ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Familial
autoimmunity
and
polyautoimmunity
in
60
Brazilian
Midwest
patients
with
systemic
sclerosis
Alex
Magno
Coelho
Horimoto
a,b,c,∗,
Aida
Freitas
do
Carmo
Silveira
c,
Izaias
Pereira
da
Costa
c,d,e,faUniversidadeFederaldeMatoGrossodoSul(UFMS),CampoGrande,MS,Brazil
bServiceofRheumatology,HospitalRegionaldeMatoGrossodoSul,CampoGrande,MS,Brazil
cProgramofMedicalResidenceinRheumatology,UniversidadeFederaldeMatoGrossodoSul(UFMS),CampoGrande,MS,Brazil dFaculdadedeMedicina,UniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
eDepartmentofInternalMedicine,FaculdadedeMedicina,UniversidadeFederaldeMatoGrossodoSul(UFMS),CampoGrande,MS,
Brazil
fServiceofRheumatology,HospitalUniversitário,HospitalMariaAparecidaPedrossian,UniversidadeFederaldeMatoGrossodoSul
(UFMS),CampoGrande,MS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received26December2014
Accepted1September2015
Availableonline8February2016
Keywords:
Autoantibodies
Systemicsclerosis
Autoimmunedisease
Polyautoimmunity
Familialautoimmunity
a
b
s
t
r
a
c
t
Introduction:Systemicsclerosis(SSc)isaconnectivetissuediseaseofunknownetiology,
characterizedbyatriadofvascularinjury,autoimmunityandtissuefibrosis.Itisknownthat
apositivefamilyhistoryisthegreatestriskfactoralreadyidentifiedforthedevelopmentof
SScinagivenindividual.Preliminaryobservationofahighprevalenceofpolyautoimmunity
andoffamilialautoimmunityinSScpatientssupporttheideathatdifferentautoimmune
phenotypesmaysharecommonsusceptibilityvariants.
Objectives:Todescribethefrequencyoffamilialautoimmunityandpolyautoimmunityin
60SScpatientsintheMidwestregionofBrazil,aswellastoreportthemainautoimmune
diseasesobservedinthisassociationofcomorbidities.
Methods:Across-sectionalstudywithrecruitmentof60consecutivepatientsselectedat
theRheumatologyDepartment,UniversityHospital,MedicineSchool,FederalUniversityof
MatoGrossodoSul(FMUFMS),aswellasinterviewsoftheirrelativesduringtheperiodfrom
February2013toMarch2014.
Results:Afrequencyof43.3%ofpolyautoimmunityandof51.7%offamilialautoimmunity
inSScpatientswasfound.Patientswiththe presenceofpolyautoimmunityand
famil-ialautoimmunitypresentedprimarilythediffuseformofSSc,butthisindicatordidnot
reachstatisticalsignificance.Theautoimmunediseasesmostfrequentlyobservedin
polyau-toimmunitypatientswere:Hashimoto’sthyroiditis(53.8%),Sjögren’ssyndrome(38.5%),and
inflammatorymyopathy(11.5%).ThemainautoimmunediseasesobservedinSScpatients’
relativeswere:Hashimoto’sthyroiditis(32.3%),rheumatoidarthritis(22.6%),andSLE(22.6%).
ThepresenceofmorethanoneautoimmunediseaseinSScpatientsdidnotcorrelatewith
diseaseseverityoractivity.
∗ Correspondingauthor.
E-mail:[email protected](A.M.C.Horimoto).
http://dx.doi.org/10.1016/j.rbre.2016.01.003
2255-5021/©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
Conclusions: FromthehighprevalenceofcoexistingautoimmunediseasesfoundinSSc
patients,westresstheimportanceoftheconceptofsharedautoimmunity,inorderto
pro-moteacontinuedvigilanceandpromptlydiagnoseotherpossibleautoimmunediseasein
patients,orintheirkin.
©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense
(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Autoimunidade
familial
e
poliautoimunidade
em
60
pacientes
portadores
de
esclerose
sistêmica
da
região
Centro-Oeste
do
Brasil
Palavras-chave:
Autoanticorpos
Esclerosesistêmica
Doenc¸aautoimune
Poliautoimunidade
Autoimunidadefamiliar
r
e
s
u
m
o
Introduc¸ão: Aesclerosesistêmica(ES)éumaenfermidadedotecidoconjuntivode
etiolo-giadesconhecida,caracterizadapelatríadedeinjúriavascular,autoimunidadeefibrose
tecidual.Sabe-sequeumahistóriafamiliarpositivarepresentaomaiorfatorderiscojá
iden-tificadoparaodesenvolvimentodaESemumdeterminadoindivíduo.Observac¸ãoprévia
dealtaprevalênciadepoliautoimunidadeedeautoimunidadefamiliarempacientescom
ES,reforc¸aaideiadequefenótiposautoimunesdistintospodemdividirvariantescomuns
desusceptibilidade.
Objetivos:Descreverafrequênciadeautoimunidadefamiliaredepoliautoimunidadeem60
pacientescomESdaregiãoCentroOestedoBrasil,bemcomorelatarasprincipaisdoenc¸as
autoimunesobservadasnestaassociac¸ãodecomorbidades.
Métodos: Realizou-seumestudotransversalcomrecrutamentode60pacientes
consecu-tivos,selecionadosnoServic¸odeReumatologiadoHospitalUniversitáriodaFaculdadede
MedicinadaUniversidadeFederaldeMatoGrossodoSul(FMUFMS),bemcomoentrevista
deseusparentes,duranteoperíododefevereirode2013amarc¸ode2014.
Resultados: Foiencontradaumafrequência de43,3% depoliautoimunidade ede 51,7%
deautoimunidadefamiliarnospacientescomES.Ospacientescompresenc¸ade
poliau-toimunidadeede autoimunidadefamiliareram principalmentedaforma difusadeES,
porémesteíndicenãoatingiusignificânciaestatística.Asdoenc¸asautoimunesmais
comu-menteobservadasnospacientescompoliautoimunidadeforam:tireoiditedeHashimoto
(53,8%),síndromedeSjögren(38,5%)emiopatiainflamatória(11,5%).Asprincipaisdoenc¸as
autoimunesobservadasnosparentesdospacientescomESforam:tireoiditedeHashimoto
(32,3%),artritereumatóide(22,6%)eLES(22,6%).Apresenc¸ademaisdeumaenfermidade
autoimuneempacientescomESnãosecorrelacionoucommaiorgravidadeouatividadeda
doenc¸a.
