w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Substance
use
and
sexual
function
in
juvenile
idiopathic
arthritis
Marlon
van
Weelden
a,b,
Benito
Lourenc¸o
c,
Gabriela
R.
Viola
a,
Nadia
E.
Aikawa
a,
Lígia
B.
Queiroz
c,
Clovis
A.
Silva
a,c,∗aPediatricRheumatologyUnit,FaculdadedeMedicina,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil bMedicalFaculty,VUUniversity,Amsterdam,TheNetherlands
cAdolescentUnit,FaculdadedeMedicina,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received18June2015 Accepted13October2015 Availableonline11March2016
Keywords:
Alcohol Tobacco Illicitdrug Bullying
Juvenileidiopathicarthritis
a
b
s
t
r
a
c
t
Objective:To evaluatealcohol/tobacco/illicitdrug useandsexualfunctionin adolescent juvenileidiopathicarthritis(JIA)andhealthycontrols.
Methods:174 adolescents with pediatric rheumatic diseases were selected. A cross-sectionalstudywith54JIApatientsand35controlsincludeddemographic/anthropometric data and pubertymarkers assessments, physician-conducted CRAFFT (car/relax/alone/ forget/friends/trouble)screentoolforsubstanceabuse/dependencehighriskanda ques-tionnaire thatevaluated sexual function,bullying and alcohol/tobacco/illicit drug use. Clinical/laboratorialdataandtreatmentwerealsoassessedinJIA.
Results:ThemediancurrentagewassimilarbetweenJIApatientsandcontrols[15(10–19) vs.15(12–18)years,p=0.506].Frequenciesofalcohol/tobacco/illicitdrugusewerehighand similarinbothJIAandcontrols(43%vs.46%,p=0.829).However,ageatalcoholonsetwas significantlyhigherinthosewithJIA[15(11–18)vs.14(7–18)years,p=0.032],particularlyin polyarticularonset(p=0.040).Highriskforsubstanceabuse/dependence(CRAFFTscore≥2) wasfoundinbothgroups(13%vs.15%,p=1.000),likewisebullying(p=0.088).Further analy-sisofJIApatientsregardingalcohol/tobacco/illicitdruguseshowedthatthemediancurrent age[17(14–19)vs.13(10–19)years,p<0.001]andeducationyears[11(6–13)vs.7(3–12)years,
p<0.001]weresignificanthigherinthosethatusedsubstances.Sexualactivitywas signifi-cantlyhigherintheformergroup(48%vs.7%,p<0.001).Apositivecorrelationwasevidenced betweenCRAFFTscoreandcurrentageinJIApatients(p=0.032,r=+0.296).
Conclusion: Ahighriskforsubstanceabuse/dependencewasobservedinbothJIAand con-trols.JIAsubstanceusersweremorelikelytohavesexualintercourse.Therefore,routine screeningissuggestedinallvisitsofJIAadolescents.
©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](C.A.Silva).
http://dx.doi.org/10.1016/j.rbre.2016.02.007
Uso
de
substâncias
e
func¸ão
sexual
na
artrite
idiopática
juvenil
Palavras-chave:
Álcool Tabaco Drogasilícitas
Bullying
Artriteidiopáticajuvenil
r
e
s
u
m
o
Objetivo: Avaliarousodeálcool/tabaco/drogasilícitaseafunc¸ãosexualemadolescentes comartriteidiopáticajuvenil(AIJ)econtrolessaudáveis.
Métodos: Selecionaram-se174adolescentescomdoenc¸asreumatológicaspediátricas. Fez-seumestudotransversalcom54pacientescomAIJe35controles.Foramfeitasavaliac¸ões dedadosdemográficos/antropométricosemarcadoresdapuberdade;aescaladetriagem CRAFFT (carro/relaxar/sozinho/esquecer/amigos/problemas)foiaplicadapor um médico paradeterminaroaltoriscodeusoabusivo/dependênciadesubstâncias.Umquestionário avaliouafunc¸ãosexual,aocorrênciadebullyingeousodeálcool/tabaco/drogasilícitas. Tambémforamavaliadosdadosclínicos/laboratoriaisedetratamentodaAIJ.
