www.jped.com.br
REVIEW
ARTICLE
Management
protocols
for
status
epilepticus
in
the
pediatric
emergency
room:
systematic
review
article
夽
Cheuk
C.
Au
a,b,
Ricardo
G.
Branco
c,∗,
Robert
C.
Tasker
a,daBostonChildren’sHospital,DepartmentofAnesthesiology,PerioperativeandPainMedicine,DivisionofCriticalCareMedicine,
Boston,UnitedStates
bQueenMaryHospital,DepartmentofPaediatricandAdolescentMedicine,HongKong,China
cCambridgeUniversityHospitalsNHSTrust,PaediatricIntensiveCareUnit,Cambridge,UnitedKingdom dBostonChildren’sHospital,DepartmentofNeurology,Boston,UnitedStates
Received7June2017;accepted23July2017 Availableonline21September2017
KEYWORDS Statusepilepticus; Seizure;
Protocol; Guideline
Abstract
Objective: ThissystematicreviewofnationalorregionalguidelinespublishedinEnglishaimed tobetterunderstandvarianceinpre-hospitalandemergencydepartmenttreatmentofstatus epilepticus.
Sources: Systematicsearchofnationalorregionalguidelines(January2000toFebruary2017) containedwithinPubMedandGoogleScholardatabases,andarticlereferencelists.Thesearch keywordswerestatusepilepticus,prolongedseizure,treatment,andguideline.
Summaryoffindings: 356articleswereretrievedand13wereselectedaccordingtothe inclu-sioncriteria.Inallsixpre-hospitalguidelines,thepreferredrouteofmedicationadministration was to use alternatives to the intravenous route: all recommended buccal and intranasal midazolam;threealsorecommendedintramuscularmidazolam,andfiverecommendedusing rectaldiazepam.All11emergencydepartmentguidelinesdescribedthreephasesintherapy. Intravenousmedication,byphase,wasindicatedassuch:initialphase---ten/11guidelines rec-ommendedlorazepam,andeight/11recommendeddiazepam;secondphase---most(ten/11) guidelinesrecommendedphenytoin,butotheroptionswerephenobarbital(nine/11),valproic acid(six/11),andeitherfosphenytoinorlevetiracetam(eachfour/11);thirdphase---four/11 guidelinesincludedthechoiceofrepeatingsecondphasetherapy,whereastheother guide-linesrecommendedusingavarietyofintravenousanestheticagents(thiopental,midazolam, propofol,andpentobarbital).
Conclusions: Alloftheguidelinesshareasimilarframeworkformanagementofstatus epilep-ticus.Thechoiceinrouteofadministrationanddrugtypevariedacrossguidelines.Hence,the
夽
Pleasecitethisarticleas:AuCC,BrancoRG,TaskerRC.Managementprotocolsforstatusepilepticusinthepediatricemergencyroom:
systematicreviewarticle.JPediatr(RioJ).2017;93:84---94.
∗Correspondingauthor.
E-mail:[email protected](R.G.Branco).
http://dx.doi.org/10.1016/j.jped.2017.08.004
adoptionofaparticularguidelineshouldtakeaccountoflocalpracticeoptionsinhealthservice delivery.
©2017SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/
4.0/).
PALAVRAS-CHAVE Estadodemal epiléptico; Convulsão; Protocolo; Diretriz
Protocolosdemanejodeestadodemalepilépticonoprontosocorropediátrico:
análisesistemática
Resumo
Objetivo: Estaanálisesistemática dediretrizes nacionaisouregionaispublicadas em inglês tem comoobjetivoentendermelhoradiferenc¸anotratamentodoestadodemalepiléptico pré-hospitalarenodepartamentodeemergência.
Fontes: Pesquisasistemáticadediretrizesnacionaisouregionais(janeirode2000afevereiro de2017)contidasnasbasededadosdoPubmededoGoogleAcadêmicoelistasdereferência deartigos.Aspalavras-chavedabuscaforamestadodemalepiléptico,convulsãoprolongada, tratamentoediretriz.
Resumodoachados: 356artigosforamidentificados,e13foramselecionadosdeacordocom oscritériosdeinclusão.Emtodasasseisdiretrizespré-hospitalares,ocaminhopreferencial de administrac¸ão da medicac¸ão foi utilizar alternativasà via intravenosa:todas recomen-darammidazolambucaleintranasal;trêstambémrecomendarammidazolamintramuscular;e cincorecomendaramutilizarodiazepamviaretal.Todasas11diretrizesdedepartamentode emergênciadescreveramtrêsfasesnaterapia.Noquedizrespeitoàmedicac¸ãointravenosa, porfase,temos:faseinicial---10/11diretrizesrecomendaramlorazepame8/11recomendaram diazepam;segundafase---amaioria(10/11)dasdiretrizesrecomendoufenitoína,porém out-rasopc¸õesforamfenobarbital(9/11),ácidovalpróico(6/11)efosfenitoínaoulevetiracetam (individualmente, 4/11);terceira fase---4/11diretrizes incluíramaopc¸ãoderepetir a ter-apiadasegundafase,aopassoqueasoutrasdiretrizesrecomendaramutilizardiversosagentes anestésicosintravenosos(tiopental,midazolam,propofolepentobarbital).
