1 M. Sc. I n Nursing, Faculty, School of Health Sciences – UNI VAS, Stom al therapist, e- m ail: [email protected] .br, Brazil; 2 PhD, Faculty, University of São Paulo School of Nursing, Brazil
Disponible en castellano/ Disponível em língua portuguesa SciELO Brasil w w w .scielo.br/ rlae
RI SK FACTORS FOR PRESSURE ULCER DEVELOPMENT I N I NSTI TUTI ONALI ZED ELDERLY
Diba Maria Sebba Tost a de Souza1 Ver a Lúcia Conceição de Gouv eia Sant os2
Souza DMST, Sant os VLCG. Risk fact ors for pressure ulcer developm ent in inst it ut ionalized elderly. Rev Lat ino-am Enferm agem 2007 set em bro- out ubro; 15( 5) : 958- 64.
This st udy aim ed t o analyze t he risk fact ors for t he developm ent of Pressure Ulcers ( PU) in old people living in Long St aying I nst it ut ions. I t is a prospect ive and cohort st udy carried out in four I nst it ut ions. A t ot al of 94 old people com posed t he sam ple and w er e assessed dur ing t hr ee consecut iv e m ont hs. The t ot al scor es of t h e Br aden Scale w er e dif f er en t bet w een t h e gr ou ps w it h an d w it h ou t PU, at t h e f ir st ( p= 0 . 0 3 0 ) an d last assessm ent s ( p= 0 , 0 0 1 ) ; hum idit y , nut r it ion and fr ict ion/ shear ing w er e significant ly differ ent bet w een t hose w it h and w it hout PU, and w er e alw ays w or st am ong t he fir st . Fem ale gender and pr evious PU w er e confir m ed as pr edict iv e for t he dev elopm ent of PU ( r2= 0,311) .
DESCRI PTORS: r isk fact or s; pr essur e ulcer ; aged; hom es for t he aged
FACTORES DE RI ESGO PARA EL DESARROLLO DE ÚLCERAS POR PRESI ÓN EN ANCI ANOS
ATENDI DOS EN ASI LO
La finalidad del est udio fue analizar los fact or es de r iesgo par a el desar r ollo de Ulcer as por Pr esión ( UP) en an cian os q u e v iv en en asilos. Es u n est u d io d e coh or t e p r osp ect iv o y f u e d esar r ollad o en cu at r o in st it u cion es. Nov en t a cu at r o an cian os com pu sier on la m u est r a y fu er on ev alu ados con secu t iv am en t e h ast a t res m eses. Las punt uaciones t ot ales de la Escala de Braden fueron diferent es ent re los grupos con y sin UP, en la prim era ( p= 0.030) y la últ im a evaluación ( P = 0.001) ; hum edad, nut rición y fricción fueron est adíst icam ent e difer ent e ent r e los ancianos con y sin UP, peor ent r e aquellos con UP. El sex o fem enino y UP pr ev io fuer on confir m ados com o pr edict iv os par a el desar r ollo de PU ( r 2= 0, 311) .
DESCRI PTORES: fact or es de r iesgo; úlcer a por pr esión; anciano; hogar es par a ancianos
FATORES DE RI SCO PARA O DESENVOLVI MENTO DE ÚLCERAS POR PRESSÃO EM I DOSOS
I NSTI TUCI ONALI ZADOS
Est e est udo obj et ivou analisar os fat ores de risco para o desenvolvim ent o de úlceras por pressão ( UP) em id osos in st it u cion alizad os. Est u d o d e coor t e p r osp ect iv o f oi r ealizad o em q u at r o in st it u ições d e lon g a per m an ên cia par a idosos. Nov en t a e qu at r o idosos f or am av aliados du r an t e at é 3 m eses con secu t iv os. Os escor es t ot ais da Escala de Br aden difer ir am ent r e os gr upos com e sem UP, na pr im eir a ( p= 0,030) e últ im a av aliações ( p= 0,001) , um idade, nut r ição e fr icção e cisalham ent o for am significat iv am ent e difer ent es ent r e os idosos com e sem UP, sem pr e pior es ent r e os pr im eir os. Sex o fem inino e úlcer a pr évia for am pr edit ivos par a a for m ação das UP ( r2= 0,311) .
