w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Low
vitamin
D
serum
levels
in
diffuse
systemic
sclerosis:
a
correlation
with
worst
quality
of
life
and
severe
capillaroscopic
findings
Marília
M.
Sampaio-Barros,
Liliam
Takayama,
Percival
D.
Sampaio-Barros,
Eloísa
Bonfá,
Rosa
Maria
R.
Pereira
∗DivisionofRheumatology,FaculdadedeMedicina,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received6August2015 Accepted11March2016 Availableonline2June2016
Keywords:
Systemicsclerosis VitaminD Qualityoflife
Nailfoldcapillaroscopy
a
b
s
t
r
a
c
t
Objective:TheaimofthisstudywastoanalyzethecorrelationofvitaminDlevelswith clini-calparameters,bonemineraldensity(BMD),qualityoflife(QoL)andnailfoldcapillaroscopy (NC)inpatientswithdiffusesystemicsclerosis(SSc).
Methods:Thirty-eight female patients with diffuse SSc were analyzed regarding 25-hydroxyvitaminD(25OHD)serumlevels.Atinclusion,organinvolvement,autoantibodies, modifiedRodnanskinscore(mRSS),MedsgerDiseaseSeverityIndex(MDSI), bodymass index(BMI),BMD,NC,Short-Form-36Questionnaire(SF-36),andHealthAssessment Ques-tionnaire(HAQ),wereperformedthroughastandardizedinterview,physicalexamination andelectronicchartreview.
Results:Mean25OHDserumlevelwas20.66±8.20ng/mL.Elevenpercentofthepatients had25OHDlevels≤10ng/mL,50%≤20ng/mLand87%≤30ng/mL.VitaminDserumlevels werepositivelycorrelatedwithBMI(r=0.338,p=0.038),BMD-totalfemur(r=0.340,p=0.037), BMD-femoralneck(r=0.384,p=0.017),SF-36-Vitality(r=0.385,p=0.017),SF-36-Social Func-tion(r=0.320,p=0.050),SF-36-EmotionalRole(r=0.321,p=0.049)andSF-36-MentalHealth (r=0.531,p=0.0006)andwerenegativelycorrelatedwithHAQ-Reach(r=−0.328,p=0.044) andHAQ-GripStrength(r=−0.331,p=0.042).AnegativecorrelationwithNC-diffuse devas-cularization(p=0.029)andNC-avasculararea(p=0.033)wasalsoobserved.
Conclusion: Thepresentstudyprovidesnovelevidencedemonstratingthatlowlevelsof 25OHDhaveanegativeimpactindiffuseSScQoLandfurtherstudiesareneededtodefine whethervitaminDsupplementationcanimprovehealthrelatedQoLinthesepatients.The additionalobservationofacorrelationwithsevereNCalterationssuggestsapossiblerole of25OHDintheunderlyingSScvascularinvolvement.
©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](R.M.R.Pereira).
http://dx.doi.org/10.1016/j.rbre.2016.05.006
Baixos
níveis
séricos
de
vitamina
D
na
esclerose
sistêmica
difusa:
correlac¸ão
com
pior
qualidade
de
vida
e
alterac¸ões
capilaroscópicas
graves
Palavras-chave:
Esclerosesistêmica VitaminaD Qualidadedevida
Capilaroscopiaperiungueal
r
e
s
u
m
o
Objetivo: Oobjetivodesteestudofoianalisaracorrelac¸ãoentreosníveisdevitaminaD eparâmetrosclínicos,densidademineralóssea(DMO),qualidadedevida(QV)e capilaro-scopiaperiungueal(CPU)empacientescomesclerosesistêmicadifusa(ES).
Métodos:Mensuraram-seosníveisséricosde25-hidroxivitaminaD(25OHD)de38pacientes dosexofemininocomESdifusa.Nomomentodainclusão,analisaram-seoenvolvimento deórgãos,autoanticorpos,escorecutâneodeRodnanmodificado(ERM),MedsgerDisease SeverityIndex (MDSI),índicedemassacorporal (IMC),DMO,CPU,Short-Form-36 Ques-tionnaire(SF-36)eHealthAssessmentQuestionnaire(HAQ)pormeiodeumaentrevista padronizada,examefísicoeavaliac¸ãodeprontuárioeletrônico.
Resultados: Amédiadonívelséricode25OHDfoide20,66±8,20ng/mL.Dospacientes,11% tinhamníveisde25OHD≤10ng/mL,50%≤20ng/mLe87%≤30ng/mL.Osníveisséricosde vitaminaDestiverampositivamentecorrelacionadoscomoIMC(r=0,338,p=0,038), DMO-fêmur total (r=0,340, p=0,037),DMO-colo femoral(r=0,384, p=0,017), SF-36-Vitalidade (r=0,385, p=0,017), SF-36-Aspecto social (r=0,320, p=0,050), SF-36-Aspecto emocional (r=0,321,p=0,049)eSF-36-Saúdemental(r=0,531,p=0,0006)esecorrelacionaram neg-ativamentecomoHAQ-Alcance(r=−0,328,p=0,044)eHAQ-forc¸adepreensão(r=−0,331, p=0,042).Tambémfoiobservadaumacorrelac¸ãonegativacomaCPU-desvascularizac¸ão difusa(p=0,029)eCPU-áreaavascular(p=0,033).