Resultados: AidademédiaatualfoisemelhanteentrepacientescomAIJecontroles[15 (10a19)vs.15 (12a 18)anos, p=0,506].Asfrequências deusodeálcool/tabaco/drogas ilícitasforamelevadasesemelhantesentrepacientescomAIJecontroles(43%vs.46%, p=0,829).Noentanto,aidadeemquecomec¸ouausarálcoolfoisignificativamentemaior naquelescomAIJ[15(11a18)vs.14(7a18anos),p=0,032],emparticularnadoenc¸ade iníciopoliarticular(p=0,040).Encontrou-seumaltoriscodeusoabusivo/dependênciade substâncias(pontuac¸ãonoCRAFFT≥2)emambososgrupos(13%vs.15%,p=1,000),do mesmomodoqueobullying(p=0,088).Umaanálisemaisaprofundadadospacientescom AIJemrelac¸ãoaousodeálcool/tabaco/drogasilícitasmostrouqueaidademédiaatual[17 (14a19)vs.13(10a19)anos,p<0,001]eosanosdeescolaridade[11(6a13)vs.7(3a12)anos, p<0,001]foramsignificativamentemaioresnaquelesqueusaramsubstâncias.Aatividade sexualfoisignificativamentemaiornoprimeirogrupo(48%vs.7%,p<0,001).Foievidenciada correlac¸ãopositivaentreapontuac¸ãonaescalaCRAFFTeaidadeatualdospacientescom AIJ(p=0,032,r=+0,296).
Conclusão: Observou-se um alto risco de usoabusivo/dependência de substâncias em pacientescomAIJecontroles.OsusuáriosdesubstânciasquetêmAIJsãomais propen-sosaterrelac¸õessexuais.Portanto,sugere-seatriagemderotinaemtodasasconsultasde adolescentescomAIJ.
©2016ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Adolescenceisanimportantphasetodevelopapositivebody image,toestablishsocialrelationships,toachieve indepen-dence and sexual identity. Some of the biggest problems during this period in healthy adolescents are substance misuse,1,2 precocious sexual activity, reduced use of
con-traceptivemethodsand higherriskofsexually transmitted infections.3
Inaddition, the use ofalcohol, tobacco andillicitdrugs seemstoberelevantinadolescentswithchronicconditions, thatmayleadtoaddiction1andhigh-risksexualbehavior.2,3
Smokingprovokecardiovasculardisease andalcoholintake caninduceliverdamageinpatientswithautoimmune dis-eases under methotrexate therapy.3 The substance use in
chronicconditionsmayalsoinducepooradherencetomedical treatment,resultingindiseaseactivityanddecrease health-relatedqualityoflife.
Adolescents may also suffer from bullying victimiza-tion, particularly those with chronic diseases.4 However,
these issues have not been investigated simultaneously in an adolescent juvenile idiopathic arthritis (JIA) popula-tion.
Therefore, the aims of the present study were to eval-uate alcohol, tobacco and/or illicit drug use in adolescent JIApatientsandhealthycontrols.Thepossibleassociations between the use of the aforementioned substances in JIA patients and: demographic data, puberty markers, sexual function, bullying, JIA clinical parameters and treatments werealsoassessed.
Materials
and
methods
Patientsandcontrols
Rheumatismcriteria5wereeligibletoparticipate.Thecontrol
groupincluded35healthyadolescents,withoutchronic dis-eases,referredfromtheprimaryandsecondaryhealthcare servicestotheAdolescentUnitofourteachingUniversity Hos-pital.Thiscross-sectionalstudy wasapprovedbythe Local EthicsCommitteeofourUniversityHospital.
Pubertymarkers,sexualfunctionand alcohol/tobacco/illicitdruguse,andbullying
Thisstudy includeddemographic/anthropometric dataand puberty markers assessments. The Portuguese CRAFFT (mnemonicacronymofcar,relax,alone,forget,friendsand trouble)screen(CRAFFT/CEASER)versionwasperformedfor both groups.2,6 A modified questionnaire evaluated sexual
function,7alcohol/tobacco/illicitdruguseandbullying.These
aspectswerecarriedout blindedtoJIAclinical,laboratorial andtreatmentdataconductedbyasingleinvestigator.