I NTRODUCTI ON
C
ert ain risk fact ors have been confirm ed as predictive for pressure ulcer ( PU) developm ent, which im plies physical, em ot ional, and social overloads for patients and their fam ilies. This consequently reduces t he qualit y of life and increases healt h service cost s, d u e t o lon g er h osp it alizat ion p er iod s an d h ig h er m orbidit y and m ort alit y rat es.I n relation to the PU concept, two definitions h av e b een ad op t ed : t h e Nat ion al Pr essu r e Ulcer Advisory Panel ( NPUAP)( 1) stated that “ PU are caused
by pr olonged pr essur e and t y pically occur on bony pr om in en ces in in div idu als r est r ain ed t o a bed or w h e e l ch a i r ” ; a n d t h e Eu r o p e a n Pr e ssu r e Ul ce r Advisory Panel ( EPUAP)( 2) says that “ PU is an area of
cellu lar d eat h on t h e sk in an d u n d er ly in g t issu es cau sed b y p r essu r e, sh ear i n g , f r i ct i o n an d o r a co m b i n a t i o n o f t h e se f a ct o r s”. Th e se co n ce p t s e st a b l i sh n o t o n l y t h e n o m e n cl a t u r e cu r r e n t l y em ploy ed for t his t y pe of lesion, but also it s m ain et iology.
I n 1987, North Am erican authors( 3) developed
a co n ce p t u a l ch a r t a b o u t e t i o p a t h o g e n y f o r PU d e v e l o p m e n t , f r o m t w o cr i t i ca l e t i o l o g i ca l det er m inant s: pr essur e int ensit y and dur at ion; and tissue tolerance to support that pressure. I n addition, ot her ext rinsic and int rinsic fact ors cont ribut e t o PU developm ent . While ext rinsic fact ors include frict ion and shearing associated with m oisture, intrinsic factors consist of loss of sensitivity and reduction in m uscular st r en g t h or m ob ilit y, in con t in en ce, h y p er t h er m ia, anem ia, pr ot ein m alnour ishm ent , sm ok ing and old ag e.
Old er p eop le’s sk in g oes t h r ou g h v ar iou s ch a n g es d u e t o t h e i n t r i n si c a g i n g p r o cess a n d environm ent al fact ors, especially ult raviolet radiat ion ( actinosenescence) . Aged skin takes part in regressive changes in various organic sect ors, and is classified in t w o t y pes: int r insic - chr onological ( genet ic) or pathological ( genetic or not) - and extrinsic. Therefore, senescence is a biological consequence of lifet im e. Pseudo- senescence, on t he ot her hand, result s from the aggression of environm ental factors on the hum an skin t hroughout one’s exist ence( 4).
El d e r l y sk i n a sse ssm e n t i s b a se d o n p h y si o l o g i ca l cr i t er i a l i k e h y d r a t i o n , ch a n g es i n se b a ce o u s se cr e t i o n a n d sw e a t g l a n d s a n d perm eability; and biological criteria, based on changes t o t h e con n ect iv e t issu e an d t h e fou r in t er cellu lar
m atrix m olecules: collagen, elastin, proteoglycans and glycoprotein, as well as the fibroblasts that synthesize t hem( 4).
Ag in g f r ag ilen ess associat ed w it h m or b id conditions, such as changes to neurological and m ental states, nutritional conditions, m obility, anal and urinary act iv it y and cont inence, char act er izes a populat ion pr edisposed t o PU dev elopm ent , r eoccur r ence and com plicat ions. This is an overall view t hat has led t o t he growing need for t heir inst it ut ionalizat ion( 5).
Long- St ay I nst it ut ions for t he Elderly ( LSI E) are facilit ies designed for int egral inst it ut ional care. The t arget populat ion includes people older t han 60, dependent or not, who are not able to stay with their fam ily or at hom e. These inst it ut ions receive various nam es, including: shelt er, hom e, nursing hom e and geriatric clinic. To m eet this age group’s needs, these f a ci l i t i e s p r o v i d e , f o r i n st a n ce , so ci a l , m e d i ca l , psychological, nursing, physical t herapy, occupat ional t herapy and dent al services( 6).