Conclusão: Opresenteestudofornece evidênciasnovasdequeníveisbaixosde25OHD têmumimpactonegativosobreaqualidadedevidadepacientescomESdifusaeque sãonecessáriosmaisestudosparadefinirseasuplementac¸ãodevitaminaDpode melho-raraqualidadedevidarelacionadacomasaúdedessespacientes.Aobservac¸ãoadicional deumacorrelac¸ãocomalterac¸õesgravesnaCPUsugereumpossívelpapelda25OHDno envolvimentovascularsubjacentedaES.
©2016ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Significance
&
innovations
1) LowvitaminDserumlevelshadanegativeimpacton phys-icalandemotionaldomainsofqualityoflifeindiffuseSSc patients.
2) LowvitaminDserum levelswerecorrelated withsevere capillaroscopicfindings.
3) LowervitaminDlevelsweremorefrequentlyobservedin patientswithanti-Scl70positive.
Introduction
Inthelasttwodecades,thesurvivalofpatientswithsystemic sclerosis(SSc)hassignificantlyimproved.1,2Nevertheless,SSc
can still cause increased disability and reduced quality of life.Several factors can beinvolved withthese conditions, asdisease subtype,3 gender,4 lung involvement,3 pruritus,5
fatigue,6 anxietyand depression.7,8 Hand,tendonandjoint
involvementare other factors which can cause significant functionaldisability,leadingtoconsequentdisuseand wors-eningofbonelossinpatientswithSSc,9,10 contributingtoa
significantimpairmentinthequalityoflifeofthesepatients.10
Low levels of 25-hydroxyvitamin D (25OHD) may also contribute to the chronic inflammation, immunological dysregulation and skeletal myopathy with a consequent reductioninqualityoflifeinautoimmunediseases.11,12
Stud-iesevaluatingvitaminDlevelsinSScpatientsrevealedahigh frequencyofthisconditionandapossibleassociationwith inflammation and pulmonaryhypertension.13–18 There are,
however,nodataregardinglowvitaminDimpactinquality oflifeinthesepatients.
Theaimofthisstudywastherefore,toanalyzethe correla-tionofvitaminDwithqualityoflife,clinicalparametersand nailfoldcapillaroscopy(NC)inpatientswithdiffuseSSc.
Methods
Patients
This is a cross-sectional study analyzing 38 diffuse SSc patientswhoattendedtheSclerodermaOutpatientClinicof the University of São Paulo from May 2012 to May 2013. All patients were classified as SSc according to the recent EULAR/ACRcriteria.19Inclusioncriteriawerefemalegender;
theinformedconsent.Exclusioncriteriaincluded:diagnosisof anotherconnectivetissuedisease(CTD),organfailure(renal, pulmonaryorcardiac),gastricsurgery,intestinal malabsorp-tion,pregnancy,breast-feeding,severe infection andsevere chroniccomorbidities.
Clinicaldata
Clinical and demographic data were obtained through a direct interview and a review of the electronic register database. Esophageal involvement was considered when patientreferredclinicalcomplaintofdysphagiaandbarium esophagram revealed esophageal hypomotility. Interstitial lung disease was considered when patient presented the characteristic“ground-glass” aspect atthe chest high res-olutioncomputed tomography.Modified Rodnanskinscore (mRSS) was used to determine the extension of the skin involvement,classifying17anatomicalsitesfrom0(noskin involvement)to3 (severeskininvolvement),withmaximal scoreof51.21
MedsgerDiseaseSeverityIndex(MDSI)wasusedto deter-minetheSScseverity,definingseverityasthetotaleffectof diseaseonorganfunction.Scalesweredevelopedfrom0(no documented involvement) to4 (endstagedisease) for each organsystem:general(weightlossinkg),peripheralvascular (digitalvascularischemia),skin(mRSS),joint/tendon,muscle (weakness),gastrointestinaltract,lung,heart,andkidney.22
WeconsideredaseverediseasewhentheMDSIwassuperior to3,accordingtopreviousstudies.16
Qualityoflife
HealthAssessmentQuestionnaire(HAQ)disabilityindex(DI), validatedtotheBrazilian-Portugueselanguage23wasapplied.