Socio-demographicandanthropometricdata
Currentage, gender,years ofeducation,weightand height wereevaluated. Bodymassindex(BMI) wasdefinedbythe formula:weightinkilograms/heightinsquaremeters.
The Brazilian socio-economic classes were classified accordingtotheABEP(Associac¸a˜oBrasileiradeEmpresasde Pesquisa).8
Pubertymarkersassessments
Secondarysexualcharacteristicswereclassifiedaccordingto Tannerpubertalchanges.7Ageatfirstmenstruation
(menar-che)andfirstejaculation(spermarche)wereregisteredbased onmemoryrecollection.
CRAFFTscreening
The validated Portuguese version of physician-conducted CRAFFT(CRAFFT/CEASER)screenwasusedandconsistedof ninequestionsdevelopedtoscreenadolescentsforhigh-risk alcoholanddruguse.6Thisquestionnaireisdividedintwo
parts. PartAincludesthree questionsregardingthe use of alcohol,marijuana,hashishoranothersubstanceinthelast twelvemonths.Iftheadolescentresponded“no”toallthree questions,only the question related to “car”of the B-part shouldbeasked.Iftheadolescentanswered“yes”tooneof theopeningquestions,allofthequestionsofpartBshould beasked.B-partcontainedsixquestions,whicharesignsof problematicsubstanceuse.Onepointwasgiventoeach“yes” answerintheB-partofthequestionnaire.Thescoreranged from0to6.Atotalscoreof≥2indicatedhighriskforsubstance abuse/dependenceandaneedforadditionalassessment.2,6
Questionnaireadministration
Apilotstudywascarriedoutin30consecutivehealthyandJIA adolescents,whoweretestedandretestedafter1–2months. The pretest evaluated the subjects’ comprehension of the questions,theconsistencyandcoherenceoftheanswersand thetimetakentoanswerthequestionnaire.Thequestionnaire
included 14 questions with the option of answer “yes/no” orage/numberoftimesaboutsexualfunction,bullyingand alcohol/tobacco/illicitdrugsuse.Sexualfunctionassessment included:ageatfirstsexualintercourse,sexualintercoursein the lastmonth, use ofmale contraceptive(condom) inthe firstsexualactivity,currentuseoforalandemergency con-traceptive,knowledgeofsexualactivitybyparentsandtotal numberofsexualpartners.Alcohol/tobaccoanddrugs[illicit inhalantsdrug(gluesniffing,aerosolandsolvents)andillicit drugs[marijuana,stimulants(cocaine,crackandspeed), pop-pers,LSD,opiates,heroin,crystalmethandecstasy]usewere alsoassessed:ageatalcoholinitiation,numberofdaysof alco-holusedinthelast30days,ageatsmokinginitiation,number ofdaysusingcigarettesinthelast30days,ageatillicitdrug initiation andnumberofdaysusingillicitdrugsinthe last 30 days.Bullying,which isdefinedasarecurrentexposure toemotionaland/orphysicalaggression,wasobtainedbya “yes/no”answertothequestion“Haveyoueversuffered bul-lying?”.Thequestionnairewasstrictlyconfidentialandwas performed inthe absence of legalguardians, relatives and friends.
JIAclinical,laboratorialandtreatmentassessments
Clinical assessments of JIA patients were assessed at the study entryandincluded: numberofactivejoints(swelling within a joint, or limitation in the range of joint move-ment with joint pain or tenderness), number of limited joints,patient and physicianglobal assessmentofarthritis activity measuredina10cmhorizontalvisualanalogscale (VAS), morning stiffness duration and Brazilian version of ChildhoodHealthAssessmentQuestionnaire(CHAQ).9
Labo-ratorialassessmentincludederythrocytesedimentationrate (ESR>20mm/1sthour) (Westergren method) and C-reactive protein (CRP>5mg/L) (nephelometry). Data concerning the use and current dosageofnon-steroidalanti-inflammatory drugs (NSAIDs), prednisone, DMARDs (methotrexate, sul-phasalazine and leflunomide), immunosuppressive drugs (cyclosporine)andbiologicalagents(adalimumab,etanercept, tocilizumabandabatacept)werealsodetermined.