Conclusões:Apartirdaaltaprevalênciaencontradadedoenc¸asautoimunescoexistentesem
pacientescomES,salientamosaimportânciadoconceitodeautoimunidadecompartilhada,
deformaapromoverumavigilânciaconstanteediagnosticarprontamenteumapossível
outradoenc¸aautoimunenospacientesouemseusfamiliares.
©2016ElsevierEditoraLtda.EsteéumartigoOpenAccesssobalicençadeCC
BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Systemicsclerosis(SSc)isadiseaseoftheconnectivetissue
withanautoimmunecharacter,andwithextreme
heterogene-ityinitsclinicalpresentation,withinvolvementofmultiple
systemsandfollowingavariedandunpredictablecourse.1Its
etiologyremainsunknown,andamultifactorialcauseis
sug-gested;possiblySScistriggeredbyenvironmentalfactorsina
geneticallypredisposedindividual.2
The hallmark of SSc is the occurrence of
microvascu-lopathy, fibroblast activation and an excessive production
ofcollagen.3 Thisisauniquecondition,becauseitdisplays
featuresofthree distinct pathophysiologicalprocesses, the
so-called triad of vascular injury, autoimmunity (cellular
and humoral), and tissue fibrosis, leading to cutaneous
involvement,besidesaffectingmultipleinternalorgans,for
instance, lungs, heartand gastrointestinal tract,aswell as
musculoskeletalmanifestations.3,4
Thegeneticcomponentofautoimmunediseasesis
repre-sentedbytheincreasedriskofdevelopingSScintwinbrothers
ofaffectedindividuals.3,4 Basically,SScisnotagenetic
dis-order,butthereisconsensusthat,actually,thediseasehas
ageneticcomponentbasedonreportsofmonozygotictwins
withapropensitytoSSc.5
In1953,ReesandBennett6describedthefirstcaseof
local-izedsclerodermainafatherandhisdaughter.Later,several
reportsoffamilialsclerodermaindifferentpopulationsand
familyrelationshipswerepublished.2,5,7Moreover,an
associ-ationbetweenHLAandSSchasbeendescribed.5,8,9
A positivefamily history isthe greatest riskfactor ever
However,thelowfrequencyofconcordancerateof
autoim-mune diseases among siblings versus monozygotic twins
favorsthepresenceofmultiplegenescontributingtoagenetic
predisposition,includingSSc.11
Hudsonetal.usedtheterm“autoimmunitykaleidoscope”
inreference toSSc patientstodescribe the factthat more
thanonedifferentautoimmunediseasemaycoexistina
sin-gle patient (polyautoimmunity) or in the same household
(familial autoimmunity).12 The high prevalence of
polyau-toimmunity(38%)aswellasoffamilialautoimmunity(36%)
in SSc patients reinforces the idea that clinically distinct
autoimmunephenotypesmayshare commonsusceptibility
variants.12
Objectives
Inthis study,we aimtodescribethe frequencyoffamilial
autoimmunityandpolyautoimmunityin60SScpatientsliving
inthe MidwestregionofBrazil,toreportthemain
autoim-munediseasesobservedinthisassociationofcomorbidities,
andalsotoevaluateifthepresenceofmorethanone
autoim-munediseaseinSScpatientsisassociatedwithanincreaseof
diseaseactivityorseverity.
Methods
Thisisanobservational,cross-sectionalstudy.
Sixty consecutive patients were seen and selected at
theRheumatologyDepartment,UniversityHospital,Medicine
School,FederalUniversityofMatoGrossodoSul(FMUFMS)
duringtheperiodfromFebruary2013toMarch2014.
Toparticipateinthisstudy,thepatientsshouldmeetthe
followingcriteria:
– Complywiththenew2013classificationcriteriaforSSc13;
– Intheabsenceofskinthickening,thepatientsshould
com-plywithLeRoyandMedsger14criteriaforearly-onsetSSc.
– Allpatientswhohadotherassociatedinfectiousdiseasesor
malignancieswereexcluded.
The study was approved by the Ethics Committee on
ResearchoftheFederalUniversityofMatoGrossodoSul
(opin-ionCAAE:31442614.3.0000.0021).
Polyautoimmunitywasdefinedasthe occurrenceofany
otherautoimmunediseaseobservedinpatientswithsystemic
sclerosis.Familialautoimmunitywas definedasthe
occur-renceofanyotherautoimmunediseaseaffectingancestors
(grandparents,mother,fatherbyblood)orblooddescendant
relatives(daughters,sons, granddaughters,grandsons)
rela-tives,or second-(sisters, brothers) orthird-(aunts, uncles,
niecesandnephews)degreecollateralSScpatients’relatives.
Toconfirmthe illnessesassociatedwithSSc patientsor
withtheirfamilies,thefollowingcriteriawereused:
– Forsystemiclupuserythematosus(SLE):compliancewith
the newSLE classificationcriteria (2012 ofthe Systemic
LupusInternationalCollaboratingClinics(SLICC)forlupus
derivationandvalidation.15
– Sjögren’ssyndrome(SS):the diagnosis wasbasedon the
AmericanCollegeofRheumatology(ACR)criteriaof2012.16
– Rheumatoid arthritis (RA): RA classification criteria of
ACR/EULAR2010.17
– Psoriasis:diagnosisbasedonclinicalcriteria18 and,when
necessary,onahistopathologicalstudy.
– Pemphigus:clinicalcriteriawereused18 through
cytologi-calanalysis,histopathologicalstudyand/orimmunological
testsfordetectionofantiepithelialantibodies.
– Vitiligo:clinicalcriteriawereused:18historyandphysical
examination,aswellasWoodlamptechnique.