Itcontains 8domains of activity (dressing,raising, eating, walking,personal hygiene, reach, grip strength, and usual dailyactivities)eachofwhichhasatleasttwoquestions,fora totalof20items.Foreachitem,patientsreporttheamountof difficultyexperiencedperformingtheactivity.Ameanscore iscalculated foreach domain,rangingfrom0(withoutany difficulty)to3(unabletodo).AcompositeHAQscoreis calcu-latedbydividingthesummeddomainscoresbythenumber ofdomainsanswered.Thecompositescoreisreported,falling between0(noimpairmentinfunction)and3(maximal impair-mentoffunction)onanordinalscale.24
The Short Form Questionnaire (SF-36), validated to the Brazilian-Portugueselanguage,25wasalsoapplied.TheSF-36
consists of 36 items organized into eight health domains measuring physical functioning, role limitations due to physicalproblems,bodily pain, generalhealthperceptions, vitality,socialfunctioning,rolelimitationsduetoemotional aspects,andgeneralmentalhealth.26Amongthesedomains,
physicalfunctioning,physicalrole,andbodilypainevaluate onlyphysicaldimensions;socialfunctioning,emotionalrole, and general mental health assess mentalaspects; general health perception and vitality evaluate both physical and mental dimensions.In SF-36 domains, scoresare ratedso thathighervaluescorrespondtobetterconditionsandlower scorestoworseconditions(range0–100).Theeightdomains, weightedaccordingtonormativedata,arealsocombinedinto
aphysicalsummaryscore(PSS)andamentalsummaryscore (MSS), which are scored from 0 to100, withhigher values reflectingbetterhealth-relatedqualityoflife(HRQOL).27
Nailfoldcapillaroscopy(NC)
Invivowidefieldcapillarymicroscopy(10and20 magnifica-tions)wasperformedandgradedbythesamerheumatologist. All ten digits were examined using a bifocal stereomicro-scope(Zeiss,Germany)andlightingwithatungsteniumlamp shadedbyagreenlens inordertohaveabetter visualiza-tion.Immersionoilwasappliedforincreasingtransparency of the skin and the whole nailfold region was examined, includingthe edges.Thenormalfindings forBrazilian pop-ulation were defined as previously described.28 Abnormal
findings were recorded on a standardized data sheet, as follow: number of loops in a linear 1mm wide, enlarge-mentofcapillaryloops (absolutenumber,independentlyof thesizeofthelimbs),presenceofbushycapillariesandthe avascularareas (lossoftwoconsecutive loops ofnail bed). In this study, it was used the following scores: (1) Diffuse devascularization (mean): 0=normal (≥7loops/mm); 1=mild (≥6to<6.9loops/mm);2=moderate (≥4to<5.9loops/mm); 3=severe (<4loops/mm); (2) Avascular areas: 0=no avascu-larareas;1=1or2discontinuousavascularareas(>0.3mm and <0.5mm); 2=more than two discontinuous avascular areas (>0.3mm and <0.5mm); 3=extense avascular areas (>0.5mm);(3)Capillarectasia: 0=rare(<8capillaries);1=mild (8–30 capillaries); 2=moderate (31–40 capillaries); 3=severe (>40 capillaries); (4) Microhemorrhages: 0=rare (<3/finger); 1=mild(≥3and <6/finger); 2=moderate (≥6and <8/finger); 3=severe (≥8/finger).29 TheSD pattern was defined as the
presence of avascular areas or enlarged loops associated with atleast one additionalSD-parameter (nailfold micro-hemorrhages,reduced capillarydensity,enlargedloops and avascularareas).30
NCwasalsoclassifiedin“early”,“active” and“late” pat-terns,accordingtoCutoloetal.31“Earlypattern”:presenceof
giantcapillarieswithoutlossofcapillaries,“Activepattern”: presenceofcombinationofgiantcapillaries,lossofcapillaries andmicrohemorrhages.“Latepattern”presenceof neoangio-genesisandlossofcapillaries.
Laboratorydata
Blood was collected in the morning, with a 12-h fasting. Serum and plasma were aliquoted and kept at −80◦C on
BoneMetabolismLaboratoryofRheumatologyDivision, Fac-ultyofMedicine.Laboratoryparametersofbonemetabolism weremeasuredinallpatients:calcium,phosphate,alkaline phosphate,parathormone,25OHDserum levelsandurinary calcium.Aradioimmunoassaytechnique(DiaSorin, Stillwa-ter, MN,USA) witha lower detection limit of5ng/mL was used tomeasure 25-hydroxyvitamin D(25OHD). The intra-andinter-assayvariationcoefficientsinourlaboratorywere 10.5% and 17.8%,respectively. Accordingtocurrent recom-mendations,25OHDconcentrations≤30ng/mLweredefined asinsufficiency,32,33whereasvalues≤10ng/mLwereclassified
Theprofile of autoantibodiesfor each patient was also obtained: antinuclear antibodies (ANA), anti-DNA topoiso-meraseI(anti-Scl70).
Bonemineraldensity
BMDwasanalyzedbydual-energyX-rayabsorptiometry(DXA; Hologic;QDR4500,Bedford,MA, USA)ofthelumbarregion (L1-L4),totalandfemoralneck.Osteoporosiswasdefinedby aT score≤−2.5SD. Bodymassindex (BMI) wascalculated bymeasuringtheweightand heightofeachpatientduring interview.
Ethicalapproval
Allpatientsgavetheirwritteninformedconsentandthestudy wasapprovedbytheEthicsCommitteeoftheUniversityofSão Paulo(Researchprotocol0294/11).
Statisticalanalysis
The results are reported as mean±standard deviation and percentage. The data were analyzed by t-test or Mann–Whitney test to access the differences between the groups.Prismprogram softwarewasusedto correlationof Pearson;pvalues≤0.05wereconsideredtobesignificant.
Results
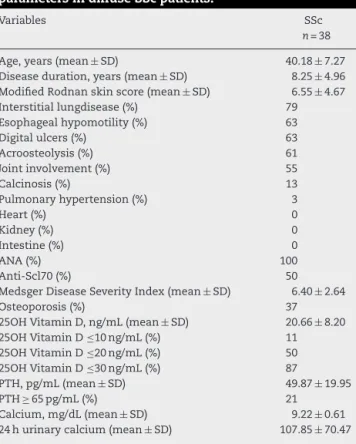
Thirty-eightfemalepatientswithdiffuseSScattendingthe Sclerodermaoutpatientclinicofourinstitutionwereeligible toparticipateinthis study.Themean agewas 40.18±7.27 years,and themean diseaseduration was8.25±4.96years (Table1).Sixteenpatients(42%)werecurrentlyusingmonthly doses of intravenous cyclophosphamide, while 18 (47%) patientsreferredprevioususe,andfour(11%)hadneverused it.Among the 18 patients who previouslyused cyclophos-phamide,15(39%)werecurrentlyusingazathioprineandthree (8%)wereusingmycophenolatemofetil.Sixteenpatients(42%) alsoreferredprevioususeofmethotrexate.