These locat ions should provide a resident ial environm ent , keeping t he charact erist ics of a hom e. They should not be m arked by isolat ion, away from ur ban life, or be a space t hat sim plifies it s user s’ lives( 6).
The m otivation to develop this study was based on r ecognizing age as a fundam ent al aspect of PU et iopat hogeny and t he lack of Brazilian st udies about PU risk fact ors in inst it ut ionalized elderly. Hence, t he study obj ectives were: to analyze PU risk factors and verify t he st at ist ical associat ions bet ween risk fact ors and PU occurrences in elderly people living in LSI E.
CASUI STI C AND METHOD
Th is qu an t it at iv e pr ospect iv e coh or t st u dy was carried out at four LSI E in three cities in Southern Minas Gerais St at e, select ed by t heir charact erist ics: philant hropic, non- profit organizat ions ( recognized as of Feder al Pu blic Ut ilit y an d r egist er ed u n der t h e Nat ional Social Service Council) , wit h sim ilar hum an and physical r esour ces.
I n this study, the LSI E are identified by letters - A, B, C, and D - so as t o pr eser v e et hic secr ecy r egar din g t h eir r eal n am es. At t h ese in st it u t ion s, healt h car e is not sy st em ized and t her e ar e no PU p r e v e n t i o n p r o t o co l s, i n cl u d i n g sp e ci f i c r i sk assessm ent for dev elopm ent or t r eat m ent . I n fact , t reat m ent is init iat ed when PU are det ect ed, usually from st age I I onwards.
The study population consisted of 275 elderly, r esident s in LSI E dur ing t he dat a collect ion per iod; distributed as follows: A= 56; B= 71; C= 46; and D= 102 elderly.
Ni n et y - f o u r el d er l y co m p r i sed t h e st u d y sam ple, and m et the following criteria: aged 60 years o r o l d e r ; Br a d e n Sca l e sco r e i n d i ca t i n g PU dev elopm ent r isk ; and agr eem ent t o par t icipat e in t he st udy. The exclusion of 181 elderly from several institutions occurred due to: age under 60 years ( 36) , total Braden score ≥ 19 ( 139) , refusal to take part in the study ( 6) . Moreover, three deaths occurred am ong t he elderly in t he final sam ple.
The lead r esear cher and nine collabor at or s collected the data. Collaborators participated in a six-st age t raining program , consisix-st ing of t heoret ical and pract ical classes, in addit ion t o group and individual assessm en t s. Th ey w er e con sid er ed ap t f or d at a collect ion w h en a 1 0 0 % agr eem en t w as obt ain ed a m o n g t h e si m u l t a n e o u s o b se r v a t i o n s m a d e b y collaborat or s and t he r esear cher. Folder s w it h dat a collect ion inst rum ent s, list s wit h t he resident elderly people’s nam es and the program for visiting days were appropriat ely organized for each LSI E.
Aft er r eceiv ing agr eem ent , w r it t en consent w as r eq u est ed . I n case t h e p ar t i ci p an t w as n o t phy sically or m ent ally capable of pr ov iding w r it t en consent , request s were m ade t o t hose responsible at t he inst it ut ion.
Aft er obt aining consent fr om t he elder ly or the person responsible and after checking their ages, t he nex t st ep w as t o assess UP dev elopm ent r isk , u sin g t h e Br aden Scale an d ph y sical ex am in at ion , aim ing to detect previous PU. Elderly with risk scores ≤ 1 8( 8) w er e included in t he st udy sam ple unt il PU
developm ent , deat h, t ransfer, “ discharge” or follow-up com plet ion ( 90 days) . Dat a collect ion t ook place in 2 0 0 4 , an d w as p er f or m ed t h r ee t im es a w eek ( Monday s, Wednesday s and Fr iday s) ; fr om June t o Sept em ber at inst it ut ions A and B, fr om August t o No v em b er a t i n st i t u t i o n C a n d f r o m Oct o b er t o Decem ber at inst it ut ion D. Elderly wit h previous PU
who st ill had a risk score were kept in t he st udy t o evaluat e t he occurrence of new lesions.
Elderly adm it t ed t o t he LSI E before t he 80t h
dat a collect ion day, w ho m et t he inclusion cr it er ia, were evaluated until com pleting at least 20 evaluation day s. When par t icipant s w er e t r ansfer r ed fr om t he LSI E to hospital or their hom e, they were considered new cases only if their return to LSI E occurred 3 days after they had left the institution.