Statisticalanalysis
Thetest–retestreliabilityofthemodifiedquestionnairewas verifiedusingtheKappaindex.Resultswerepresentedasthe mean±standard deviation (SD)or median (range)for con-tinuousandnumber(%)forcategoricalvariables.Datawere compared byt or Mann–Whitney tests in continuous vari-ablestoevaluatedifferencesbetweenJIAand controls,and betweenJIAsubgroups.Forcategoricalvariables,differences wereassessedbyFisher’sexactorPearsonchi-squaretests. Spearmanrankcorrelationcoefficientwasusedfor correla-tionsbetweenCRAFFTscoreandage.Thelevelofsignificance wassetat5%(p<0.05).
Results
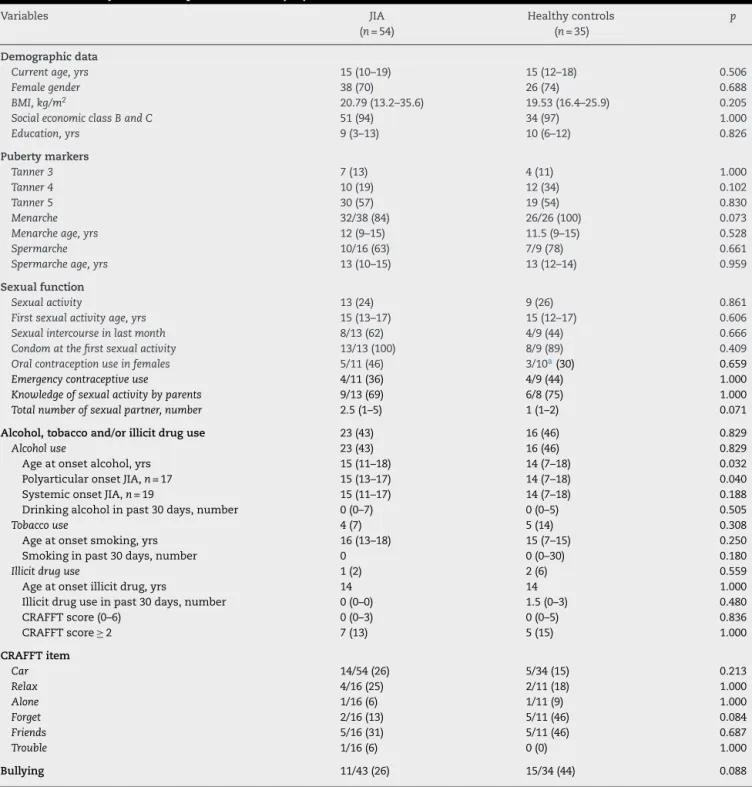
Table1–Demographicdata,pubertymarkers,sexualfunction,alcohol,tobaccoandillicitdruguse,andbullyingin adolescentswithjuvenileidiopathicarthritis(JIA)andcontrols.