Conclusões: Todasasdiretrizescompartilhamumaestruturasemelhanteparamanejodoestado demalepiléptico.Aescolhadaviadeadministrac¸ãoedotipodemedicamentovariouemtodas asdiretrizes.Assim,aadoc¸ãodeumadiretrizespecíficadevelevaremconsiderac¸ãoasopc¸ões dapráticalocalnaprestac¸ãodeservic¸osdesaúde.
©2017SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.
0/).
Introduction
Status epilepticus (SE) is defined as ‘‘a condition result-ing either from the failure of mechanisms responsible for seizure termination or from the initiation of mecha-nisms which lead toabnormally prolongedseizures (after time point t1), and a condition that can have long-term consequences (after time point t2), including neuronal death,neuronalinjury,andalterationofneuronalnetworks, dependingonthetypeanddurationofseizures,etc.Inthe caseofconvulsive(tonic---clonic)SE,bothtimepoints(t1at 5minandt2at30min)arebasedonanimalexperimentsand clinicalresearch’’.1
Therefore, in children, there are two subgroups of patientspresentingwithaseizure:thosewithbriefepisodes <5minduration(beforet1)thatarehighlylikelytoresolve
withouttreatment;andthosewithepisodes>7min,whoare more likelyto progress to prolonged episodes necessitat-ingacutetreatmenttostoptheseizure.The consensusof theInternationalLeagueAgainstEpilepsy (ILAE)taskforce onthe classificationof SEis thattreatment ofconvulsive seizuresshouldthereforebeinitiatedataround5min.1
This article discusses some of the issues related to emergency anticonvulsant treatment of acute, prolonged seizures and SE in children with particular emphases on pre-hospital,emergencymedicalservices(EMS),and emer-gency department (ED) guidelines, as well as protocols usedbynationalandregionalsocieties,organizations,and authorities. The reader interested in other management, investigations,andsubsequentclinicalfollow-upinthe out-patient department or by the primary care practitioner should review recent practice reviews and the American AcademyofNeurologyrecommendations.2,3
Methods
Sourceofdata
English: status epilepticus, prolonged seizure, treatment, andguideline.
Selectioncriteria
In thisqualitative review,articles were selected for con-sideration using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) group 2009 statement.4Publishedarticleswereincludedinthereview
when they met the following criteria: (1) protocol or guidelineonthe useof anticonvulsantdrugtreatment for prolonged seizure or SE published January 1st, 2000 to February28th,2017;(2)publicationthatfeaturedanational orregionalguidelineforthepediatricpopulationintheEMS orEDsetting;and(3)whenmorethanonearticlewas iden-tifiedfromthesameorganizationorsociety,themostrecent publicationwasincluded.
Allarticlesthatmettheinclusioncriteriaweresubmitted todataextraction andcriticalevaluation by each author. The main characteristics weresummarized following data extraction:authorship;periodofmanagement;EMSorED; time course of treatment; and recommended medication andadministrationroute.
Datasynthesis/analysis
The searchstrategy of thedatabases identifieda totalof 356listedtitles.Eachabstractwasscreenedand344were excludedbecausetheydidnotmeettheinclusioncriteria. Twelvearticleswereeligibleforfullreview,andtheir refer-encelistsidentifiedonefurtherarticle.Atotalof13articles were therefore included in the qualitative synthesis, and theirfindingsweredescriptivelyanalyzed.5---17
Results
and
discussion
Table1describesthecharacteristicsofthetreatment guide-lines.Table2presentsuseofimmediate(‘‘STAT’’orstatim
[Latin]) anticonvulsant drug by type,dosing and route of administrationcoveredintheguidelines.Itisevidentthat theguidelinesdonotrecommendexactlythesamedosing for each anticonvulsant drug. However,these differences maybeduetoregionalpreference,history,orexperience. Developersofnewguidelinesshouldtakeintoaccountthe spreadindosingandthemaximarecommended,aswellas anynewclinicaldrugstudiesthatarepublishedafter2017.
Pre-hospitalmanagement
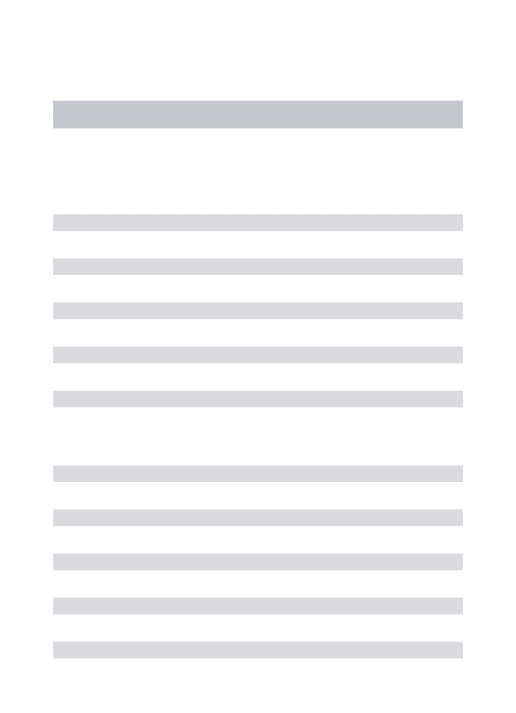
Six guidelines focused on EMS management.7,10---14 Fig. 1
presentsthealgorithmbytheEmergencyMedicalServices forChildren(EMSC)forcomparison.11Thisguidelineshould
beappliedtochildrenwithawitnessedseizurethatwasnot duetotrauma,andwasongoingatthetimeofarrivalofthe EMS.