During follow- up, when PU was det ect ed, a careful local exam was perform ed, evaluat ing st age, m e a su r e m e n t a n d l o ca t i o n . Fr o m t h i s m o m e n t onwards, elderly were excluded from t he st udy and lesion treatm ent was initiated, in accordance with the inst it ut ion’s pract ice.
Sociodem ographic and clinical dat a ( diseases and drugs used) were collect ed from t he inst it ut ion’s pat ient form and com plet ed at t heir side, during t he ph y sical ex am in at ion . Ot h er dat a, lik e w eigh t an d height , were collect ed t hrough individual evaluat ions, using standardized techniques and equipm ent in every LSI E. Techniques were adj ust ed t o part icipant s who were rest rict ed t o t heir beds.
Som e clinical variables, such as Body Mass I ndex ( BMI ) and PU stages, were evaluated according t o int er nat ional st andar ds( 1). PU m easur em ent w as
done with a m illim eter ruler: the length was m easured in t h e ceph alic- cau dal dir ect ion , an d w idt h in t h e latero- lateral direction. For ulcers in stages I I and I V, dept hs were evaluat ed using st erilized cot t on swabs, w h ich w er e lat er m easu r ed w it h t h e st an dar dized m illim et er rule. I rregular wounds were m easured by t h e l a r g e st d i m e n si o n s, a s p e r i n t e r n a t i o n a l r ecom m endat ions( 9).
Results were subj ected to the following tests: Pear son’s chi squar e, Fischer ’s ex act , Kolm ogor ov -Sm ir nov, St udent ’s t ; Mann- Whit ney and St ep w ise Fo r w a r d. Va r i a b l e a sso ci a t i o n s b e l o w . 0 5 w e r e considered st at ist ically significant .
RESULTS
Study results show that m ost participants were wom en ( 62.8% ) , whit e ( 68.1% ) , bet ween 60 and 103 y ear s old, w it h an av er age age of 7 9 . 1 ± 9 . 5 9 an d m edian of 80.5 years. The inst it ut ionalizat ion period ranged from 1 day t o 23,360 days.
elder ly had ur inar y sy st em diseases ( 5 8 . 4 % ) , and car diov ascular and r espir at or y condit ions ( 57. 4% ) . Neu r ological ( 4 7 . 9 % ) an d der m at ological ( 4 0 . 4 % ) diseases also st ood out . There w as frequent use of neurolept ic and psychot ropic drugs ( 52.1% ) , as well
as ant ihypert ensives ( 38.3% ) , wit h a m edian of t wo m edicat ion s per per son , w it h u p t o six dr u gs per per son. As t o sm ok ing, it w as obser v ed t hat m ost elder ly ( 8 0 . 1 % ) w er e n on - sm ok er s. Tw en t y- sev en elderly ( 28.7% ) had previous PU cases.
12,8%
35,1%
31,9%
46,8%
68,1%
37,2%
23,4%
48,9%
54,3% 25,5%
26,6%
45,7%
70,2%
16,0% 11,7%
25,5%
4,3% 5,3%
1,1% 2,1%
2,1% 3,2%
2,1%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Sensorial perception
Dampness Activity Mobility Nutrition Friction
Braden Scale - 1st assessment
1 2 3 4
12,8%
39,4%
35,1%
48,9%
67,0%
40,4%
29,8%
42,6%
54,3% 26,6%
24,5%
40,4%
61,7%
18,1% 7,4%
18,1%
6,4% 5,3%
5,3%
3,2% 6,4% 3,2%
3,2%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Sensorial perception
Dampness Activity Mobility Nutrition Friction
Braden Scale - final assessment
1 2 3 4
Figure 1 - Braden’s sub- scale score rat es, on t he 1st assessm ent
Figure 1 shows that, on the 1st risk assessm ent of the 94 elderly, the sub- scales m oist ure ( very wet) ,
act iv it y ( r est r ict ed t o w heelchair ) and f r ict ion an d shear ing ( pot ent ial problem ) scored highest .