Variables JIA
(n=54)
Healthycontrols (n=35)
p
Demographicdata
Currentage,yrs 15(10–19) 15(12–18) 0.506
Femalegender 38(70) 26(74) 0.688
BMI,kg/m2 20.79(13.2–35.6) 19.53(16.4–25.9) 0.205
SocialeconomicclassBandC 51(94) 34(97) 1.000
Education,yrs 9(3–13) 10(6–12) 0.826
Pubertymarkers
Tanner3 7(13) 4(11) 1.000
Tanner4 10(19) 12(34) 0.102
Tanner5 30(57) 19(54) 0.830
Menarche 32/38(84) 26/26(100) 0.073
Menarcheage,yrs 12(9–15) 11.5(9–15) 0.528
Spermarche 10/16(63) 7/9(78) 0.661
Spermarcheage,yrs 13(10–15) 13(12–14) 0.959
Sexualfunction
Sexualactivity 13(24) 9(26) 0.861
Firstsexualactivityage,yrs 15(13–17) 15(12–17) 0.606
Sexualintercourseinlastmonth 8/13(62) 4/9(44) 0.666
Condomatthefirstsexualactivity 13/13(100) 8/9(89) 0.409
Oralcontraceptionuseinfemales 5/11(46) 3/10a(30) 0.659
Emergencycontraceptiveuse 4/11(36) 4/9(44) 1.000
Knowledgeofsexualactivitybyparents 9/13(69) 6/8(75) 1.000
Totalnumberofsexualpartner,number 2.5(1–5) 1(1–2) 0.071
Alcohol,tobaccoand/orillicitdruguse 23(43) 16(46) 0.829
Alcoholuse 23(43) 16(46) 0.829
Ageatonsetalcohol,yrs 15(11–18) 14(7–18) 0.032
PolyarticularonsetJIA,n=17 15(13–17) 14(7–18) 0.040
SystemiconsetJIA,n=19 15(11–17) 14(7–18) 0.188
Drinkingalcoholinpast30days,number 0(0–7) 0(0–5) 0.505
Tobaccouse 4(7) 5(14) 0.308
Ageatonsetsmoking,yrs 16(13–18) 15(7–15) 0.250
Smokinginpast30days,number 0 0(0–30) 0.180
Illicitdruguse 1(2) 2(6) 0.559
Ageatonsetillicitdrug,yrs 14 14 1.000
Illicitdruguseinpast30days,number 0(0–0) 1.5(0–3) 0.480
CRAFFTscore(0–6) 0(0–3) 0(0–5) 0.836
CRAFFTscore≥2 7(13) 5(15) 1.000
CRAFFTitem
Car 14/54(26) 5/34(15) 0.213
Relax 4/16(25) 2/11(18) 1.000
Alone 1/16(6) 1/11(9) 1.000
Forget 2/16(13) 5/11(46) 0.084
Friends 5/16(31) 5/11(46) 0.687
Trouble 1/16(6) 0(0) 1.000
Bullying 11/43(26) 15/34(44) 0.088
CRAFFT,car,relax,alone,forget,friends,troubleinthelast12months;screeningtest. Theresultsarepresentedinn(%)andmedian(range)ormean±SD.
a Onehealthycontrolusedoralcontraceptionbeforesexualactivity.
ThemediancurrentagewassimilarbetweenJIApatients andcontrols[15(10–19)vs.15(12–18)years,p=0.506],likewise the frequency offemale gender (p=0.688), years of educa-tion(p=0.826),socialeconomicclasses(p=1.000)andTanner 5(p=0.830).Themedianmenarcheageandspermarcheage werealsoalike[12(9–15) vs.11.5(9–15) years,p=0.528and 13(10–15)vs.13(12–14)years,p=0.959],respectively,aswell asfrequencyofsexualactivity(p=0.861)andageofthefirst
sexual intercourse[15 (13–17)vs.15 (12–17)years,p=0.606] (Table1).
Table2–Demographicdata,pubertymarkers,bullyinganddiseaseparametersinadolescentswithjuvenileidiopathic arthritis(JIA)accordingtoalcohol,tobaccoandillicitdruguse.