– Spondyloarthritis:newclassificationcriteria(2011)foraxial
andperipheralespondiloartritritesbyASAS(Assessmenton
SpondyloarthritisInternationalSociety)groupwereused.19
– Crohn’sdisease:criteriafromtheAmericanCollegeof
Gas-troenterology’sPracticeParameterCommittee2001.20
– Antiphospholipidsyndrome:criteriafromtheinternational
consensus(2006)forupdatingantiphospholipidsyndrome
classificationanddefinition.21
– Hashimoto’s thyroiditis: the diagnosis was based on
the presence of anti-thyroid peroxidase and/or
anti-thyroglobulin antibodies in association with thyroid
parenchyma ultrasonographic changes compatible with
thyroiditis.22
– Diabetesmellitustype1:criteriaoftheAmericanDiabetes
Association,basedonglycatedhemoglobin,fastingglucose,
oralglucosetolerancetestandclassicsymptomsof
hyper-glycemia,revisedin2010.23
– Mixedconnectivetissuedisease(MCTD):criteriaof
Alarcon-Segovia,1989.24
– Inflammatorymyopathy:BohanandPetercriteria,1975.25
– Localizedscleroderma:thediagnosiswasbasedmainlyon
visualexamination,takingintoaccountthecharacteristics
commonlyobservedinskinlesions,plusaskinbiopsy
con-sistentwithincreasedcollagendeposits.18
Weobtainedtheinformationnecessaryfora
sociodemo-graphicandclinicalcharacterizationofthediseasethrough
ananalysisofthemedicalrecordsofeachpatient,with
com-pletionbypatientinterviews.Atthefirstvisit,demographic
andclinicaldatawerecollected,includingdiseaseduration,
yearofdiagnosis,Rodnanskinscore(modified),26
autoanti-bodytests,afullclinicalexamination,andcurrenttreatment.
Subsequently, all patients were evaluated and interviewed
withrespecttoallfamilymembers,inordertoconfirmthe
occurrenceofotherautoimmunediseases.
Attheinitialevaluationofthepatient,wecollected
spe-cificdataonMedsgerseveritycriteria,27Valentinicriteriafor
diseaseactivity28andSclerodermaHealthAssessment
Ques-tionnaire(sHAQ).29
In our study, we used sera from patients previously
selected. Thesamples were properly frozen to −50◦C and
storedinthelaboratoryattheUniversityHospitalofUFMS.
a. Antinuclearantibodies(ANA)–anindirect
immunofluores-cencetechniquewasusedforANAtest,andHEp2cellswere
usedassubstrate(Faartechnique).TheIIBrazilian
Consen-susonAntinuclear FactorinHep-2cells(2003)criteria30
Serawereconsideredpositivewithatitle≥160anddiluted
toobtainfluorescencenegativity.
Serawereconsideredpositivewithatitle≥160anddiluted
untilanegativeresultoffluorescencehasbeenobtained.
b. Anti-Sm,anti-RNP,anti-Jo1,anti-Ro(SSA)andanti-La(SSB)
test–enzyme-linkedimmunosorbentassay(ELISA)
tech-nique was used, as previously described by McClain;31
specifickitswereusedassubstrateforeachtest,according
to the manufacturer’s specifications (Hemagen
Diagnos-tics,Inc.).Weconsideredapositiveresultforthesample
whenthevaluefoundwas≥3-foldgreaterthanthecutoff
point.
c. Rheumatoid Factor test – nephelometry technique was
used; the sample was considered positive with a title
>40IU/ml.
d. Anti-thyroglobulin and anti-thyroid peroxidasetests – a
chemiluminescentmicroparticleimmunoassaytechnique
was used according to the manufacturer’s
instruc-tions (Abbott ARCHITECT anti-Tg and anti-TPO,
chemi-luminescentmicroparticleimmunoassayforquantitative
determination of autoantibodies of IgG class
anti-thyroglobulinandthyroidperoxidaseinhumanserumand
plasma).Foranti-thyroglobulin,thetestwasconsideredas
non-reactiveif<40.0IU/ml,andasreactiveif>40.0IU/ml.
For anti-thyroid peroxidase, the test was considered as
non-reactiveif<35.0IU/ml,andasreactiveif>35.0IU/ml.
e. Anticentromeretest–indirectimmunofluorescence
tech-nique, with HEp2 cells as substrate,according to the II
BrazilianConsensusonAntinuclearFactorinHep-2cells
(2003)criteria30forinterpretationofresults.
f. Anti-DNAtopoisomerase1(anti-Scl70)test–anenzymatic
immunoassaytechnique32wasusedwiththespecifickit
QUANTA LiteTM Scl-70 from INOVALaboratory (INOVA
Diagnostics, Inc., San Diego, CA, USA), according tothe
manufacturer’sspecifications.Thetestwasconsideredas
non-reactiveif<20units;weaklyreactiveifbetween20and
39units;moderatelyreactiveifbetween40and80units;
andhighlyreactive(highvalues)if>80units.
g. Anti-RNApolymeraseIIIantibody–ELISAwasusedas
pre-viouslydescribed33withthespecifickitQUANTALiteRNA
Pol III ELISA INOVALaboratory(INOVA Diagnostics, Inc.,
SanDiego,CA,USA),accordingtothemanufacturer’s
spec-ifications.Thetestwasconsideredasnon-reactiveif<20
units;weaklyreactiveifbetween20and39units;
moder-atelyreactiveifbetween40and80units;andhighlyreactive
(highvalues)if>80units.
Statisticalanalysis
Thecomparisonbetweenpatientswithandwithout
polyau-toimmunityandfamilialautoimmunity,withrespecttothe
quantitativevariablesevaluatedinthisstudy,wascarriedout
usingStudent’sttest.Thechi-squaredtestwasusedtoassess
theassociationbetweenthepresenceorabsenceof
polyau-toimmunityandfamilialautoimmunitywiththequalitative
variablesmeasuredinthisstudy.Theresultsoftheother
vari-ablesassessedinthisstudy were presentedintheformof
descriptivestatistics,orintablesandgraphs.Statistical
anal-ysiswasperformedusingthesoftwareSPSS,version20.0,and
a5%significancelevelwasconsidered.
Results
Table 1 shows, indescending order, the diseases observed
amongpolyautoimmunitypatients,andamongpatients’
rela-tives in whom familial autoimmunity was diagnosed. The
mostfrequentillnessesamongpatientswith
polyautoimmu-nitywereHashimoto’sthyroiditis(n=14–53.8%),Sjögren’s
dis-ease(n=10–35.8%)andinflammatorymyopathy(n=3–11.5%).