Figure 2 - Braden’s sub- scale score rat es, on t he final assessm ent
The final assessm ent was different for each of the 94 elderly. I t depended on the event that caused
sh ow ed t h e h i g h est v al u es f or Cr on b ach ’s al p h a ( 0.6591 and 0.6631) . Moist u r e obt ained t he low est Cronbach’s alpha values ( 0.2001 and 0.3750) , for the first and final assessm ent s, respect ively.
I n t erm s of t he risk fact ors present am ong elderly w it h and w it hout PU, approxim at ely 55% of those with PU have score 2 ( very wet) on the m oist ure su b sca l e , o n t h e f i r st a sse ssm e n t , sh o w i n g a st at ist ically significant difference when com pared t o those without PU ( p= .021) .
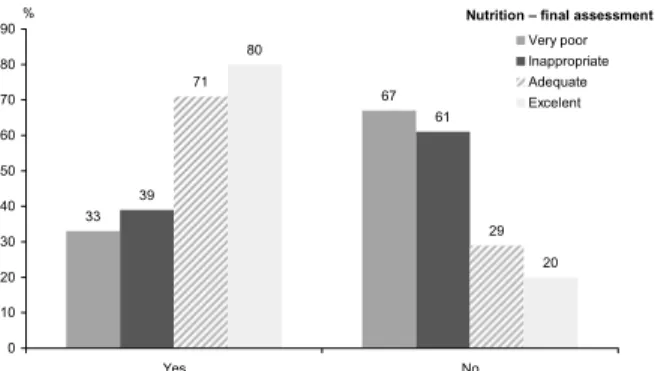
Figures 3, 4, and 5 identify the categories of h igh est r isk f or elder ly w it h PU, on t h e 3 Br aden subscales: m oist ur e ( com plet ely wet ) , nut r it ion ( very p o o r a n d i n a d eq u a t e) a n d f r i ct i o n a n d sh e a r i n g ( p r o b l em an d p o t en t i al p r o b l em ) . Al l cat eg o r i es sh o w ed st at i st i cal l y si g n i f i can t d i f f er en ces w h en com pared to the group of elderly without PU ( p= .034; p= .013, and p= .036, respect ively) .
For t h e t ot al Br ad en Scale scor e, r esu lt s showed a st at ist ically significant difference bet ween t he gr oups w it h and w it hout PU, for bot h t he fir st ( p= . 030) and final ( p= . 001) assessm ent s. Logist ic regression showed t hat fem ale gender and previous PU were predict ive fact ors for PU developm ent (odds rat io of 3.46 and 2.76, respect ively; r2= .311) .
DI SCUSSI ON
LSI E sh ow ed d if f icu lt ies r eg ar d in g eld er ly healt h m aint enance, especially because t hey oft en present ed organic syst em im pairm ent , including t he skin, due to the natural aging process, associated with ch r on ic- d eg en er at iv e d iseases t h at cau se v ar iou s ch a n g e s, m a k i n g e l d e r l y w e a k e r a n d m o r e v ulner able( 5).
I n a d d i t i o n , o t h e r c h a n g e s , s u c h a s d e m e n t i a , n e u r o - m o t o r a n d m u s c u l a r - s k e l e t a l im pair m ent s, also com m on am ong t he elder ly and oft en t he cause of t heir inst it ut ionalizat ion, lim it t heir lif est y le, self car e an d act iv it ies. Th er ef or e, t h is cert ainly affect s t heir sensorial percept ion, m obilit y, act ivit y, nut rit ion and m oist ure, as clinical fact ors of PU risk( 3).
An al an d u r in ar y in con t in en ce ar e f or m er clinical situations that require specific approaches due t o t he involved prej udice, m yt hs and t aboos, which m ade diagnosis and t r eat m ent difficult . This led t o perm anent m oisture and often turned these situations i n t o t h e m a i n r e a so n f o r t h e e l d e r l y p e o p l e ’ s inst it ut ionalizat ion.
Th is ar r ay of im pair m en t s an d f r agilen ess im ply specific health care needs. These needs require hum an or physical support that is often possible only t hrough inst it ut ionalizat ion. However, as opposed t o w h at is ex pect ed, in st it u t ion alizat ion can in cr ease t hese client s’ dependence and lack of aut onom y.