Variables Usealcohol,tobaccoand/or
illicitdrug (n=23)
Nonusealcohol,tobaccoand/or illicitdrug
(n=31)
p
Demographicdata
Currentage,yrs 17(14–19) 13(10–19) <0.001
Diseaseduration,yrs 6(1–17) 4(0.25–15) 0.063
Femalegender 16(70) 22(71) 0.911
BMI,kg/m2 21.15(18–27) 20.09(13–30) 0.132
SocialeconomicclassBandC 22(96) 28(90) 0.628
Education,yrs 11(6–13) 7(3–12) <0.001
Pubertymarkers
Tanner3 1(4) 6(20) 0.123
Tanner4 3(13) 7(23) 0.484
Tanner5 19(83) 11(37) 0.001
Menarche 16(100) 16(73) 0.030
Menarcheage,yrs 12(9–15) 12(9–14) 0.861
Spermarche 7(100) 3(33) 0.011
Spermarcheage,yrs 13(12–15) 11(10–13) 0.082
Sexualfunction
Sexualactivity 11(48) 2(7) <0.001
Firstsexualactivityage,yrs 16(13–17) 14(14) 0.227
Sexualintercourseinlastmonth 7/11(64) 1/2(50) 1.000
Condomatthefirstsexualactivity 11/11(100) 2/2(100) 1.000
Oralcontraceptionuseinfemales 4/9(44) 1/2(50) 1.000
Emergencycontraceptiveuse 4/9(44) 0 0.491
Knowledgeofsexualactivitybyparents 7/11(64) 2/2(100) 1.000
Totalnumberofsexualpartner,number 3(1–5) 1(1) 0.074
Bullying 5/18(28) 6/25(24) 1.000
JIAparameters
Morningstiffness 7(30) 2/29(7) 0.061
Morningstiffness,min 30(10–120) 20(10–30) 0.492
Activejoints 7(30) 10(32) 0.887
Numberofactivejoints 1(1–8) 1(1–9) 0.956
Limitedjoints 16(70) 20(65) 0.697
Numberoflimitedjoints 2(1–11) 3.5(1–61) 0.165
ESR,mm/1sth 14.5(2–60) 20(2–47) 0.809
ESR,>20mm/1sth 10/22(46) 11/27(41) 0.740
CRP,mg/L 2.23(0–76) 1.23(0–155) 0.847
CRP,>5mg/L 6/22(27) 7/26(27) 0.978
Patient’sVAS,cm 1(0–9) 1(0–5) 0.748
Physician’sVAS,cm 0(0–4) 1(0–4) 0.307
CHAQ 0.56(0–2.6) 0.63(0–1.5) 0.779
Currenttreatment 19(83) 29(94) 0.384
NSAID 7(30) 16(52) 0.120
Naproxen 2(9) 6(19) 0.443
Glucocorticoids 3(13) 8(26) 0.319
Dose,mg/day 11.3(2.5–40) 5(2.5–25) 0.214
Methotrexate 4(17) 6(19) 1.000
Dose,mg/week 25(10–50) 25(10–37.5) 0.731
Leflunomide 3(13) 5(16) 1.000
Dose,mg/day 20(20) 20(10–20) 0.094
Sulfasalazine 0 1(3) 1.000
Cyclosporine 2(9) 3(10) 1.000
Dose,mg/day 190(180–200) 150(100–200) 0.584
Biologicalagents 12(52) 10(32) 0.141
Abatacept 1(4) 2(7) 1.000
Etanercept 5(22) 3(10) 0.217
Adalimumab 4(17) 3(10) 0.443
Tocilizumab 2(9) 2(7) 1.000
Illicit drugs were used by one JIA patient (marijuana and cocaine)andtwocontrols(marijuana)(p=0.559)andno dif-ferencewasobservedinthefrequencyoftobaccouse.CRAFFT score≥2wassimilarinbothgroups(13%vs.15%,p=1.000).Of our7JIApatientswithCRAFFTscore≥2,4hadpolyarticular onset,5usedmethotrexateand6biologicalagents.The fre-quencyofbullyingwaslowerinpatientswithJIAvs.controls, howeveritdidnotreachstatisticalsignificance(26%vs.44%,
p=0.088)(Table1).
OfJIAsubtypes,systemiconsetwasobservedin19patients, polyarticular in 17, pauciarticular in 13, enthesitis-related arthritisin3andpsoriaticarthritisin2.Furtheranalysisof JIApatientsregardingalcohol/tobacco/illicitdruguseshowed thatthemediancurrentage[17(14–19)vs.13(10–19)years,
p<0.001]and education years [11 (6–13) vs. 7(3–12) years,
p<0.001]weresignificantlyhigherinthosethatusedthe afore-mentionedsubstances.ThefrequenciesofTanner5(p=0.001), menarche(p=0.030)andspermarche(p=0.011)werealso sig-nificantlyhigherintheformergroup,likewisesexualactivity (48%vs.7%,p<0.001).Nodifferenceswereevidencedbetween alcohol/tobacco/illicitdruguseand diseaseparametersand currenttreatmentinbothgroups(p>0.05,Table2).
A positive correlation was evidenced between CRAFFT score and current age in JIA patients (p=0.032, r=+0.296), withnocorrelationincontrols(p=0.571).Nocorrelationswere evidenced betweenCRAFFTscore andage ofalcoholonset (p=0.751),onsetofsexualintercourse(p=0.606)andeducation years(p=0.066)inJIApatients.