Amongthe clinical manifestations, interstitiallung dis-ease(79%),esophagealhypomotility(63%),digitalulcers(63%) and joint involvement(55%) were the most frequent find-ings.Hand deformitieswere observed in 21 patients (55%) andsubcutaneouscalcinosisin5patients(13%).Other clin-icalmanifestationsofSScwerepresentin<5%ofthepatients. MeanmRSSwas6.55±4.67,andmeanMDSIwas6.40±2.64 (Table1).
Osteoporosis (total femur, femoral neck and/or lumbar spine)wasfound in37% ofthediffuseSSc patients. Mean 25OHDserum levels were 20.66±8.20ng/mL. Four patients (11%)hadlevelsof25OHD≤10ng/mL,19patients(50%)had
≤20ng/mLand33patients(87%)had≤30ng/mL(Table1). FurtheranalysisofvitaminDlevelsinpatientswithand withoutesophagealinvolvement(20.40±8.23vs.21.12±8.43,
p=0.80),interstitiallungdisease(19.76±7.90vs.24.05±8.93,
p=0.19), digitalulcers (20.63±8.28 vs. 20.71±8.36,p=0.98), hand deformities (18.70±8.33 vs. 23.09±7.57, p=0.10), jointinvolvement(19.40±7.74vs. 22.23±8.71,p=0.30),and
Table1–Anthropometric,clinical,andlaboratory parametersindiffuseSScpatients.
Variables SSc
n=38
Age,years(mean± SD) 40.18± 7.27
Diseaseduration,years(mean± SD) 8.25± 4.96 ModifiedRodnanskinscore(mean ± SD) 6.55± 4.67
Interstitiallungdisease(%) 79
Esophagealhypomotility(%) 63
Digitalulcers(%) 63
Acroosteolysis(%) 61
Jointinvolvement(%) 55
Calcinosis(%) 13
Pulmonaryhypertension(%) 3
Heart(%) 0
Kidney(%) 0
Intestine(%) 0
ANA(%) 100
Anti-Scl70(%) 50
MedsgerDiseaseSeverityIndex(mean ± SD) 6.40± 2.64
Osteoporosis(%) 37
25OHVitaminD,ng/mL(mean± SD) 20.66± 8.20
25OHVitaminD≤10ng/mL(%) 11
25OHVitaminD≤20ng/mL(%) 50
25OHVitaminD≤30ng/mL(%) 87
PTH,pg/mL(mean± SD) 49.87± 19.95
PTH≥ 65pg/mL(%) 21
Calcium,mg/dL(mean ± SD) 9.22± 0.61 24hurinarycalcium(mean± SD) 107.85± 70.47
ANA,antinuclearantibody;SD,standarddeviation.
calcinosis (17.40±9.61 vs. 21.16±8.02, p=0.35) revealed no associationoflowerserumlevelsofthishormoneandthe dif-ferentclinicalmanifestations.Nevertheless,anti-Scl70 posi-tivepatientspresentedlowerlevelsofvitaminDcomparedto anti-Scl70negative(17.94±7.10vs.23.40±8.49,p=0.039).
ThepossiblecorrelationsofvitaminDwithdemographic, bone mineraldensity and nailfoldcapillaroscopy data was performed and revealed a positivecorrelation with weight (r=0.333;p=0.041),BMI(r=0.338;p=0.038),totalfemurBMD (r=0.340;p=0.037),femoralneckBMD(r=0.384;p=0.017)and fat mass (r=0.323; p=0.048). No correlation was observed between25OHDwithage,diseaseduration,mRSSandMDSI (Table2).
All the patients presented the characteristic “SD pat-tern” and the mean NC score was 5.50±2.29. The mean scoresforcapillaroscopiccharacteristicswere:diffuse devas-cularization=1.71±0.73; avascular areas=1.92±0.88; capil-laryectasia=0.42±0.76;andmicrohemorrhages=0.45±0.92. Eighteen (47%) patients presented “active pattern” and 20 (53%) “late pattern” in NC. There was negative correlation among 25OHD serum levels and diffuse devascularization (r=−0.355;p=0.029)andavascularareas(r=−0.347;p=0.033) (Table2).
MeanSF-36was53.05±8.71.Theanalysisofthe8domains ofSF-36showedapositivecorrelationamong25OHDserum levels and SF-36-Vitality (r=0.385; p=0.017); SF-36-Social Function (r=0.320; p=0.050); SF-36-MentalHealth (r=0.531;
Table2–Correlationof25OHDwithage,weight,height,bodymassindex(BMI),diseaseduration,bonemineraldensity (BMD),nailfoldcapillaroscopy(NC),MedsgerDiseaseSeverityIndex(MDSI)andModifiedRodnanSkinScore(mRSS)in38 diffuseSScpatients.