Overall, all six guidelines recommended buccal mida-zolam or intranasal midazolam, and three recommended intramuscular midazolam.10,11,14 Five guidelines
recom-mended rectal diazepam as an option.7,10,12---14 A second
dose of benzodiazepine was recommended in two of the
guidelines, one at 5min11 and the other at 10min.13
All of the guidelines stated a preference for alternative non-intravenous routesof administration ratherthan gain intravenous access on arrival. Two of the guidelines11,13
recommended attempting to place either intravenous or intraosseous accessin specificsituations.Finally, onlyone of the guidelines providedcriteria for patienttransfer to ED.13
Commentonpre-hospitalEMSguidelines
Midazolamthroughthebuccalorintranasalroutewas rec-ommendedinthesixpre-hospitalguidelines.Thisguidance likelyreflectstheefficacyof midazolamversusdiazepam, and the ease of administration by these access routes. However,rectaldiazepamwasstillpresent inmostof the pre-hospital guidelines. Buccal midazolam is more effec-tivethanrectaldiazepamforstoppingseizuresandreducing their recurrence within 1h of onset, and as safe as rec-tal diazepam in relation to the incidence of respiratory depression.18 The effectiveness of intranasal midazolam
is similar to, or more effective than rectal diazepam. Intranasal midazolam also has a shorter drug administra-tiontimeandfasteractiontoseizurecessationthanrectal diazepam.Intranasalmidazolamiseasytoadminister,butit hasashort-lastingnasalirritanteffect.Asystematicreview demonstratedthatmidazolam,byanyroute,issuperiorin seizurecessationthandiazepam,byanyroute.19
Besidesefficacyandease ofadministration, thechoice ofnon-intravenousbenzodiazepinesdependsonlocal avail-ability,expertise,andpreference.Forexample,according to Osborne et al.,13 ambulances in the United Kingdom
did not carry midazolam, and soEMS staff would admin-ister the patient’s own buccal or intranasal midazolam, if available; otherwise, rectal diazepam would be used becauseofthedifficultygainingintravenousaccessin chil-dren. Forsimilarreasons, rectaldiazepamwascommonly available and recommended in theItalian LeagueAgainst Epilepsy pre-hospitalguideline.10 The World Health
Orga-nization(WHO)pediatricemergencytriageassessmentand treatment (ETAT)guideline14 recommends that,whenoral
and intranasal preparations of midazolam and lorazepam are not readily available, especially in resource-limited settings, the available intravenous preparations could be administered through the oral or intranasal routes. Last, intramuscularmidazolamwasrecommendedinthreeofthe sixguidelines.10,11,14Suchadministrationrequiresadditional
expertise, and it is effective and safe. For example, in the Rapid Anticonvulsant Medication Prior toArrival Trial (RAMPART), intramuscular midazolam was as effective as intravenouslorazepaminthepre-hospitalsetting.20Similar
ratesofendotrachealintubationandrecurrenceofseizures wereobservedinboththemidazolamandlorazepamgroups. Consideredtogether,alloftheguidelinesrecommendedthe non-intravenousrouteofadministration.
Two of the guidelines recommend attempting intra-venousorintraosseousaccessonlyinspecificsituations.11,13
TheEMSCalgorithm11intheUnitedStatesconsiders
Table1 Guidelineorprotocolcharacteristics.
Year,Ref# CountryorRegion Endorsedby Population(A,P) Scope
EMS ED
2014,11 USA EmergencyMedicalServicesforChildren P Y ---2015,13 UK JointRoyalCollegesAmbulanceLiaisonCommittee A,P Y ---2011,7 Canada CanadianPaediatricSocietyAcuteCareCommittee P Y Y
2013,10 Italy ItalianLeagueAgainstEpilepsy P Y Y
2014,12 India AssociationofChildNeurology(Indian) P Y Y
2016,14 Global WorldHealthOrganizationETAT P Y Y
2000,5 UK BritishPaediatricNeurologyAssociation P --- Y
2009,6 Aus/NZ PaediatricResearchinEDsInternationalCollaborative P --- Y
2012,8 USA NeurocriticalCareSociety A,P --- Y
2012,9 UK NHSNationalInstituteofHealthandCareExcellence A,P --- Y
2016,15 USA AmericanEpilepsySociety A,P --- Y
2016,16 Spain SpanishSocietyofNeurology A,P --- Y
2017,17 HongKong HongKongEpilepsySociety A,P --- Y
A,adult;P,pediatric;Aus/NZ,AustraliaandNewZealand;ED,EmergencyDepartment;EMS,EmergencyMedicalServices;ETAT,pediatric
emergencytriageassessmentandtreatment;NHS,NationalHealthService;UK,UnitedKingdom;USA,UnitedStatesofAmerica;Y,yes.