Discussion
Tothebest ofourknowledge,this wasthe first studythat assessedsimultaneouslyadolescenthealthissuesinJIA pop-ulationandcontrols,andevidencedahigherageatalcohol onsetinpatients,mainlyinpolyarticularsubtype.IntheJIA adolescentgroup,substanceusersweremorelikelytohave sexualintercourse.Wealsofoundahigherriskforsubstance abuse/dependenceatlaterageinJIAadolescents.
Theadvantageofthepresentstudywastheevaluationof physician-conductedCRAFFT (CEASER) screeningtool. This scoreisusedtodeterminethehigh-riskofalcoholanddrug dependenceinadolescents.2,6Aquestionnairewithexcellent
test–retestreliabilitythatevaluatedsexualfunction,bullying and licit/illicitdrug consumptionwas alsoused. Ahealthy controlgroupwithsimilarage,academicbackground,gender andsocio-economicclasswaspertinentherein,sincethese datawererelatedwithbullyinganddruguse.1,2However,the
mainweaknessesofthisstudywasthecrosssectional anal-ysis,aswellasthesmallsamplestudiedandthelackofthe evaluationofdifferentformsofbullying.
Alcoholusewaspreviouslyreportedin36%ofadolescent andyoungadultswithpediatricrheumaticdiseases.10In
addi-tion,Nash etal.reporteda19%ofalcoholexperimentation in52JIAadolescents,11 contrastingto43%observedherein.
Thisfindingmayberelatedtoanincreasedalcoholintakein adolescentsduringthenineties12andtheeconomicgrowth
inourcountry,13thusenablingmiddlesocio-economicclass
toconsume.Therefore,restrictionstrategiesarerequiredto decreasealcoholuse.
Ofnote,theageatalcoholonsetwashigherinJIApatients, especiallyinpolyarticularonsetundermethotrexateand bio-logicalagents.Ourpatientsignoredtheinformationtoavoid substance useconcomitant tobiological andnon-biological DMARDs, with a high risk to adverse events, particularly hepatotoxicity.11Weusedascreeningprocedureforsubstance
use.2,6Indeed,CRAFFTscore≥2inourJIApatientsindicated
higherriskforsubstanceabuse/dependence.2Basedonthat,
additional assessmentand therapeuticintervention witha multidisciplinaryandmultiprofessionalteamisrequired.
Importantly, JIA substance users engaged more in sex-ual activity, withpossibleunsafesexual relations, sexually transmitteddiseasesandpregnancy.Thisfindingmaybealso relatedtothefactthatthe patientswereolderwithhigher sexualmaturity.DespiteJIAisapainful,chronicanddisability disease,andmayinfluencesexualfunction,14,15ourpatients
presentedtheirfirstsexualactivityearlier.
A delay of puberty markers was not evidenced in JIA patients, which is a distinct pattern in our adolescent with juvenile systemic lupus erythematosus15 and
juve-niledermatomyositis.16Inaddition,bullyingwasfrequently
reportedinJIAandcontrolsthatmaycausedepression, anx-ietyandinterferewithproperadherenceofmedicationuse.4
Aprospectivestudy,recruitinglargersampleofJIAand evalu-atingtheseaspects,willbenecessary.
Inconclusion,highriskforsubstanceabuse/dependence was observedinbothJIAandcontrols.JIAsubstance users weremorelikelytohavesexualintercourse.Ourstudy rein-forcesthatJIAadolescentsshouldbesystematicallyscreened bypediatriciansforsexual,alcoholanddrugshealth behav-ioralpatterns,aspartofPediatricRheumatologyservicevisits. AlcoholandcontraceptioneducationtoJIApatients,especially thosetreatedwithmethotrexateandbiologicagents,should beincludedintheroutinecare.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
OurgratitudetoUlyssesDoria-Filhoforthestatistical analy-sis.WethankDr.JRKnight andDr.PSchramforsupplying the Portugueseversion ofCRAFFT screen (CEASER) instru-ment,BostonChildren’sHospital,MA, USA.Thisstudy was supported bygrantsfrom Fundac¸ãode Amparo àPesquisa doEstadodeSãoPaulo(FAPESP2011/12471-2toCAS), Con-selhoNacionaldeDesenvolvimentoCientíficoeTecnológico (CNPQ 302724/2011-7toCAS),FedericoFoundation(toCAS), andNúcleodeApoioàPesquisa“SaúdedaCrianc¸aedo Ado-lescente”daUSP(NAP-CriAd)toCAS.
r
e
f
e
r
e
n
c
e
s
withfocusondevelopingcountries.JPsychiatrMentHealth Nurs.2014;21:609–17.