Since pr ev ent ion is st ill t he best m edicine, this study aim ed to investigate risk factors present in t he inst it ut ionalized elderly.
50 50 50 50
64
36 88
12
0 10 20 30 40 50 60 70 80 90 100
Yes No
Completely wet Very wet Occasionally wet Rarely wet %
Moisture – final assessment
33
67
39
61 71
29 80
20
0 10 20 30 40 50 60 70 80 90
Yes No
Very poor Inappropriate Adequate Excelent
% Nutrition – final assessment
54
46 55
45 88
12
0 10 20 30 40 50 60 70 80 90 100
Yes No
Problem Potential Problem No problem
% Friction/shearing
Figure 3 - Elderly wit h and wit hout PU, according t o m oist ure subscale scores on t he final assessm ent
Figure 4 - Elderly wit h and wit hout PU, according t o nut rit ion subscale scores on t he final assessm ent
Am ong t he 2 7 5 r esident s in t he four LSI E under st udy, 94 were included in t he st udy sam ple, since they were at risk of developing PU. Most elders were white wom en, with an average age of 79 years. Hospitalization periods were long ( average of 11 years and m edian of 5 years) , which varies am ong LSI E.
Clinically, LSI E elder ly w er e w it hin nor m al nutritional standards, with none to six illnesses each, m ost ly ur inar y, car diovascular and r espirat or y. The m ost f r eq u en t d r u g s u sed w er e n eu r olep t ics an d p sy ch ot r op ics. Th ese con d it ion s, associat ed w it h previous PU, which is t he case of approxim at ely one third of the elderly, in addition to m obilit y im pairm ent - as the m ost im portant risk on both the first and final a sse ssm e n t s - ca u se d h i g h e r v u l n e r a b i l i t y t o dev eloping t hese lesions. Anot her st udy pr ev iously described the use of sedatives as a risk factor for PU developm ent , since pat ient s do not feel t he need t o change posit ions, t hus com pr om ising t he m obilit y / act ivit y fact or( 10).
I n t his sense, during dat a collect ion, it was obser v ed t hat t he elder ly dev eloped few act iv it ies. Th ey at e an d sl ep t , f ew p er f or m ed occu p at i on al therapy and, despite being encouraged, they reported t iredness and lack of vit alit y. This led t o a need for long rest periods, which affected activity and m obility lev els.
Despit e t he pr evalence of ur inar y diseases, as a general charact erist ic for t he 94 st udied elderly, there was no difference between the groups with and wit hout PU. Nevert heless, m oist ur e - being very wet - showed a statistically significant association with the presence of PU on both the first and final assessm ents. Ex ce ssi v e m o i s t u r e, e sp e ci a l l y d u e t o u r i n a r y incontinence, also relates with frict ion and shearing( 11), which are com m on am ong elderly wit h PU, as a real or pot ent ial problem on t he final assessm ent .
An al an d u r in ar y in con t in en ce ar e clin ical sit uat ions t hat require specific approaches, since t he r esu l t i n g p er m an en t m o i st u r e o f t en t u r n s t h ese sit uat ions int o t he m ain r eason for t hese people’s inst it ut ionalizat ion.
Though m ost elderly have a norm al BMI , their food consum ption - evaluated by the Braden nutrition subscale - was com prom ised. Very poor or inadequate n u t r it ion w as pr esent in 51.3% of elder ly w it h PU, which was significantly different from the group without PU. LSI E f r eq u en t l y r ep o r t d i f f i cu l t i es r eg ar d i n g in d ep en d en ce t o eat . A st u d y t h at assessed t h e in f lu en ce of BMI on t h e glu t eal- isch iat ic in t er f ace
pressure in a populat ion of inst it ut ionalized elderly( 12)
evidenced t hat pressure on t his region was higher in thin elders with low BMI . Despite our findings, another st u d y( 1 3 ) sh o w e d t h a t e v e r y su b - sca l e , e x ce p t nut rit ion, presented statistically significant associations t hat indicat ed t he risk of ulcerat ion.