25OHD Mean ± SD Pearsonr p-Value
Age,years 40.18± 7.27 0.289 0.079
Weight,kg 63.78± 14.20 0.333 0.041
Height,m 1.58± 0.06 0.149 0.373
BMI,kg/m2 25.49± 4.96 0.338 0.038
Diseaseduration,years 8.25± 4.96 −0.280 0.088
L1–L4BMD,g/cm2 0.917± 0.163 0.239 0.149
TotalfemurBMD,g/cm2 0.795± 0.167 0.340 0.037
FemoralneckBMD,g/cm2 0.710± 0.130 0.384 0.017
DistalradiusBMD,g/cm2 0.516± 0.071 0.272 0.099
Fatmass,g 23.05± 8.17 0.323 0.048
Leanmass,g 38.38± 7.11 0.264 0.109
NC
Diffusedevascularization 1.71± 0.73 −0.355 0.029
Avasculararea 1.92± 0.88 −0.347 0.033
Capillarectasia 0.42± 0.76 0.114 0.498
Microhemorrhages 0.45± 0.92 0.164 0.325
MDSI 6.40± 2.64 −0.277 0.092
mRSS 6.55± 4.67 0.028 0.866
Table3–Correlationof25OHDwithShortFormQuestionnaire(SF-36)andHealthAssessmentQuestionnaire(HAQ)in38 diffuseSScpatients.
25OHD Mean ± SD Pearsonr p-Value
SF-36
Physicalfunctioning 51.58± 27.46 0.270 0.101
Physicalrole 42.76± 42.28 0.074 0.659
Bodilypain 51.80± 27.30 0.245 0.139
Generalhealth 49.40± 25.30 0.309 0.059
Vitality 48.95± 22.73 0.385 0.017
Socialfunction 70.39± 26.22 0.320 0.050
Emotionalrole 48.24± 45.65 0.321 0.049
Mentalhealth 61.26± 16.35 0.531 0.0006
HAQ
Dressing 0.82± 0.77 −0.231 0.164
Raising 0.54± 0.61 −0.293 0.075
Eating 0.58± 0.67 −0.042 0.803
Walking 0.32± 0.47 −0.154 0.356
Hygiene 0.43± 0.53 −0.206 0.214
Reach 1.01± 0.80 −0.328 0.044
Gripstrength 0.88± 0.74 −0.331 0.042
Activities 0.87± 0.73 −0.197 0.235
withHAQ-Reach(r=−0.328;p=0.044)andHAQ-GripStrength (r=−0.331;p=0.042)(Table3).
Discussion
Thisisthe first study identifyingthat vitaminD is signifi-cantlycorrelatedwithQoLandseverecapillaroscopicfindings in diffuse SSc. The decision to focus the analysis on dif-fuseSScandfemalegenderwasimportanttoselectamore homogeneousgroupofpatientsinaheterogeneousdisease as SSc. Consideringthat limited and diffuseSSc subtypes canpresentdistinctprofiles oforgan involvement,20,35 they
couldaffectQoLinadistinctway;infact,diffuseSScpatients
presenthigherglobalandlocaldisability,andlowerQoLthan limitedSSc patients.36 Theinclusionofonlyfemalegender
mayberelevantsinceapossibleassociationofgenderwith diseaseclinicalexpressionandanxietyinpatientswithSSc wasreported.4Infact,arecentcross-sectionalstudyobserved
thatpsychiatricsymptoms,particularlyanxietyand depres-sion,aremoreassociatedwithincreaseddisabilityandaltered health-relatedQoLinSScpatients,thanwithdisease-specific organmanifestations.8Moreover,handdeformity,a
complica-tionwhichisknowntohaveadeleteriouseffectindisability andreducedhealth-relatedQoLinSSc,36isreportedtohavea
positiveassociationwithanti-Scl70antibody.37
diseases,11,12 includingdiffuseSSc.13–18 Althoughtherewas
noassociationwithSSc-specificorganmanifestations,there wasastatisticalassociationwithSSc-specificautoantibody, theanti-Scl70(aknownbiomarkerofdiffuseSSc),which pre-sentedlowerlevelsof25OHD.
Despiterecentstudieshaveclearlyevidencedahigh preva-lence of 25OHD deficiency in SSc, its role has not been completelyunderstoodinSScdiseasepathogenesis.Although it could be advisable to regularly check 25OHD status in these patients, there is no consensus that 25OHD supple-mentation might be sufficient to modulate immunological homeostasis,andreducediseaseactivityorseverity.13,14
Sev-eral studies about lower serum 25OHD concentrations are linkedwith variousclinical aspects inSSc patients. In our study,thepresenceofosteoporosis/osteopeniawasfrequent inourpatientsandthepositivecorrelationbetween25OHD and total femurand femoralneck BMDwas alsofound in the literature, but there is no clear demonstration about therelationshipof25OHDdeficiencywithlowbonemineral density.15,17,38
AsvitaminDsupplementationwasnotaroutinepractice fortheOutpatientSclerodermaClinicbefore thisstudy,no sclerodermapatientwaspreviouslysupplementedwith vita-minD.
Importantly,themaincausesofvitaminDdeficiency,such asintestinalmalabsorption,gastrectomy,kidneyandliver fail-ure, were exclusion criteria forthis study.As inBrazil the seasonsarenotclearlydemonstratedastheyareinEuropean andNorthAmericancountries, thepatientsparticipatingin thisstudy hadtheir clinicalandlaboratoryevaluation con-secutively, from May 2012 to May 2013, regardless of the season.Reducedsunexposureforpsychologicaland social reasonswasnotevaluatedinourstudyandmaycontribute to this deficiency in scleroderma patients.14 Of note, one
fourth ofpatients had high PTH levels, which may reflect secondaryhyperparathyroidismassociatedwithasilent mal-absorption.InlimitedSSc,vitaminDdeficiencywascorrelated withhyperparathyroidismandthelatterwasassociatedwith acroosteolysis.39
Anotherimportantconcernistheinteractionamong vita-minDandthedrugsusedinthelongtermtreatmentofSSc. Someofthesedrugs,likecyclophosphamide,calcium chan-nelblockers(ex.nifedipine)andproton-pumpinhibitors(ex. omeprazol),whicharemetabolizedthroughcytochromeP450 3A4 (CYP3A4),could theoreticallyinterfere with vitaminD metabolism.40However,therearenospecificstudies
analyz-ingitseffectsonbonemetabolisminSSc.