Ontheotherhand,themostfrequentautoimmunediseases
observedinSScpatients’relativeswereHashimoto’s
thyroidi-tis (n=10–32.3%),rheumatoid arthritis(n=7–22.6%)andSLE
(n=7–22.6%).
Table 2showsthe number ofconcomitant autoimmune
diseasesinSScpatients.Thevastmajority(n=19–73.08%)of
patientshadonlyoneautoimmunediseaseassociatedwith
SSc.Among patientswithtwo other autoimmune diseases
concomitantlywithSSc(n=6–23.08%),oneofthesewasalways
Hashimoto’sthyroiditis,andtheotherautoimmunediseases
were:3patients alsowithSjögren’ssyndrome, onepatient
withpolymyositis,1patientwithpsoriasis,and1patientwith
type1diabetes.Onlyone(3.84%)patient(awoman)hadmore
than three concomitant diseases (SSc, Sjögren’ssyndrome,
Hashimoto’sthyroiditis,andpolymyositis).
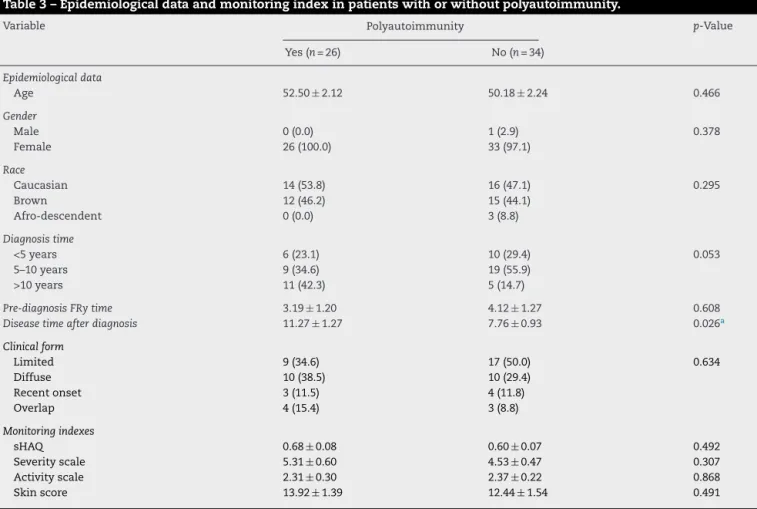
Theresultsregardingepidemiologicaldataand
monitor-ingindexinpatientswithandwithoutpolyautoimmunityare
showninTable3,whiletheresultsregarding
epidemiologi-caldataandmonitoringindexinpatientswithandwithout
familialautoimmunityarepresentedinTable4.
The time elapsed after the diagnosis of the disease
among polyautoimmunity patients (11.27±1.27 years) was
Table1–Diseasesmostfrequentlyobservedamong polyautoimmunitypatientsandamongSScpatients’ relativesandfamilialautoimmunity.
Variable n(%)
Polyautoimmunity(n=26)
Hashimoto’sthyroiditis 14(53.8)
Sjögren’ssyndrome 10(38.5)
Inflammatorymyopathy 3(11.5)
Type1Diabetesmellitus 3(11.5)
APS 2(7.7)
Rheumatoidarthritis 1(3.8)
Crohndisease 1(3.8)
Psoriasis 1(3.8)
Familialautoimmunity(n=31)
Hashimoto’sthyroiditis 10(32.3)
Rheumatoidarthritis 7(22.6)
SLE 7(22.6)
Systemicsclerosis 5(16.1)
Type1Diabetesmellitus 3(9.7)
Scleroderma 2(6.5)
Sjögren’ssyndrome 2(6.5)
Vitiligo 2(6.5)
Crohn’sdisease 1(3.2)
MCTD 1(3.2)
Pemphygus 1(3.2)
Spondyloarthritis 1(3.2)
MCTD,mixedconnectivetissuedisease.
Table2–Numberofconcurrentautoimmunediseasesin patientswithadiagnosisofsystemicsclerosis(n=26).
Numberofotherconcurrentdiseases n(%)
1 19(73.08)
2 6(23.08)
≥3 1(3.84)
Theresultsarepresentedinabsolutefrequency(relativefrequency).
significantly greater than this time for patients without
polyautoimmunity. On the other hand, wefound no other
significant difference between patients with and without
polyautoimmunity, with respect to other quantitative and
qualitativevariables.
Nosignificantdifferencebetweenpatientswithand
with-out familial autoimmunity was observed in relation to
quantitativeorqualitativevariables.
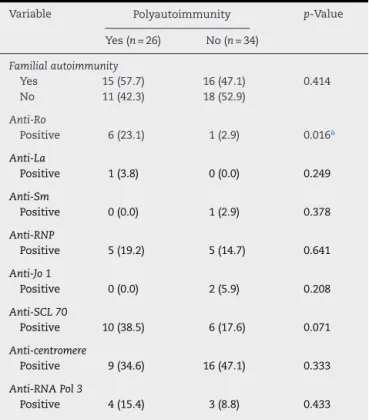
Tables 5 and 6 present, respectively, distributions of
patientswithorwithoutpolyautoimmunityandwithor
with-outfamilialautoimmunityinrelationtoresultsoflaboratory
tests. It was observed that the percentage of
polyautoim-munity patients positive for anti-Ro antibody (n=6–23.1%)
wassignificantlyhigherthanthatofthosepatientswithout
polyautoimmunity(n=1–2.9%;p=0.016).Nootherstatistical
significancewasfoundbetweenthepresenceorabsenceof
polyautoimmunityandfamilialautoimmunity.
Inthisstudy,thepercentageofpolyautoimmunitypatients
withapositiveanticentromereantibody(n=9–29.0%)was
sig-nificantly lower versus patients without polyautoimmunity
(n=16–55.2%; p=0.040). However,no association wasfound
betweenthe presenceor absenceoffamilialautoimmunity
andtheresultforotherautoantibodies.