AmbulanceLiaisonCommittee(JRCALC)algorithm13
recom-mendsaseconddoseof diazepamiftheseizurecontinues after rectal diazepam, and that must be given via the intravenousorintraosseousroute.Establishingintravenous accesscouldbedifficult,however,inachildwithanongoing seizureinthepre-hospitalsetting.Itrequires trainedEMS providersandequipment,whichmaybelackingin resource-limited settings (see ETAT guideline14). Furthermore, the
seizure may stop before intravenous access is obtained, making the procedure unnecessary11; the time needed to
set-up intravenous access may prolong the time at the sceneanddelaydrugadministration.13
Twooftheguidelinesrecommendedadministeringa sec-onddoseofbenzodiazepinesinthepre-hospitalsetting.11,13
Theotherfourguidelinesdidnotincludethisoption. Main-taining adequate airway, breathing, and circulation while thepatientistransferredtotheED,7,10,12,13aswellas
com-municating with the medical control center for advice, are recommended.11 One guideline provided guidance on
criteria for transfer to hospital. The JRCALC guideline13
recommendstransfertohospitalforchildrenunder1yearof age,caseswiththeirfirstseizureorfirstfebrileconvulsion, andcaseswithserialseizuresordifficultymonitoring.The JRCALCguideline13alsorecommendsatime-criticaltransfer
tothehospitalifanyofthefollowingarepresent:difficulty withairway,breathing,circulation,or disabilityproblems; seriousheadinjury;SEafterfailedtreatment;or,underlying infection.
Emergencydepartmentmanagement
Eleven guidelines focused on ED management.5---10,12,14---17
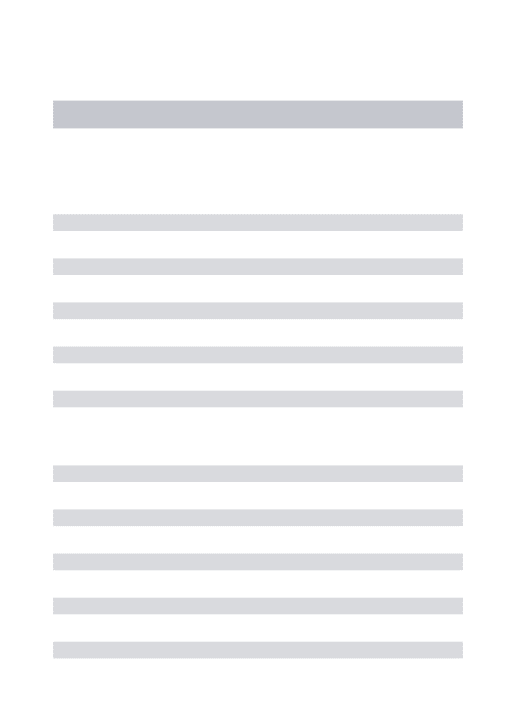
For comparison, the authors have selected the American Epilepsy Society (AES) algorithm for convulsive seizure lasting at least 5min.15 The structure of this algorithm
follows threephases of therapy (Figs. 2---4, and Table 3). The first phase of therapy is initial stabilization and the administration of a benzodiazepine. The second phase of therapy is the administrationof a non-benzodiazepine
second anticonvulsant drug, when benzodiazepines have failed.Thethirdphaseoftherapyistheadministrationofa generalanestheticdrugunderintensivecaresupportwhen SE has become refractory to at least two anticonvulsant drugsfromthefirstandsecondtherapyphases.
The timetostarting eachphaseoftherapy wassimilar acrosstheguidelines.Inthe initialphaseoftherapy,nine oftheguidelinesreportedastarttimeequalto,orearlier thantheAESalgorithm.5---7,9,10,12,15---17Theonsetofthesecond
andthirdphasesoftherapywereequalto,orearlierthan, theAESstarttimesinfiveoftheguidelinesthatstatedthe starttime.5---7,12,15 Endotracheal intubation wasconsidered
inthestabilization phasein twooftheguidelines,8,15 and
inthecontextofrapid sequenceintubation infourofthe guidelines.5---7,9
In regard to the route of anticonvulsant drug admin-istration, intravenous access may be available after the pre-hospitalstageoftherapy(Fig.1).Whenthereisno intra-venous accessat the start of the ED stage of treatment, the guidelinesrecommend intraosseous access in the ini-tial(n=1)6or secondphaseoftreatment(n=2).5,7Inboth
ofthese phases, benzodiazepines andphenytoin couldbe administeredthroughtheintraosseousroute.