Interestingly,thisisthefirststudytorevealtheimportance ofvitaminDforseveralphysicalandemotionaldomainsof qualityoflifeindiffuseSSc.VitaminDwascorrelatedwith vitality,socialfunction,mentalhealthandemotionalrolein SF-36.Thisfindingisfurthersupportedbytherecent obser-vationincommunity-basedelderlyCanadiansdemonstrating the importanceofthis hormoneinhealthquality oflife.41
ThesignificantcorrelationofvitaminDinSScpatientswith mentalhealthobservedhereinisconsistentwiththe hypoth-esisofarecentsystematicreviewinmorethan30,000adults demonstratingthatlowvitaminDconcentrationisassociated withdepression42andalsowithanxietyinalargecommunity
sample.41
ThenovelcorrelationoflowvitaminDwithHAQreachand gripstrengthdomainsmayberelatedtothefactthatvitaminD improvesmusclestrength,anditssupplementationhasa pos-itiveeffectinmobilityandphysicalfunction.43Infact,higher
levelsareassociatedwithabettermobilityandusual activ-itiesperformance.43Inthisregard,futurestudiesanalyzing
handgripindiffuseSScwillbeinteresting,sincevitaminD statuswas reportedtopredicthand-gripstrength inyoung adultwomen.44
The well-establishedrole ofcapillaroscopy forthe early diagnosisofSSc,anditsinclusionintherecentACR/EULAR classificationcriteria,combinedwithitspotentialfor moni-toringdiseaseprogressionandtreatmentresponse,makesNC animportantassessmentinclinicalpracticeandresearch.31,45
Inthepresentstudy,asmostpatientspresentedlatediffuse SSc,the“active”andthe“late”capillaroscopicpatternswere predominant.Weconfirmedthenegativecorrelationof25OHD serumlevelsandNC–diffusedevascularizationandavascular areas,14althoughnotassociatedwithlunginvolvement.This
findingraisesthehypothesisthatlowlevelsofthishormone maycontributetoendothelialdysfunctioninSSc.Infact,low vitamin D status was associated with arterial dysfunction andvitaminDsupplementationwasreportedtocounteract thisendothelialalterationinasymptomaticsubjectsand dia-betes patients.46,47 Currentevidence indicates thatvitamin
Dsupplementationmayhaveasmalltomoderateeffecton qualityoflifewhenusedonashort-termbasisindiseased populations.However,theevidenceforabeneficialeffectof long-termvitaminDsupplementationonhealth-related qual-ityoflifeislacking.48–50
Thepresentstudyprovidesnovelevidencedemonstrating thatlowlevelsof25OHDcancontributetoadecreasedQoL inpatientswithdiffuseSScthroughitsassociationwiththe underlyingvascularinvolvement(worstcapillaroscopic find-ings)andtheautoantibodyproduction(anti-Scl70).
Funding
Marília M. Sampaio-Barrosisarecipient ofaPost-Doctoral Research Grantfrom the Coordenac¸ão de Aperfeic¸oamento dePessoaldeNívelSuperior(CAPES)/MinistériodaEducac¸ão (MEC). Percival D. Sampaio-Barros, Eloísa Bonfá and Rosa Maria R. Pereira were recipients of a research Grant from FedericoFoundation,SwitzerlandandgrantsfromConselho NacionaldeDesenvolvimentoCientíficoeTecnológico(CNPQ #472754/2013-0toRMRPand#301411/2009-3toEB).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
2. Sampaio-BarrosPD,BortoluzzoAB,MarangoniRG,RochaLF, DelRioAP,SamaraAM,etal.Survival,causesofdeath,and prognosticfactorsinsystemicsclerosis:analysisof947 Brazilianpatients.JRheumatol.2012;39(10):1971–8.
3. SchnitzerM,HudsonM,BaronM,SteeleR,Canadian SclerodermaResearchGroup.Disabilityinsystemicsclerosis –alongitudinalobservationalstudy.JRheumatol.
2011;38(4):685–92.
4. NguyenC,BéreznéA,BaubetT,Mestre-StanislasC,RannouF, PapelardA,etal.Associationofgenderwithclinical
expression,qualityoflife,disability,anddepressionand anxietyinpatientswithsystemicsclerosis.PLoSONE. 2011;6(3):e17551.
5. El-BaalbakiG,RazykovI,HudsonM,BasselM,BaronM, ThombsBD,etal.Associationofprurituswithqualityoflife anddisabilityinsystemicsclerosis.ArthritisCareRes (Hoboken).2010;62(10):1489–95.
6. SandqvistG,SchejaA,HesselstrandR.Pain,fatigueandhand functioncloselycorrelatedtoworkabilityandemployment statusinsystemicsclerosis.Rheumatology(Oxford). 2010;49(9):1739–46.