Discussion
The coexistence of several autoimmune diseases in SSc
patients (polyautoimmunity) is well established.12,34–38 The
aggregationofvariousautoimmunediseasesinfamiliesofSSc
patientsisbeingalsoincreasinglyrecognized.12,36,37,39
Many genetic factors that confer susceptibility to SSc
were recentlyidentified and are primarilyrelated togenes
coding forproteins responsible for transduction of signals
that comprise autoimmunity pathways common to many
diseases.12,39–41 In this group, polymorphisms related to
innate immunitypathways (IRF5), activation and
differen-tiationofT lymphocytes(STAT4,PTPN22)and autoimmune
intracellular signaling pathways(BANK1, BLK, TNFAIP3) are
included.12,39,40
The fact that most of these susceptibility factors have
been identifiedin other autoimmune diseases support the
existence of genetic overlapping between SSc and other
Table3–Epidemiologicaldataandmonitoringindexinpatientswithorwithoutpolyautoimmunity.
Variable Polyautoimmunity p-Value
Yes(n=26) No(n=34)
Epidemiologicaldata
Age 52.50±2.12 50.18±2.24 0.466
Gender
Male 0(0.0) 1(2.9) 0.378
Female 26(100.0) 33(97.1)
Race
Caucasian 14(53.8) 16(47.1) 0.295
Brown 12(46.2) 15(44.1)
Afro-descendent 0(0.0) 3(8.8)
Diagnosistime
<5years 6(23.1) 10(29.4) 0.053
5–10years 9(34.6) 19(55.9)
>10years 11(42.3) 5(14.7)
Pre-diagnosisFRytime 3.19±1.20 4.12±1.27 0.608
Diseasetimeafterdiagnosis 11.27±1.27 7.76±0.93 0.026a
Clinicalform
Limited 9(34.6) 17(50.0) 0.634
Diffuse 10(38.5) 10(29.4)
Recentonset 3(11.5) 4(11.8)
Overlap 4(15.4) 3(8.8)
Monitoringindexes
sHAQ 0.68±0.08 0.60±0.07 0.492
Severityscale 5.31±0.60 4.53±0.47 0.307
Activityscale 2.31±0.30 2.37±0.22 0.868
Skinscore 13.92±1.39 12.44±1.54 0.491
Theresultsarepresentedasmean±meanstandarderror,orasabsolutefrequency(relativefrequency).
Table4–Epidemiologicaldataandmonitoringindexinpatientswithorwithoutfamilialautoimmunity.
Variable Familialautoimmunity p-Value
Yes(n=31) No(n=29)
Epidemiologicaldata
Age 54.00±2.02 48.17±2.31 0.062a
Gender
Male 1(3.2) 0(0.0) 0.329
Female 30(96.8) 29(100.0)
Race
Caucasian 15(48.4) 15(51.7) 0.741
Brown 15(48.4) 12(41.4)
Afro-descendent 1(3.2) 2(6.9)
Diagnosistime
<5years 9(29.0) 7(24.1) 0.912
5–10years 14(45.2) 14(48.3)
>10years 8(25.8) 8(27.6)
Pre-diagnosisFRytime 3.42±0.99 4.03±1.51 0.731
Diseasetimeafterdiagnosis 9.16±1.22 9.41±1.00 0.874
Clinicalform
Limited 12(38.7) 14(48.3) 0.193
Diffuse 14(45.2) 6(20.7)
Recentonset 3(9.7) 4(13.8)
Overlap 2(6.5) 5(17.2)
Monitoringindexes
sHAQ 0.62±0.07 0.66±0.08 0.682
Severityscale 5.26±0.54 4.45±0.51 0.284
Activityscale 2.60±0.27 2.07±0.21 0.136
Skinscore 14.06±1.59 12.03±1.37 0.341
Theresultsarepresentedasmean±meanstandarderror,orasabsolutefrequency(relativefrequency).
a p-ValueinStudent’sttestorchi-squaredtest.
autoimmune diseases, as well as the concept of shared
autoimmunity.39,40
Asharedautoimmunityseemstobeacriticalcomponent
ofthegeneticbasisofautoimmunediseases.39,42,43
Polymor-phismsinmajorhistocompatibilitycomplex(HLA)havealso
beenlinkedtonumerousautoimmunediseasessuchasRA,
spondyloarthritis,andSLE,39,40,43beingofparticularinterest
thehighfrequencyofHLA-DQA1*0501inmenwithSSc.40
Atfirst,itwasbelievedthatsclerodermaorsystemic
scle-rosisfamilialgroupingwasanuncommonevent.44However,
subsequentlyitwasdemonstrated1.6%ofrecurrenceof
sys-temicsclerosisinfamiliesofSScpatientsversusanestimated
risk ofonly 0.026% in the generalpopulation.45 Currently,
itissuggestedthatapositivefamilyhistoryisthegreatest
riskfactoreveridentifiedfordevelopmentofSScinagiven
individual.8,12,40
Likewise,itiswell knownthe highincidenceofoverlap
syndromes in SSc patients, represented by an association
withinflammatorymyopathies,Sjögren’ssyndrome,
rheuma-toid arthritis, and systemic lupus erythematosus in these
patients.38,43,46–48
This study confirms the high frequency of
polyautoim-munity (43.3%) and familial autoimmunity (51.7%) in SSc
patientslivingintheBrazilianMidwest region.Caramaschi
et al.35 found, among 118SSc patients, 32.2% with oneor
twoconcomitantautoimmunediseases,withatotalof42
dif-ferentdiagnoses.Inalargersample,astudyof719patients
fromCanadaandColombia,itsauthorsfound38%of
polyau-toimmunity and 36% of autoimmunity in SSc patients,12
but onlyfirst-degree relatives of these patients were
eval-uated, which could explain the divergence between the
Canadian/Colombianstudyandours.
Amorerecentstudyfound,among121of373(32.4%)
fam-iliesofSSCpatients,atleastoneautoimmunediseaseinone
ormorefirst-degreerelatives.39 Itislikelythatthe
percent-ageoffamilialautoimmunity,muchhigheronourpopulation
comparedtootherstudies,isduetothefactthatwedecided
toextendoursearchalsoforancestors,descendantsand
col-lateralstothethirddegreeofkinship.
Inour study,themainautoimmune diseasesassociated
withSScpatientswereinagreementwiththeliterature,being
mainlyrepresentedbyautoimmunethyroiditis,Sjögren’s
syn-drome, and inflammatory myopathies.12,35,38,46–48 However,
wefoundalower prevalenceofrheumatoidarthritisinour
patients, comparedtoother studies.Probablythisoccurred
becausewehaveadoptedastrictercriterionforthediagnosis
ofanactualoverlapwithrheumatoidarthritiswiththeuse
ofACR/EULAR17classificationcriteriaforRA,plusthe
com-pulsorypresenceofanti-cycliccitrullinatedpeptideantibody
(anti-CCP)and/oroftypicalradiologicalmanifestationsofthe
disease.