CommentonEDtimecourse
Nosignificantdiscrepancieswereobservedamongthe guide-lines in regard to the timing for starting each phase of anticonvulsant drug therapy. All guidelines recommended ‘‘startingtheclock’’whenaseizurelastslongerthan5min, whichcanbeassumed tobewheneveran activelyseizing patientarrivesintheED.Thistimepointisalsoconsistent withthenewILAEdefinitionandclassificationofSE.1Aminor
Table2 Commonlyusedimmediateanticonvulsantdrug,administrationrouteanddose.
Drug Administrationroute
Rectal Buccal(B)/Intranasal(N) Intraosseous
(IO)/Intramuscular(IM)
Intravenous
Diazepam Bolus Bolus Bolus
0.2---0.5mg/kg/dose15,17 IO:0.25mg/kg×2 doses6
0.15---0.2mg/kg×2
doses15,17
0.5mg/kg/dose5,6 0.2---0.3mg/kg×2
doses12
0.5mg/kg×2doses7 0.25mg/kg×2doses6
0.3mg/kg×2dose7
0.5mg/kg10
Maximumdose Maximumdose
10mg6;20mg15,17 <5year,5mg7;≥5year, 10mg7;10mg10,12,15,17
Lorazepam Bolus Bolus Bolus
0.1mg/kg×2doses7 B:0.1mg/kg×2
doses7,10
0.1mg/kg×2
doses5,7,10,12,15,17
Maximumdose Maximumdose Maximumdose
4mg7 B:2.5mg10;4mg7 4mg5,7,10,12,15,17
Midazolam Bolus Bolus Bolus
B:5---10mg17 IO:0.15mg/kg×2 doses6
0.15mg/kg×2doses6
IN:0.2mg/kg7 IM:0.15mg/kg×2 doses6
0.15to0.2mg/kg×2
doses12 IM:0.2mg/kg×2
doses7,10
0.2mg/kg×2doses10
Maximumdose Maximumdose IN:5mg/nostril7 IM:5mg10;13---40kg,
5mg15;>40kg,10mg15; 10mg17
Fosphenytoin (PE,phenytoin equivalents)
Bolus Bolus
IM:20mgPE/kg7 20mgPE/kg7,12,15 Maximumdose Maximumdose IM:1000mgPE7 1000mgPE7;1500mg
PE15
Phenytoin Bolus Bolus
IO:20mg/kg6 15---20mg/kg16,17 18mg/kg5 18---20mg/kg10 20mg/kg6,7,12 Maximumdose Maximumdose IO:1000mg7 1000mg11,16
Phenobarbital Bolus
Table2(Continued)
Drug Administrationroute
Rectal Buccal(B)/Intranasal(N) Intraosseous
(IO)/Intramuscular(IM)
Intravenous
Valproicacid Bolus
20mg/kg12 25---45mg/kg16 30---45mg/kg10 40mg/kg15,17 Maximumdose 1500mg10;3000mg15,17
Levetiracetam Bolus
20mg/kg16 20---30mg/kg12 60mg/kg15,17 Maximumdose 4500mg15,17
EDfirstphaseanticonvulsanttherapy
In regard to the choice of anticonvulsant drug treat-ment, a benzodiazepine was universally recommended in the initial phase of therapy (Fig. 2 and Table 3). Intravenous lorazepam was recommended in ten of the guidelines,5---10,12,14,15,17 followed by intravenous
diazepam in eight of the guidelines.6,7,10,12,14---17 If no
intravenous access was available, the most commonly recommended anticonvulsant drug was midazolam: intra-muscular midazolam (n=8),6---8,10,12,15---17 buccal midazolam
(n=8),6,7,9,10,12,15---17orintranasalmidazolam(n=5).6,7,12,15,16
As an alternative, rectal diazepam (n=7) was commonly recommended.5,7,8,12,15---17 A repeated dose of
benzodi-azepinewasrecommendedinfiveguidelines;fourofthem considered the pre-hospital dose received,6,7,9,10 while
the other excluded the pre-hospital dose.5 Intravenous
phenobarbitalwasrecommendedasanon-benzodiazepine alternativeintwooftheguidelines.8,15
CommentonEDfirstphaseanticonvulsanttherapy
Intravenouslorazepamand diazepamwerethemost com-monly recommended intravenous benzodiazepines in the first phaseof therapy. All except for one guideline (from theSpanishSocietyofNeurology)recommendedintravenous lorazepam.16 In Spain, in 2016, intravenous lorazepam
wasnotavailable;thus,intravenousclonazepamis recom-mended instead. Intravenous lorazepam or diazepam are efficacious and safetouse. Forexample, in one random-izedcontrolledtrial21comparingintravenouslorazepamand
intravenous diazepam,72.9% of the lorazepam group and 72.1% of the diazepam group had cessation of SE within 10minwithoutrecurrencewithin30min,withsimilarrates of assisted ventilation (17.6%in the lorazepamgroup and 16.0%inthediazepamgroup).Intheresource-limited set-ting,oneadditionalconsiderationwithlorazepamuseisthe needforrefrigerationofthedrug,becauseofitsdegradation athightemperature.Althoughbothintravenouslorazepam anddiazepamareincludedintheWHOmodellistofessential
medicines for children, the ETAT guideline recommends intravenousdiazepaminhightemperatureregionswithno refrigerationfacility.14
When a repeat dose of benzodiazepine is required becauseofanongoingseizure,fourofthe11guidelines6,7,9,10
recommendedtakingaccountof whetheranypre-hospital benzodiazepinedose(s)had been administered,sinceEMS dosing would affect the choice of next anticonvulsant drug. Interestingly, these four guidelines were published after 2008, which is when Chin et al.22 showed that in
community-onset childhood convulsive SE there was an association between no pre-hospital anticonvulsant drug treatment, or use of more than two doses of benzodi-azepines,andSElastingmorethan60min.Moreover,their study demonstrated that treatment with more than two dosesof benzodiazepines was associated withrespiratory depression.Only oneguideline, from2000,recommended excludingconsideration ofpriorEMS treatment,5 andthat
was on the basis of possible variability in pre-hospital dosing.
