationtotheleft;(B)computedtomography3-Dreconstruction
demonstratingthedislocationtotheleft.
Fig.2–(A)Radiographyafterclosedreduction;(B)computedtomographyshowingrecurrentdislocation.
showedthereduceddislocationandthepatientwastreated withaslingandradiographicfollow-up.
Discussion
Traumaticposteriordislocationofthesternoclavicularjoint is a rare injury with less than 1% incidence among all
dislocations, but which is potentially serious.1 The
litera-turehasreportedthat injurieswithposteriordisplacement of the medialclaviclemay be associatedtotrauma to the trachea,esophagus,andgreatvessels.However,duetothe rar-ityofsuchinjuries,long-termstudieswithlargenumbersof patientsarenotavailable.1,3–11
Thesternoclavicularjointisstabilizedanteriorlyand pos-teriorly by the joint capsule and by the sternoclavicular,
Fig.3–(A)Imageofthesternoclavicularjointafteropenreductionwithcerclage;(B)computedtomographyshowingtheleft
Fig.4–(A)Radiographyshowingthesternoclaviculardislocationtotheleft;(B)computedtomography3-Dreconstruction
demonstratingthedislocationtotheleft.
interclavicular,andcostoclavicularligaments.Theposterior ligamentsaresignificantlymoreresistant,requiring50%more force to produce a posterior dislocation than an anterior dislocation.12 Mobility and laxity of sternoclavicular joint
decreasewithage,thereforethisinjuryismorecommonin young adults. The clavicle is the first long bone to ossify, whilethemedialphysisisthelasttoclose.Themedial clav-icleis notossifiedbefore 18–20years ofageand it merges withthediaphysisaroundthe23rdto25thyearofage.13This
isimportantbecausetraumainyoungpeople,especiallyin athletes, maynot belimitedtothe classicsternoclavicular posteriordislocation,butrathermaymaskanepiphyseal devi-atedfracture-avulsion.
Thediagnosis throughconventional X-raysforposterior dislocationofthesternoclavicularjointmaybedifficultdue tothesuperpositionoftheradiographicanatomy,which hin-dersanidealimage.Specialviewshavebeenrecommended bysomeauthors,buttheyarelimited.14Intheanteroposterior
(AP)view,dislocationofthesternoclavicularjointissuspected whenthereisadifferenceinrelationtothecraniocaudal posi-tiongreaterthan50%ofthemedialclavicularepiphysis.7
NumerousarticleshavereportedtheadvantagesoftheCT scantoassess the medialclavicleand thesternoclavicular joint.Theimages providedbyCT scanhelptoobserve not onlythebonedetails,butalsothesofttissuestructuresaround theinjury.6,13,15Especiallyinposteriordislocationofthe
ster-noclavicularjoint,whichisamoreserious injuryand may compromise the structuresof the thoracicregion, anterior andposteriormediastinum(esophagusandtrachea),nerves, andgreatvessels(brachiocephalicvein,superiorvenacava, andaorta),theCTscanhasgreatvalueinthediagnosisand prognosisofthe injury, despitethe absorbed radiation.14,16
Therefore,onsuspicionofposteriordislocationofthe stern-oclavicularjoint,analysiswithCTscanand3Dreconstruction are recommended, as it was particularly importantin the presentcasestoobservethe medialinjury,bothtoconfirm thediagnosisandmonitorthereduction.Inpatientsyounger than25years,thepossibilitythattheinjuryisanepiphyseal fracture-detachmentratherthanonlydislocationofthejoint shouldbeobservedontheCTscan.6
Aspreviouslyreported,duetotherarityofinjuries, long-termstudieswithlargenumbersofpatientsarenotavailable. Thismakesitdifficulttoindicatethebesttreatmentfor poste-riordislocationsoftheclavicle.Thereisnoevidencethatcan guidetreatmentchoice.However,theauthorsbelievethatif thepatientdoesnotshowsignsofmediastinalcompression, closedreductionshouldbeattempted,supervisedbya tho-racicorvascularsurgeontoavoidunpleasantsurprisesduring the reduction.Vigorous limbtractionshouldbeavoided,as nervous structurescan bestretchedor damaged.2 Theuse
of areductionclamp may be agood technique, as recom-mended byKayias et al.17 and Wettsteinet al.18 Moreover,
inpatientswithsignsofmediastinalcompression,meniscus injury,orinstabilitywithrecurrentdislocation,surgical treat-ment shouldbe indicated.19 Numeroussurgicaltechniques
havebeenproposed.19–25Inordertoavoidfunctional
limita-tion,treatmentshouldsparethearticularsurface,stabilizethe capsularandligamentousstructuresand,inthecaseofyoung patients,reducetheepiphysealfracture.TheuseofKirschner wirestotemporarilyaidreductionshouldbeavoided,asitcan leadtocomplicationssuchasbreakageofthematerialorwire migration.13,26,27
Inthecasewheresurgerywasneeded,an8-shaped cer-clagetechniquewasused,withEthibondExelM46®No.5wire andasuperiorreinforcementonthejoint,withthesamewire, topreventlossofreduction.Thepatientwaskeptinasling forsixtoeightweeksandwasrecommendedtoavoidraising thearm≥60◦.After12weeks,hewasinstructedtogradually increasetheuseofthelimbtoperformactivitiesofdailyliving.
Conclusion
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. JougonJB,LeprontDJ,DromerCE.Posteriordislocationofthe sternoclavicularjointleadingtomediastinalcompression. AnnThoracSurg.1996;61(2):711–3.