Astofamilialautoimmunity,ourdatawereconsistentwith
thosepublishedintheliterature,representedbythe
Table5–Autoantibodiesinpatientswithorwithout polyautoimmunity.
Variable Polyautoimmunity p-Value
Yes(n=26) No(n=34)
Familialautoimmunity
Yes 15(57.7) 16(47.1) 0.414
No 11(42.3) 18(52.9)
Anti-Ro
Positive 6(23.1) 1(2.9) 0.016a
Anti-La
Positive 1(3.8) 0(0.0) 0.249
Anti-Sm
Positive 0(0.0) 1(2.9) 0.378
Anti-RNP
Positive 5(19.2) 5(14.7) 0.641
Anti-Jo1
Positive 0(0.0) 2(5.9) 0.208
Anti-SCL70
Positive 10(38.5) 6(17.6) 0.071
Anti-centromere
Positive 9(34.6) 16(47.1) 0.333
Anti-RNAPol3
Positive 4(15.4) 3(8.8) 0.433
The results are presented as absolute frequency (relative frequency).
a p-Valueinchi-squaredtest.
Table6–Autoantibodiesinpatientswithorwithout familialautoimmunity.
Variable Familialautoimmunity p-Value
Yes(n=31) No(n=29)
Anti-Ro
Positive 4(12.9) 3(10.3) 0.758
Anti-La
Positive 1(3.2) 0(0.0) 0.329
Anti-Sm
Positive 0(0.0) 1(3.4) 0.297
Anti-RNP
Positive 6(19.4) 4(13.8) 0.563
Anti-Jo1
Positive 1(3.2) 1(3.4) 0.962
Anti-SCL70
Positive 9(29.0) 7(24.1) 0.668
Anti-centromere
Positive 9(29.0) 16(55.2) 0.040a
Anti-RNAPol3
Positive 4(12.9) 3(10.3) 0.758
The results are presented as absolute frequency (relative frequency).
a p-Valueinchi-squaredtest.
relatives.36,39,42,43Koumakisetal.foundthatthyroid
autoim-munediseaseandconnectivetissuediseases(SSc,SLE,SS,RA)
weremorecommoninfamiliesofSScpatientsthaninfamilies
inthecontrolgroup.39
Withregard toepidemiologicaldata, theonlydifference
foundinthegroupofpolyautoimmunitypatientswasalonger
duration ofthe diseaseafterdiagnosis.Themostplausible
explanationforthisfindingwouldbeadiagnosisthatoccurred
earlierinthesecarrierswithmorethananautoimmune
dis-ease,contributingtotheirdevelopmentandsurvival.Recently,
another Brazilianstudy conductedbySkare49 stressed that
theknowledgeofthecoexistenceofautoimmunediseasesis
vitally importantforthecorrectdiagnosis ofother
autoim-munediseasesinSScpatients.
Wewouldexpecttofindalowerqualityoflife,oragreater
severity/disease activity in polyautoimmunitypatients, but
thisresultdidnotcometrue.Actually,theliteraturedescribes
theinverse.Avouacetal.,50forinstance,foundamilderform
ofthediseaseinpatientswiththelimitedformofSSc,and
an association withpolyautoimmunity. Caramaschiet al.35
emphasizethattheseverityofSScappearstobeariskfactor
fordevelopmentofanadditionalautoimmunedisease.
However,wepointoutthat, inSScpatientsand
polyau-toimmunity, there is a likelihood of clinically significant
differenceswhenonesetapartaparticularsubgroupof
asso-ciatedcomorbidities.Forexample,arecentBrazilianSouthern
regionalstudyfoundahigherfrequencyofpulmonary
hyper-tension(PH)andatrendofinterstitiallungdiseaseinagroup
of SSc patients inassociation with Hashimoto’sthyroiditis
(HT),whencomparedtopatientswithoutHT.49Taking into
accountthe6casesofPHobservedinourSScpatients,we
also foundahigher prevalenceofPH inthose showingan
associationwithHT(n=4–66.67%)versuspatientswithoutHT
(unpublisheddata).
Thesepatientswerepredominantlyaffectedbythelimited
formofthe disease (57.0%versus34.6%) andexhibited
sig-nificant featuresofvasculardisease,suchastheincreased
occurrenceofanobjectiveRaynaud’sphenomenon(92.6%
ver-sus66.7%)andtelangiectasia(85.7%versus68.3%).Ourpatients
withSScandHThadahigherincidenceofpulmonary
fibro-sis,butthisfindingdidnotreachstatisticalsignificance(57.1%
versus45.0%).
Moreover,alargestudyof24,728patientsand55,632
con-trolsfoundapositiveassociationbetweenhistoryofpersonal
andfamilialautoimmunediseasewithriskofnon-Hodgkin’s
lymphomadevelopment,anditsauthorssuggestedthatthe
sharedsusceptibilitycanonlyexplainasmallfractionofthis
increase.37
Inthisstudy,theobservationofanincreasedfrequencyof
anti-RoinpatientswithSScandpolyautoimmunityiseasily
explained,becausethepositivitytothisantibodywas
associ-atedwithSjögren’ssyndrome,averyprevalentconditionin
thisgroupofpatients.Ontheotherhand,theobservationof
alowerfrequencyofanticentromereinpatientswithfamilial
autoimmunitywasduetothefactthatthisgroupofpatients
wasprimarilypresentingthediffuseformofthedisease,once
againwithoutreachingstatisticalsignificance.Thepatients
showingpolyautoimmunityandfamilialautoimmunitywere
primarilycarriersofthediffuseformofSSc,butthisindicator
A peculiarity of the city of Campo Grande–MS is that
itspopulationisbasicallycomposedofnationalandforeign
immigrants, who came predominantly from the states of
MinasGerais,RioGrandedoSul,ParanaandSaoPaulo;and
fromcountrieslikeGermany,Spain,Italy,Japan,Paraguay,
Por-tugal,SyriaandLebanon.