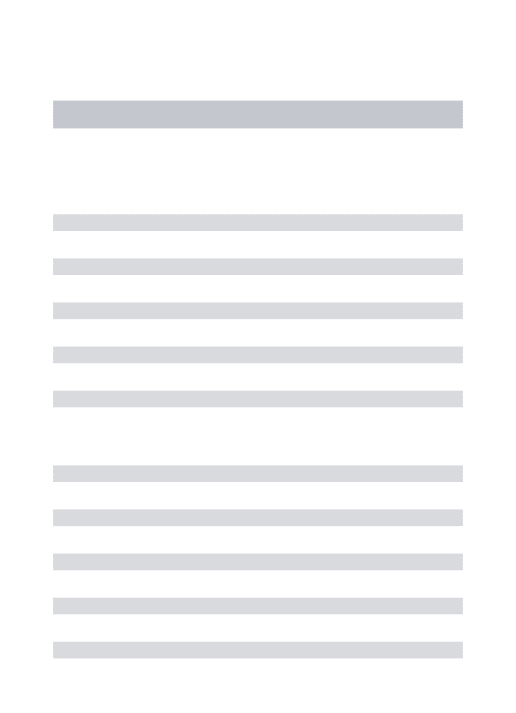
EDsecondphaseanticonvulsanttherapy
In the second phase of therapy (Fig. 3 and Table 3), guideline recommendations for intravenous medications included: phenytoin (n=10),5---10,12,14,16,17 phenobarbital
(n=9),6---10,14---17 valproic acid (n=6),8,10,14---17
fospheny-toin (n=4),7,12,14,15 and levetiracetam (n=4).8,15---17 If no
intravenous access was available, intraosseous pheny-toin was recommended in three guidelines,5---7 and the
otheroptionspresentedwereintramuscularfosphenytoin,7
phenobarbital,14andrectalparaldehyde.5,7
CommentonEDsecondphaseanticonvulsanttherapy
Pre-hospital EMS treatment
Variance (n=6)
No IV/IO access
1st midazolam
1st diazepam
1st lorazepam
2nd drug timing (2)
1st midazolam
2nd midazolam
2nd BDZ • R (5)
• B (1), R (2), IN (1), IM (1)
• 5 minutes (1) • Buccal
• or intranasal
• or intramuscular
• 10 minutes (1)
• B (6), IN (6), IM (3)
Timing
No IV/IO access
• Buccal
• or intranasal
• or intramuscular
• Midazolam
• or lorazepam EMS arrival
Seizure ongoing
Check BG & treat
No IV/IO access
5 minutes
IV present
call control
Transport to ED
Ongoing seizure or recurrent seizures
• or diazepam
Figure1 Pre-hospital EMStreatment.B, buccal;BDZ,benzodiazepine;BG, bloodglucose; ED,emergency department;EMS,
emergencymedicalsystem;IO,intraosseous;IN, intranasal;IM, intramuscular;IV,intravenous;R, rectal.Note:the numberin parenthesesisguidelines-out-of-sixinthiscategory(seetextfordetails).