2. BuckerfieldCT,CastleME.Acutetraumaticretrosternal dislocationoftheclavicle.JBoneJointSurgAm. 1984;66(3):379–85.
3. OnoK,InagawaH,KiyotaK,TeradaT,SuzukiS,MaekawaK. Posteriordislocationofthesternoclavicularjointwith obstructionoftheinnominatevein:casereport.JTrauma. 1998;44(2):381–3.
4. GrohGI,WirthMA.Managementoftraumatic sternoclavicularjointinjuries.JAmAcadOrthopSurg. 2011;19(1):1–7.
5. HoekzemaN,TorchiaM,AdkinsM,CassiviSD.Posterior sternoclavicularjointdislocation.CanJSurg.
2008;51(1):E19–20.
6. LaffosseJM,EspiéA,BonnevialleN,MansatP,TricoireJL, BonnevialleP,etal.Posteriordislocationofthe
sternoclavicularjointandepiphysealdisruptionofthemedial claviclewithposteriordisplacementinsportsparticipants.J BoneJointSurgBr.2010;92(1):103–9.
7. KhorashadiL,BurnsEM,HeastonDR.Posteriordislocationof thesternoclavicularjoint.RadiolCaseRep.2011;6(3):439–44. 8. MirzaAH,AlamK,AliA.Posteriorsternoclavicular
dislocationinarugbyplayerasacauseofsilentvascular compromise:acasereport.BrJSportsMed.2005;39(5):e28. 9. NakayamaE,TanakaT,NoguchiT,YasudaJ,TeradaY.
Trachealstenosiscausedbyretrosternaldislocationofthe rightclavicle.AnnThoracSurg.2007;83(2):685–7.
10.WormanLW,LeagusC.Intrathoracicinjuryfollowing retrosternaldislocationoftheclavicle.JTrauma. 1967;7(3):416–23.
11.WasylenkoMJ,BusseEF.Posteriordislocationoftheclavicle causingfataltracheoesophagealfistula.CanJSurg. 1981;24(6):626–7.
12.RockwoodCAJr.Injuriestothesternoclavicularjoint.In: RockwoodCAJr,GreenDP,BucholzRW,HeckmanJD,editors. Fracturesinadults.3rded.Philadelphia:Lippincott;1991.p. 1253–307.
13.WirthMA,RockwoodCAJr.Acuteandchronictraumatic injuriesofthesternoclavicularjoint.JAmAcadOrthopSurg. 1996;4(5):268–78.
14.McCullochP,HenleyBM,LinnauKF.Radiographiccluesfor high-energytrauma:threecasesofsternoclavicular dislocation.AmJRoentgenol.2001;176(6):1534.
15.JaggardMK,GupteCM,GulatiV,ReillyP.Acomprehensive reviewoftraumaanddisruptiontothesternoclavicularjoint withtheproposalofanewclassificationsystem.JTrauma. 2009;66(2):576–84.
16.KaewlaiR,AveryLL,AsraniAV,NovellineRA.MultidetectorCT ofbluntthoracictrauma.Radiographics.2008;28(6):1555–70. 17.KayiasEH,DrososGI,AnagnostopoulouGA.Atraumatic
retrosternaldislocationoftheclavicle.ActaOrthopBelg. 2004;70(3):273–5.
18.WettsteinM,BorensO,GarofaloR,KombotC,ChevalleyF, MouhsineE.Anteriorsubluxationafterreductionofa posteriortraumaticsterno-claviculardislocation:acase reportandareviewoftheliterature.KneeSurgSports TraumatolArthrosc.2004;12(5):453–6.
19.BenitezCL,MintzDN,PotterHG.MRimagingofthe sternoclavicularjointfollowingtrauma.ClinImaging. 2004;28(1):59–63.
20.RobinsonCM,JenkinsPJ,MarkhamPE,BeggsI.Disordersof thesternoclavicularjoint.JBoneJointSurgBr.
2008;90(6):685–96.
21.BoothCM,RoperBA.Chronicdislocationofthe
sternoclavicularjoint:anoperativerepair.ClinOrthopRelat Res.1979;(140):17–20.
22.BrinkerMR,BartzRL,ReardonPR,ReardonMJ.Amethodfor openreductionandinternalfixationoftheunstableposterior sternoclavicularjointdislocation.JOrthopTrauma.
1997;11(5):378–81.
23.ArmstrongAL,DiasJJ.Reconstructionforinstabilityofthe sternoclavicularjointusingthetendonofthe
sternocleidomastoidmuscle.JBoneJointSurgBr. 2008;90(5):610–3.
24.FranckWM,SiassiRM,HennigFF.Treatmentofposterior epiphysealdisruptionofthemedialclaviclewithamodified Balserplate.JTrauma.2003;55(5):966–8.
25.PimentaR,AlegreteN,VidinhaV,LimaS,PintoI. Fratura-descolamentoepifisáriomedialdaarticulac¸ão esternoclavicularcomdesvioposteriorematletadejudô– Equivalentedeluxac¸ãoesternoclavicularposterior.RevBras Ortop.2013;48(2):196–9.
26.Smolle-JuettnerFM,HoferPH,PinterH,FriehsG,Szyskowitz R.Intracardiacmalpositioningofasternoclavicularfixation wire.JOrthopTrauma.1992;6(1):102–5.
27.PerdreauA,BingenB,GossingL,LejeuneE,BeugniesA. Posteriorsternoclavicularepiphysealfracture-dislocation: casereportandreviewofliterature.InjuryExtra.