Ot her aut hors( 14) describe hypoalbum inem ia,
low diast olic pressure, anal and urinary incont inence and peripheral edem a as factors that cause PU am ong elderly in rehabilitation units. Not all these factors were invest igat ed in t he present st udy. Nevert heless, t he p r esen ce of t h ese co- m or b id it ies is an im p or t an t epidem iological f act f or f u r t h er copin g w it h t h ese condit ions. I n t he referred st udy, Braden sub- scales w er e classif ied as p r im ar y r isk f act or s; an d ag e, edem a and hypot ension w er e consider ed secondar y fact ors for developing PU. Result s for prim ary fact ors w er e sim ilar t o t hose of t he pr esent st udy, for t he sam e su b- scales: m oist u r e, n u t r it ion , f r ict ion an d shear ing.
I t w as obser v ed t hat w om en and pr ev ious PU are predictive of PU occurrence, com pared to m en and elderly wit hout previous lesions.
Am on g t h e su r v ey ed st u d ies, d esp it e t h e prevalence of wom en in m ost, PU incidence was higher am ong m en, wit h no epidem iological foundat ions for bot h findings. As for pr ev ious PU, only one of t he st u d i es( 1 5 ) r ep o r t s t h e h i g h er sev er i t y o f el d er l y
adm it t ed wit h PU, indicat ing higher m ort alit y. Th e sig n if ican t d if f er en ces b et w een t ot al Braden Scale scores for elderly wit h and wit hout PU, on t he first and final assessm ent s, always lower for t he first group, confirm t he im port ance of syst em at ic r i sk a sse ssm e n t t o i m p l e m e n t e a r l y p r e v e n t i v e m easu r es.
I n a st u d y a b o u t t h i s sca l e ’ s p r e d i ct i v e v alid it y, t h e au t h or( 1 4 ) d em on st r at ed t h at scor es
decreased in every sub- scale when subj ect s had PU. I n anot her longit udinal prospect ive st udy( 16)
Finally, it should be stated that risk assessm ent - based on knowledge concerning specific factors - in ad d it ion t o ear ly p r ev en t ion an d in t er v en t ion ar e cr ucial for appr oaching t he t hr eat ening pr ev alence and incidence of PU in t his populat ion.
FI NAL CONSI DERATI ONS
Population aging, including in our country, has caused a significant increase in the so-called LSIE. These facilities are an alternative residence for elderly and all of them admit that they should undergo significant changes in structure and human resources over the next decades. Regarding the elderly, it is observed that this gener at ion did not hav e access t o infor m at ion lik e today. Perhaps this causes a passive approval of aging, different from t oday’s adult s, who seem t o st ruggle to stop tim e. I t is m ost likely that the vast m aj ority is a l r e a d y co n ce r n e d w i t h h o w t h e y w i l l l i v e t h e senescence phase. Nursing should m ake m ore use of t hese t echnological alt er nat iv es in t he educat ional process of fam ilies and pat ient s.
By knowing and det ect ing t he prevailing risk fact ors of PU developm ent in inst it ut ionalized elderly,
as w ell as t heir influence on sensor ial per cept ion, m obilit y, act ivit y, m oist ure and frict ion and shearing, it is possible t o elaborat e and syst em ize prophylact ic nursing and m ult idisciplinary m easures.
Am ong t he fact ors ident ified in t his st udy, it should be r ecognized t hat m ob ilit y appear ed t o be one of t he m ost im port ant for t he occurrence of PU. The m ult iple causalit y of t hese lesions, however, also shows that changes in sensorial perception - also due t o cont inuous m edicat ion use, such as neurolept ics/ p sy ch ot r op ics- as w ell as t h e id en t if ied illn esses, especially urinary - which com prom ise m oist ure and ca u se f r i ct i o n a n d sh e a r i n g - co n f i r m t h e ch a r a ct e r i za t i o n o f a p o p u l a t i o n t h a t i s h i g h l y vulnerable t o developing t hese chronic lesions.
Elder ly an d car egiv er s, eit h er pr ofession al or n ot , sh ou ld be con st an t ly in st r u ct ed abou t t h e i m p or t an ce of an d m easu r es f or p r essu r e r el i ef, reviewing and im plem ent ing sim ple procedures, such as changing decubit us, correct ly using m obile sheet s, sit t in g an d ly in g p osit ion s, p r ev en t in g m ov em en t fr ict ion, cont r olling m oist ur e, as w ell as facilit at ing an d en co u r ag i n g eat i n g an d h y d r at i o n ; w h i ch i s e s s e n t i a l f o r t h e e l d e r l y, p a r t i c u l a r l y w h e n inst it ut ionalized.