guidelines.There area numberof reasons why fospheny-toinshould berecommended in preference tophenytoin: it does not require the excipient propylene glycol; it has less risk of hypotension and cardiac dysrhythmia; it does not cause the serious extravasation reaction, pur-ple glove syndrome; and, it can be administered via the intramuscular route when intravenous access is not available.7
Intravenousphenobarbitalwasrecommendedinnineof the11 guidelines.6---10,14---17 Ofnote, twoguidelines
recom-mended phenobarbital only if the patient had received phenytoin,9,16 the reasoning being that phenobarbital
has more depressant side effects than phenytoin (e.g., respiratorydepressionandsedation),especiallywhen ben-zodiazepineshavealreadybeenused.Theevidenceforusing intramuscularphenobarbitalis basedonpediatricpractice incerebralmalaria.23 Forexample,an intramusculardose
of 20mg/kg reduces seizure frequency, but it causes an increasedriskofrespiratorydepressionandmortality, espe-ciallyinthosewhohavealreadyreceivedmultipledosesof diazepam.23
Valproic acid was recommended in six of the 11 guidelines.8,10,14---17 Valproic acid may be hepatotoxic and
may lead to hyperammonemia. Three of the guidelines point out that it should be avoided or used withcaution in liver disease (or suspected metabolic disease) and in children younger than 2---3 years with uncertain seizure etiology.10,12,14 Valproic acid causes less hypotension or
respiratory depression when compared with phenytoin or
phenobarbital. For example, in a randomized controlled trial, although rapid intravenous loading of valproic acid stoppedseizuresinacomparableratetointravenous phe-nobarbital (90%versus 77%, nostatistical difference), the rate of adverse effects were lower (24% versus 74%); the phenobarbitalgroup experiencedmorelethargy,vomiting, orrespiratorydepression.24Incomparisonwithintravenous
phenytoin,valproic acidis aseffective in seizurecontrol, and better tolerated in regardto risk of hypotensionand respiratorydepression,butitdoescausemildelevationof liverenzymes.25 Takentogether,valproicacidcanbe
con-sideredaneffectiveoptionforsecondphaseanticonvulsant drugtherapy.
Levetiracetam was recommended in four of the 11 guidelines.8,15---17Ithastheadvantagesofgoodtolerability,
intravenous administrationoverrelatively shorttime,and absenceofhemodynamicandsedativeeffects.10
Nonethe-less, no randomized controlled trials of levetiracetam in pediatricconvulsiveSEhavebeenconducted.Arandomized, pilot open study has demonstrated equivalence of effec-tivenessinseizurecontrolwithlorazepam,andit hasless associatedrespiratorydepressionandhypotension.26
Variance (n=11)
Start time
0 min (4), 5 min (5)
No IV access
IV present 1st Midazolam
1st phase ED treatment
1st Diazepam
1st Lorazepam
• B (8), IN (5), IM (8), IO (1)
• R (7),IO (1) • or Diazepam (R)
• or, phenobarbital (IV)
• Midazolam (B,IN) • Midazolam (IM)
• or lorazepam
• or diazepam
• R (1), IO (1)
1st BDZ
• Lorazepam (10) • Lorazepam
• or Diazepam
• Diazepam (8)
• Midazolam (4)
• Clonazepam (1)
ED stabilization
ABCDEFG
Monitoring & IVA
5 minutes
Ongoing seizure or recurrent seizures
2nd BDZ Repeat therapy 1st BDZ 1st BDZ
Initial therapy Alternatives
20 minutes
Figure2 First-phaseEDtreatment.ABCDEFG,stabilizationsupportwithinterventionforAirway,Breathing,Circulation,Dextrose,
Essentialneurology,Fluids,Globalpicture;BDZ,benzodiazepine;ED,emergencydepartment;EMS,emergencymedicalsystem;IO, intraosseous;IN,intranasal;IM,intramuscular;IV,intravenous;IVA,intravenousaccess;R,rectal.Note:thenumberinparentheses isguidelines-out-of-11inthiscategory(seetextfordetails).
valproicacidforbenzodiazepine-refractorySE,andprovide informationoneffectivenessandsafetyinchildren.
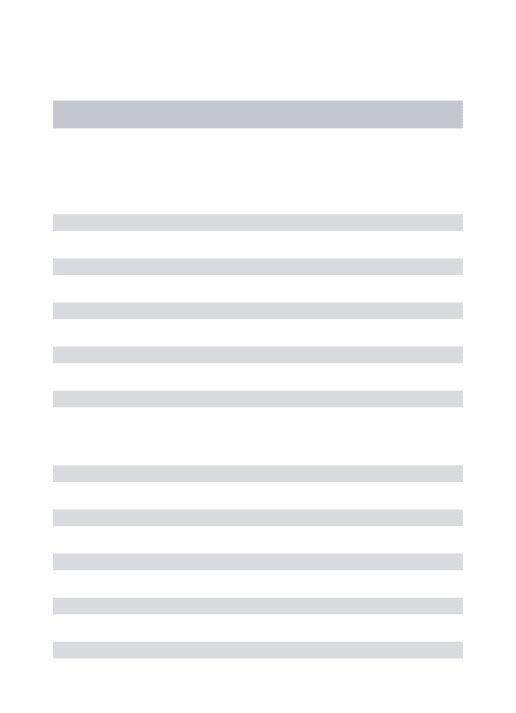
EDthirdphaseanticonvulsanttherapy
In the third phase of therapy (Fig. 4 and Table 3), four guidelines included the choice for repeating sec-ond phase therapy.7,10,12,15 Nine guidelines recommended
inducing anesthesia with thiopental5---9,12,15---17; all four of
the guidelines which recommended rapid sequence intu-bation suggested thiopental as the inducting agent.5---7,9
Seven of the guidelines recommended using mida-zolam infusion,7,8,10,12,15---17 six recommended propofol
infusion,6,8,10,15---17 and three recommended pentobarbital
infusion.7,8,15
CommentonEDthirdphaseanticonvulsanttherapy
At the time of starting the third phaseof anticonvulsant drug treatment, four of the 11 guidelines included the choiceforrepeatingsecondphasetherapy.7,10,12,15The
Cana-dian Pediatric Society Acute Care Committee guideline7
recommended a combination of using two second-phase drug therapies, each separated by a 5-minute interval, before proceeding to the induction of anesthesia. The Association of Child Neurology (India, 2013)12 guideline
groupconsideredthescenariowhennointensivecarebed
is available, and recommended the following before a midazolam infusion: either valproic acid and phenobarbi-tal,or levetiracetam. The Italian LeagueAgainst Epilepsy guideline10 recommendedvalproicacidaftersecondphase
therapy,ifdelayordifficultyinendotrachealintubationwas expected.