Themainlimitationofthisstudywasthesmallsampleof
SScpatients;butwiththisstrategy,weseektoeliminatethe
mainbiasobservedinlargestudiesofcoexistenceof
autoim-munediseases,inwhichthefamilialautoimmunityhistory
wasprovidedbythe patient, without anindependent
con-firmation, or amedical record review.All our SSc patients
areaccompaniedbythesame physician,someofthem for
almost10years;andalltheirfamilyand alargenumberof
SScpatients’relativesarefollowedinotheroutpatientclinics
atFMUFMS.
It is worth emphasizing the importance of the shared
autoimmunity concept, in order to promote a continuous
surveillanceofSScpatients;itisexpectedthatinthisscenario
thedoctorisabletoestablishatimelydiagnosisofpossible
secondorthirdassociatedautoimmunedisease,orevenan
autoimmunediseasethatisaffectingthepatient’srelatives.
Conclusions
OurSScpatientshadafrequencyof43.3%of
polyautoimmu-nityand51.7%offamiliarautoimmunity.
The autoimmune diseases most frequently observed
in polyautoimmunity patients were: Hashimoto’s
thyroidi-tis (53.8%), Sjögren’s syndrome (38.5%), and inflammatory
myopathy(11.5%).Themainautoimmunediseasesobserved
in of SSc patients’ relatives were: Hashimoto’s thyroiditis
(32.3%), rheumatoid arthritis (22.6%), and SLE(22.6%). The
presence of more than one autoimmune disease in SSc
patientsdidnotcorrelatewithdiseaseseverityoractivity.
Conflict
of
interests
Theauthorsdeclarenoconflictofinterests.
r
e
f
e
r
e
n
c
e
s
1. VargaJ,AbrahamD.Systemicsclerosis:aprototypic
multisystemfibroticdisorder.JClinInvest.2007;117(3):557–67.
2. HerrickAL,WorthingtonJ.Geneticepidemiology:systemic sclerosis.ArthritisRes.2002;4(3):165–8.
3. GeyerM,Müller-LadnerU.Thepathogenesisofsystemic sclerosisrevisited.ClinRevAllergImmunol.2011;40(3):92–103.
4. MedaF,FolciM,BaccarelliA,SelmiC.Theepigeneticsof autoimmunity.CellMolImmunol.2011;8(3):226–36.
5. BriggsD,WelshKI.MajorhistocompatibilitycomplexclassII genesandsystemicsclerosis.AnnRheumDis.1991;50:862–5.
6. ReesRB,BennettJ.Localizedsclerodermainfatherand daughter.AMAArchDermSyphilol.1953;68(3):360.
7. BarnettAJ,McNeilageLJ.Antinuclearantibodiesinpatients withscleroderma(systemicsclerosis)andintheirblood relativesandspouses.AnnRheumDis.1993;52:365–8.
8. MayersMD,TrojanowskaM.Geneticfactorsinsystemic sclerosis.ArthritisResTher.2007;9Suppl2:S5.
9.RomanoE,ManettiM,GuiducciS,CeccarelliC,AllanoreY, Matucci-CerinicM.Thegeneticsofsystemicsclerosis:an update.ClinExpRheumatol.2011;29(65):S75–86.
10.Arora-SinghRK,AssassiS,JuncoDJ,ArnettFC,PerryM,Irfan U,etal.Autoimmunediseasesandautoantibodiesinthefirst degreerelativesofpatientswithsystemicsclerosis.J Autoimmun.2010;35(1):52–7.
11.AnayaJM,GómezLM,CastiblancoJ.Isthereacommon geneticbasisforautoimmunediseases?ClinDevImmunol. 2006;13(2-4):185–95.
12.HudsonM,Rojas-VillarragaA,Coral-AlvaradoP, López-GuzmánS,MantillaRD,ChalemP,etal.
Polyautoimmunityandfamilialautoimmunityinsystemic sclerosis.JAutoimm.2008;31:156–9.
13.HoogenF,KhannaD,FransenJ,JohnsonSR,BaronM,Tyndall A,etal.2013classificationcriteriaforsystemicsclerosis:an Americancollegeofrhematology/Europeanleagueagainst rheumatismcollaborativeinitiative.AnnRheumDis. 2013;72:1747–55.
14.LeRoyEC,MedsgerTAJr.Criteriafortheclassificationofearly systemicsclerosis.JRheumatol.2001;28(7):1573–6.
15.PetriM,OrbaiAM,AlarcónGS,GordonC,MerrillJT,FortinPR, etal.Derivationandvalidationofthesystemiclupus internationalcollaboratingclinicsclassificationcriteriafor systemiclupuserythematosus.ArthritisRheum.
2012;64(8):2677–86.
16.ShiboskiSC,ShiboskiLH,CriswellLA,BaerAN,Challacombe S,LanfranchiH,etal.AmericanCollegeofRheumatology ClassificationcriteriaforSjögren’ssyndrome:adata-driven, expertconsensusapproachintheSjögren’sInternational CollaborativeClinicalAllianceCohort.ArthritisCareRes. 2012;64(4):475–87.
17.AletahaD,NeogiT,SilmanAJ,FunovitsJ,FelsonDT,Bingham COIII,etal.2010RheumatoidArthritisclassificationcriteria. AnAmericanCollegeofRheumatology/EuropeanLeague AgainstRheumatismcollaborativeinitiative.Arthritis Rheum.2010;62(9):2569–81.
18.SampaioSAP,RivittiEA.Dermatologia.3ed.SãoPaulo:Artes Médicas;2007.p.231–56.
19.RudwaleitM,vanderHeijdeD,LandewéR,AkkocN,BrandtJ, ChouCT,etal.TheassessmentofSpondyloArthritis InternationalSocietyclassificationcriteriaforperipheral spondyloarthritisandforspondyloarthritisingeneral.Ann RheumDis.2011;70(1):25–31.
20.HanauerSB,SandbornW.Thepracticeparameters CommitteeofTheAmericanCollegeofGastroenterology. ManagementofCrohn’sdiseaseinadults.AmJGastroenterol. 2001;96:635–43.
21.MiyakisS,LockshinMD,AtsumiT,BranchDW,BreyRL, CerveraR,etal.Internationalconsensusstatementonan updatetotheclassificationfordefiniteantiphospholipid syndrome(APS).JThrombHaemost.2006;4:
295–306.