2. LevyS,SherrittL,GabrielliJ,ShrierLA,KnightJr.Screening adolescentsforsubstanceuse-relatedhigh-risksexual behaviors.JAdolescHealth.2009;45:473–7.
3. SawyerSM,DrewS,YeoMS,BrittoMT.Adolescentswitha chroniccondition:challengesliving,challengestreating. Lancet.2007;369:1481–9.
4. SentenacM,GavinA,GabhainnSN,MolchoM,DueP, Ravens-SiebererU,etal.Peervictimizationandsubjective healthamongstudentsreportingdisabilityorchronicillness in11Westerncountries.EurJPublicHealth.2013;23:421–6.
5. PettyRE,SouthwoodTR,MannersP,BaumJ,GlassDN, GoldenbergJ,etal.Revisionoftheproposedclassification criteriaforjuvenileidiopathicarthritis:Durban,1997.J Rheumatol.1998;25:1991–4.
6. KnightJR,SchramP.PortugueseversionofCRAFFTscreen (CEASER).Availablefrom:http://www.ceasar-boston.org/ CRAFFT/pdf/CRAFFTPortuguese.pdf[accessedinJuly,17, 2014].
7. FebronioMV,PereiraRM,BonfaE,TakiutiAD,PereyraEA, SilvaCA.Inflammatorycervicovaginalcytologyisassociated withdiseaseactivityinjuvenilesystemiclupus
erythematosus.Lupus.2007;16:430–5.
8. ABEP(Associac¸a˜oBrasileiradeEmpresasdePesquisa)2008: Availablefrom:www.abep.org–[email protected][accessedin July17,2014].
9. MachadoCS,RupertoN,SilvaCH,FerrianiVP,RoscoeI, CamposLM,etal.PaediatricRheumatologyInternational
TrialsOrganisation.TheBrazilianversionoftheChildhood HealthAssessmentQuestionnaire(CHAQ)andtheChild HealthQuestionnaire(CHQ).ClinExpRheumatol.2001;19 Suppl.23:S25–9.
10.BrittoMT,RosenthalSl,TaylorJ,PassoMH.Improving rheumatologists’screeningforalcoholuseandsexual activity.ArchPediatrAdolescMed.2000;154:478–83.
11.NashAA,BrittoMT,LovellDJ,PassoMH,RosenthalSL. Substanceuseamongadolescentswithjuvenilerheumatoid arthritis.ArthritisCareRes.1998;11:391–6.
12.PoelenEA,ScholteRH,EngelsRC,BoomsmaDI,WillemsenG. Prevalenceandtrendsofalcoholuseandmisuseamong adolescentsandyoungadultsintheNetherlandsfrom1993 to2000.DrugAlcoholDepend.2005;79:413–21.
13.MadrugaCS,LaranjeiraR,CaetanoR,PinskyI,ZaleskiM,Ferri CP.Useoflicitandillicitsubstancesamongadolescentsin Brazil—anationalsurvey.AddictBehav.2012;37:1171–5.
14.deAvilaLimaSouzaL,GallinaroAL,AbdoCH,KowalskiSC, SuehiroRM,daSilvaCA,etal.Effectofmusculoskeletalpain onsexualityofmaleadolescentsandadultswithjuvenile idiopathicarthritis.JRheumatol.2009;36:1337–42.
15.AikawaNE,SallumAM,PereiraRM,SuzukiL,VianaVS,Bonfá E,etal.Subclinicalimpairmentofovarianreserveinjuvenile systemiclupuserythematosusaftercyclophosphamide therapy.ClinExpRheumatol.2012;30:445–9.