7. DelRossoA,MikhaylovaS,BacciniM,LupiI,MatucciCerinic M,MaddaliBongiS.Insystemicsclerosis,anxietyand depressionassessedbyhospitalanxietydepressionscaleare independentlyassociatedwithdisabilityandpsychological factors.BioMedResInt.2013;2013:507493.
8. NguyenC,RanqueB,BaubetT,BéreznéA,Mestre-StanislasC, RannouF,etal.Clinical,functionalandhealth-relatedquality oflifecorrelatesofclinicallysignificantsymptomsofanxiety anddepressioninpatientswithsystemicsclerosis:a cross-sectionalsurvey.PLOSONE.2014;9(2):e90484.
9. MouthonL.Handinvolvementinsystemicsclerosis.Presse Med.2013;42(12):1616–26.
10.BasselM,HudsonM,BaronM,TailleferSS,MouthonL, PoiraudeauS,etal.Physicalandoccupationaltherapyreferral anduseamongsystemicsclerosispatientswithimpaired handfunction:resultsfromaCanadiannationalsurvey.Clin ExpRheumatol.2012;30(4):574–7.
11.OrbachH,Zandman-GoddardG,AmitalH,BarakV,Szekanecz Z,SzucsG,etal.Novelbiomarkersinautoimmunediseases: prolactin,ferritin,vitaminD,andTPAlevelsinautoimmune diseases.AnnNYAcadSci.2007;1109:385–400.
12.AnticoA,TampoiaM,TozzoliR,BizzaroN.Can
supplementationwithvitaminDreducetheriskormodify thecourseofautoimmunediseases?Asystematicreviewof theliterature.AutoimmunRev.2012;12(2):127–36.
13.VaccaA,CormierC,MathieuA,KahanA,AllanoreY.Vitamin Dlevelsandpotentialimpactinsystemicsclerosis.ClinExp Rheumatol.2011;29(6):1024–31.
14.CaramaschiP,DallaGassaA,RuzzenenteO,VolpeA, RavagnaniV,TinazziI,etal.VerylowlevelsofvitaminDin systemicsclerosispatients.ClinRheumatol.
2010;29(12):1419–25.
15.ArnsonY,AmitalH,Agmon-LevinN,AlonD,
Sánchez-Casta ˜nónM,López-HoyosM,etal.Serum25-OH vitaminDconcentrationsarelinkedwithvariousclinical aspectsinpatientswithsystemicsclerosis:aretrospective cohortstudyandreviewoftheliterature.AutoimmunRev. 2011;10:490–4.
16.AvouacJ,KoumakisE,TothE,MeunierM,MauryE,KahanA, etal.Increasedriskofosteoporosisandfractureinwomen withsystemicsclerosis:acomparativestudywithrheumatoid arthritis.ArthritisCareRes(Hoboken).2012;64(12):1871–8.
17.Rios-FernándezR,Callejas-RubioJL,Fernández-RoldánC, Simeón-AznarCP,García-HernándezF,Castillo-GarcíaMJ, etal.BonemassandvitaminDinpatientswithsystemic sclerosisfromtwoSpanishregions.ClinExpRheumatol. 2012;30(6):905–11.
18.AtteritanoM,SorbaraS,BagnatoG,MiceliG,SangariD, MorganteS,etal.Bonemineraldensity,boneturnover markersandfracturesinpatientswithsystemicsclerosis:a casecontrolstudy.PLoSONE.2013;8(6):e66991.
19.vandenHoogenF,KhannaD,FransenJ,JohnsonSR,BaronM, TyndallA,etal.2013classificationcriteriaforsystemic sclerosis:anAmericanCollegeofRheumatology/European LeagueagainstRheumatismcollaborativeinitiative.Arthritis Rheum.2013;65(11):2737–47.
20.LeRoyEC,BlackC,FleischmajerR,JablonskaS,KriegT, MedsgerTAJr,etal.Scleroderma(systemicsclerosis): classification,subsetsandpathogenesis.JRheumatol. 1988;15(2):202–5.
21.FurstDE,ClementsPJ,SteenVD,MedsgerTAJr,MasiAT, D’AngeloWA,etal.ThemodifiedRodnanskinscoreisan accuratereflectionofskinbiopsythicknessinsystemic sclerosis.JRheumatol.1998;25(1):84–8.
22.MedsgerTAJr,SilmanAJ,SteenVD,BlackCM,AkessonA, BaconPA,etal.Adiseaseseverityscaleforsystemicsclerosis: developmentandtesting.JRheumatol.1999;26(10):2159–67.
23.FerrazMB,OliveiraLM,AraujoPM,AtraE,TugwellP.Cross culturalreliabilityofthephysicalabilitydimensionofthe healthassessmentquestionnaire.JRheumatol.
1990;17(6):813–7.
24.BruceB,FriesJF.TheStanfordHealthAssessment Questionnaire:areviewofitshistory,issues,progress,and documentation.JRheumatol.2003;30:167–78.
25.CiconelliRM,FerrazMB,SantosWS,MeinãoI,QuaresmaMR. Traduc¸ãoparaalínguaportuguesaevalidac¸ãodo
questionáriogenéricodequalidadedevidaSF-36(Brasil SF-36).BrazJRheumatol.1999;39(3):143–50.
26.WareJEJr,SherbourneCD.TheMOS36-itemshort-form survey(SF-36).I.Conceptualframeworkanditemselection. MedCare.1992;30(6):473–83.