22.DeGrootLJ,LarsenPR,HennemanG.Hashimoto’sthyroiditis. In:TheThyroidandIt’sDiseases.6thed.NewYork:Churchill Livingstone;1996.p.307–22.
23.AmericanDiabetesAssociation.Standardsofmedicalcarein diabetes.DiabetesCare.2010;33:11–61.
24.Alarcon-SegoviaD,CardielMH.Comparisonbetween3 diagnosticcriteriaformixedconnectivetissuedisease.Study of593patients.JRheumatol.1989;16:328–34.
25.BohanA,PeterJB.Polymyositisanddermatomyositis(firstof twoparts).NEnglJMed.1975;292:344–7.
27.MedsgerTAJr.Naturalhistoryofsystemicsclerosisandthe assessmentofdiseaseactivity,severity,functionalstatus,and psychologicwell-being.RheumDisClinNAm.2003;29:255–73.
28.ValentiniG,SilmanAJ,VealeD.Assessmentofdisease activity.ClinExpRheumatol.2003;21:39–41.
29.RannouF,PoiraudeauS,BereznéA,BaubetT,Le-GuernV, CabaneJ,etal.Assessingdisabilityandqualityoflifein systemicsclerosis:constructvaliditiesoftheCochinhand functionscale,healthassessmentquestionnaire(HAQ), systemicsclerosisHAQ,andmedicaloutcomesstudy36-item shortformhealthsurvey.ArthritisRheum.2007;57(1):94–102.
30.DellavanceA,GabrielAJr,CintraAFU,XimenesAC,Nuccitelli B,TabilertiBH,etal.IIConsensoBrasileirodeFator
AntinuclearemcélulasHep-2.RevBrasReumatol. 2003;43(3):129–40.
31.McClainMT,RamslandPA,KaufmanKM.Anti-Sm
autoantibodiesinsystemiclupustargethighlybasicsurface structuresofcomplexedspliceosomalautoantigens.J Immunol.2002;168:2054–62.
32.SatoS,HamaguchiY,HasegawaM,TakeharaK.Clinical significanceofanti-topoisomeraseIantibodylevels determinedbyELISAinsystemicsclerosis.Rheumatology. 2001;40:1135–40.
33.CodulloV,MorozziG,BardoniA,SalviniR,DeleonardiG,Pità O,etal.Validationofanewimmunoenzymaticmethodto detectantibodiestoRNApolymeraseIIIinsystemicsclerosis. ClinExpRheumatol.2007;25:373–7.
34.ShapiraY,Agmon-LevinN,ShoenfeldY.Geoepidemiologyof autoimmunerheumaticdiseases.NatRevRheumatol. 2010;6:468–76.
35.CaramaschiP,BiasiD,VolpeA,CarlettoA,CecchettoM, BambaraLM.Coexistenceofsystemicsclerosiswithother autoimmunediseases.RheumatolInt.2007;27:407–10.
36.TanakaA,IgarashiM,KakinumaM,Oh-iT,KogaM,OkudaT. Theoccurrenceofvariouscollagendiseasesinonefamily:a sisterwithLSSc,PBC,APS,andSSandabrotherwith systemiclupuserythematosus.JDermatol.2001;28:547–53.
37.MellemkjaerL,PfeifferRM,EngelsEA,GridleyG,WheelerW, HemminkiK,etal.Autoimmunediseaseinindividualsand closefamilymembersandsusceptibilitytonon-Hodgkin’s lymphoma.ArthritisRheum.2008;58(3):657–66.
38.PakozdiA,NihtyanovaS,MoinzadehP,OngVH,BlackCM, DentonCP.Clinicalandserologicalhallmarksofsystemic sclerosisoverlapsyndromes.JRheumatol.2011;38:2406–9.
39.KoumakisE,DieudeP,AvouacJ,KahanA,AllanoreY. AssociationdesSclérodermiquesdeFrance.Familial autoimmunityinsystemicsclerosis–resultsofa French-basedcase–controlfamilystudy.JRheumatol. 2012;39:532–8.
40.AgarwalSK,TanFK,ArnettFC.Geneticsandgenomicstudies inscleroderma(systemicsclerosis).RheumDisClinNAm. 2008;34:17–40.
41.ZimmermannAF,PizzichiniMMM.Atualizac¸ãona etiopatogênesedaesclerosesistêmica.RevBrasReumatol. 2013;53(6):516–24.
42.AnayaJM,TobonGJ,VegaP,CastiblancoJ.Autoimmune diseaseaggregationinfamilieswithprimarySjögren’s syndrome.JRheumatol.2006;33:2227–34.
43.JawaheerD,SeldinMF,AmosCI,ChenWV,ShigetaR, MonteiroJ,etal.Agenomewidescreeninmultiplex rheumatoidarthritisfamiliessuggestsgeneticoverlapwith otherautoimmunediseases.AmJHumGenet.2001;68:927–36.
44.McGregorAR,WatsonA,YunisE.Familialclusteringof sclerodermaspectrumdisease.AmJMed.1988;84(6):1023–32.
45.ArnettFC,ChoM,ChatterjeeS.Familialoccurrence frequenciesandrelativerisksforsystemicsclerosis (scleroderma)inthreeUnitedStatescohorts.Arthritis Rheum.2001;44(6):1359–62.
46.BaldiniC,MoscaM,DellaRossaA,PepeP,NotarstefanoC, FerroF,etal.OverlapofACA-positivesystemicsclerosisand Sjögren’ssyndrome:adistinctclinicalentitywithmildorgan involvementbutathighriskoflymphoma.ClinExp Rheumatol.2013;31:272–80.
47.NakamuraT,HigashiS,TomodaK,TsukanoM,SugiK. Primarybiliarycirrhosis(PBC)-CRESToverlapsyndromewith coexistenceofSjögren’ssyndromeandthyroiddysfunction. ClinRheumatol.2007;26:596–600.
48.Balbir-GurmanA,Braun-MoscoviciY.Sclerodermaoverlap syndrome.IMAJ.2011;13:14–20.
49.CostaCCB,MedeirosM,WatanabeK,MartinP,SkareTL. TireoiditedeHashimotopodeestarassociadaaumsubgrupo depacientesdeesclerosesistêmicacomhipertensão pulmonary.RevBrasReumatol.2014;54(5):366–70.