REFERENCES
1. Nat ional Pressure Ulcer Advisory Panel [ hom epage on t he I nt er net ] . Unit ed St at es of Am er ica; [ cit ed 2006 Apr 26] . Pressure Ulcer Definit ion and Et iology. Available from : ht t p: / / www.npuap.org/ pressureulcerdef.ht m l
2. Eur opean Pr essur e Ulcer Adv isor y Panel [ hom epage on t he I nt ernet ] . Unit ed Kingdom ; [ cit ed 2006 Apr 26] . Pressure Ul ce r Tr e a t m e n t Gu i d e l i n e s. Av a i l a b l e f r o m : h t t p : / / www.epuap.org/ glt reat m ent .ht m l
3. Br aden BJ, Ber gst r om NA. A concept ual schem e for t he st udy of t he et hiology of pressure sores. Rehab Nurs 1987 Januar y - Febr uar y ; 12( 1) : 8- 12.
4. Nascim ent o LV. Derm at ologia do idoso. I n: Cucé LC, Fest a CN. Manual de derm at ologia 2ed. São Paulo: At heneu; 2001. p . 5 3 7 - 4 2 .
5 . So u za D MST, San t o s VLCG. Ùl cer as p o r p r essão e envelhecim ento. Rev Estim a 2006 j aneiro- m arço; 4( 1) : 36- 44. 6. Sociedade Brasileira de Geriat ria e Geront ologia ( SBGG) . I nst it uição de longa per m anência par a idosos: m anual de funcionam ent o. Biênio 2002- 2003.
7. Bergst rom N, Braden BJ, Laguzza A, Holm an V. The Braden Scale for predict ing pressure sore risk. Nurs Res 1987 July-Au g u st ; 3 6 ( 4 ) : 2 0 5 - 1 0 .
8. Ram undo JM. Reliabilit y and validit y of t he Braden Scale in t he hom e care set t ing. J WOCN. 1995 May; 22( 3) : 128- 34.
9. Cooper DM. Assessm ent , Measur em ent , and Evaluat ion: Th e i r Pi v o t a l Ro l e s i n W o u n d H e a l i n g . I n : Br y a n t RA, organizadora. Acut e & chronic wounds: nursing m anagem ent . Missou r i: Mosby ; 2 0 0 0 . p. 5 1 - 8 3 .
1 0 . Sm it h DM. Pr essur e ulcer s in t he nur sing hom e. Ann I nt er n Med 1995 Sept em ber 15; 123( 6) : 433- 42.
11. Maklebust J. Pressure ulcers: decreasing risk for old adult. Ger iat r Nur s 1997 Nov em ber - Decem ber ; 18( 6) : 250- 4. 12. Kernozek TW, Wilder PA, Am undson A, Hum m er J. The effect s of body m ass index on peak seat - int erface pressure of inst it ut ionalized elderly. Arch Phys Med Rehabil 2002 June; 8 3 ( 6 ) : 8 6 8 - 7 1 .
13. Bergquist S. Subescales, subscores, or sum m at ive score: evaluat ing t he cont ribut ion of Braden Scale it em s for predict ing pressure ulcer risk in older adult s receiving hom e healt h care. J WOCN 2 0 0 1 Nov em ber ; 2 8 ( 6 ) : 2 7 9 - 8 9 .
1 4 . Sch u e RM, Lan g em o DK. Pr ev alen ce, in cid en ce an d predict ion of pressure ulcers on a rehabilit at ion unit . J WOCN 1 9 9 9 May ; 2 6 ( 3 ) : 1 2 1 - 9 .
15. Brandeis GH, Morris JN, Nash DJ, Lipisit L. The epidem iology and natural history of pressure ulcers in elderly nursing hom e r esident s. JAMA 1990 Decem ber 12; 264( 22) : 2905- 9. 16. Pieper B, Sugrue M, Weiland M, Sprague K, Heim ann C. Presence of pressure ulcer prevent ion m et hods used am ong pat ient s consider ed at r isk v er sus t hose consider ed not at r isk . J WOCN 1997 July ; 24( 4) : 191- 9.