27.DelRossoA,BoldriniM,D’AgostinoD,PlacidiGP,ScarpatoA, PignoneA,etal.Health-relatedqualityoflifeinsystemic sclerosisasmeasuredbytheshortform36:relationshipwith clinicalandbiologicmarkers.ArthritisRheum.
2004;51(3):475–81.
28.AndradeLE,GabrielAJr,AssadRL,FerrariAJL,AtraE. Panoramicnailfoldcapillaroscopy:anewreadingmethodand normalrange.SeminArthritisRheum.1990;20(1):21–31.
29.DiógenesAHM,BonfaE,FullerR,CorreiaCaleiroMT. Capillaroscopyisadynamicprocessinmixedconnective tissuedisease.Lupus.2007;16(4):254–8.
30.MaricqHR.Widefieldcapillarymicroscopytechniqueand ratingscaleforabnormalitiesseeninsclerodermaand relateddisorders.ArthritisRheum.1981;24(9):1159–65.
31.CutoloM,SulliA,SmithV.Howtoperformandinterpret capillaroscopy.BestPractResClinRheum.2013;27(2):237–48.
32.Dawson-HughesB,HeaneyRP,HolickMF,LipsP,MeunierPJ, ViethR.EstimatesofoptimalvitaminDstatus.Osteoporos Int.2005;16(7):713–6.
33.HollisBW,WagnerCL.NormalserumvitaminDlevels[letter]. NEnglJMed.2005;352(5):515–6.
34.HolickMF.VitaminDdeficiency.NEnglJMed. 2007;357:266–81.
35.SteenVD,MedsgerTAJr.Severeorganinvolvementin systemicsclerosiswithdiffusescleroderma.ArthritisRheum. 2000;43(11):2437–44.
36.Maddali-BongiS,DelRossoA,MikhaylovaS,FranciniB, BranchiA,BacciniM,etal.Impactofhandandface disabilitiesonglobaldisabilityandqualityoflifeinsystemic sclerosispatients.ClinExpRheumatol.2014;326Suppl. 86:S15–20.
Thaisystemicsclerosispatientswithpositiveversusnegative anti-topoisomeraseI.IntJRheumDis.2016;19:312–20.
38.CorradoA,ColiaR,MeleA,DiBelloV,TrottaA,NeveA,etal. Relationshipbetweenbodymasscomposition,bonemineral density,skinfibrosisand25(OH)vitaminDserumlevelsin systemicsclerosis.PLOSONE.2015;10(9):e0137912.
39.Braun-MoscoviciY,FurstDE,MarkovitsD,RozinA,Clements PJ,NahirAM,etal.VitaminD,parathyroidhormone,and acroosteolysisinsystemicsclerosis.JRheumatol. 2008;35(11):2201–5.
40.RobienK,OppeneerSJ,KellyJA,Hamilton-ReevesJM. Drug-vitaminDinteractions:asystematicreviewofthe literature.NutrClinPract.2013;28(2):194–208.
41.ChaoYS,EkwaruJP,OhinmaaA,GrienerG,VeugelersPJ. VitaminDandhealth-relatedqualityoflifeinacommunity sampleofolderCanadians.QualLifeRes.2014;23(9):2569–75.
42.AnglinRE,SamaanZ,WalterSD,McDonaldSD.VitaminD deficiencyanddepressioninadults:systematicreviewand meta-analysis.BrJPsychiatry.2013;202:100–7.
43.BunoutD,BarreraG,LeivaL,GattasV,delaMazaMP, Avenda ˜noM,etal.EffectsofvitaminDsupplementation andexercisetrainingonphysicalperformanceinChilean vitaminDdeficientelderlysubjects.ExpGerontol. 2006;41(8):746–52.
44.vonHurstPR,ConlonC,FoskettA.VitaminDstatuspredicts hand-gripstrengthinyoungadultwomenlivinginAuckland, NewZealand.JSteroidBiochemMolBiol.2013;136:330–2.
45.IngegnoliF,GualtierottiR.Asystematicoverviewontheuse andrelevanceofcapillaroscopyinsystemicsclerosis.Expert RevClinImmunol.2013;9(11):1091–7.
46.TarcinO,YavuzDG,OzbenB,TelliA,OguncAV,YukselM, etal.EffectofvitaminDdeficiencyandreplacementon endothelialfunctioninasymptomaticsubjects.JClin EndocrinolMetab.2009;94(10):4023–30.
47.Shab-BidarS,NeyestaniTR,DjazayeryA,EshraghianMR, HoushiarradA,GharaviA,etal.Regularconsumptionof vitaminD-fortifiedyogurtdrink(Doogh)improved endothelialbiomarkersinsubjectswithtype2diabetes:a randomizeddouble-blindclinicaltrial.BMCMed.2011;9:125.
48.HoffmannMR,SeniorPA,MagerDR.VitaminD supplementationandhealth-relatedqualityoflife:a systematicreviewoftheliterature.JAcadNutrDiet. 2015;115(3):406–18.
49.LimaGL,PaupitzJ,AikawaNE,TakayamaL,BonfaE,Pereira RM.VitaminDsupplementationinadolescentsandyoung adultswithjuvenilesystemiclupuserythematosusfor improvementindiseaseactivityandfatiguescores:a randomized,double-blindplacebo-controlledtrial.Arthritis CareRes.2016;68(1):91–8.
50.HussinAM,AshorAW,SchoenmakersI,HillT,MathersJC, SiervoM.EffectsofvitaminDsupplementationon