Finally, in regard to the choice of anesthetic agent, the guidelines do not have clear recommendations for preferencebetweenthiopental,midazolam,propofol,and pentobarbital.Rather,specificdrugselectionisdeferredto localexpertise.Itshouldbenoted,however,thatalthough propofolisusedinadultpracticeofrefractorySE,therisk ofpropofol infusion syndromein children is unacceptable and, therefore, continuous infusion is not recommended in a number of countries. In regard to the other anes-thetic agents, the data on intensive care treatment of pediatricrefractorySEareofpoorquality,yettheyshowa hierarchyinstrategies:earlymidazolambycontinuous infu-sion,then barbiturates,andthen trialof otheranesthetic therapies.27,28 Recently, a two-year prospective
observa-tional study assessed the use of continuous infusion of anestheticagentinpediatricpatients(agerange,1month to21years)withrefractorySEnotresponding totwo anti-convulsant drug classes.29 The United States PediatricSE
Variance (n=11)
Start time
• 10 minutes (3) • 20 minutes (2) • 25 minutes (2)
• IO (3), IM (f-PHT 1) • Fosphenytoin • or valproate • or levetiracetam • or phenobarbital • IM (1)
• R (2)
• phenytoin (10) • Phenobarbital (9) • Valproate (6) • Fosphenytoin (4) • Levetiracetam (4)
No IV access
IV present
Phenytoin (PHT)
Phenobarbital
Paraldehyde
2nd therapy
Single dose (IV)
Ongoing seizure or recurrent seizures
2nd phase ED treatment
20 minutes
40 minutes
Figure3 Second-phase EDtreatment. ED,emergency department; f-PHT,fosphenytoin; IO,intraosseous; IN, intranasal; IM,
intramuscular;IV,intravenous;R,rectal. Note:thenumber inparenthesesisguidelines-out-of-11inthiscategory(seetextfor details).
3rd phase ED treatment
Variance (n=11)
Start time
• 30 min (2) • 35 min (1) • 40 min (2) • 45 min (1)
• Thiopental (9)
• Thiopental • or midazolam
• ICU support • cEEG • or pentobarbital • or propofol
• Midazolam (7) • Propofol (6) • Pentobarbital (3)
Repeat 2nd therapy (4)
Repeat 2nd therapy
3rd therapy
Anesthesia
Anesthesia
See figure 3
40 minutes
60 minutes Monitoring
Ongoing status epilepticus
Figure4 Third-phaseEDtreatment.cEEG,continuouselectroencephalography;ED,emergencydepartment;ICU,intensivecare
unit.Note:thenumberinparenthesesisguidelines-out-of-11inthiscategory(seetextfordetails).
Conclusion
Managing a child who presents in an emergency with a seizureisachallenge;knowinghowtobestdealwithacute
interventions and follow-up is an important part of pedi-atricpractice.30 Guidelinesonanticonvulsantdrugtherapy
Table3 Comparisonofanticonvulsantdrugsusedineachofthethreephasesoftherapyandtheiradministrationroutes(see also,Tables1and2).
Year,Ref# Group First-phasetherapies Second-phasetherapies Third-phasetherapies
LZ DZ MZ PHT f-PHT PB VPA Lev Par TH MZ Pfl Pent
2000,5 BPNA iv r iv,io iv
2009,6 PREDICT iv,io iv,io im,b,in,io,iv iv,io iv iv iv 2011,7 CPS iv,r iv,r im,b,in,iv iv,io iv,im iv r iv iv iv
2012,8 NCS iv r im iv iv iv iv iv iv iv iv iv
2012,9 NICE iv b iv iv r iv
2013,10 LICE iv iv im,b iv iv iv iv iv iv
2014,12 AOCN iv iv,r im,b,in,iv iv iv iv
2016,14 WHO iv iv iv iv,im iv
2016,15 AES iv iv,r im,b,in iv iv iv iv iv iv iv iv
2016,16 SEN iv,r im,b,in,iv iv iv iv iv iv iv iv
2017,17 HKES iv iv,r im,b iv iv iv iv iv iv iv
Groups:AES,AmericanEpilepsySociety;AOCN,AssociationofChildNeurology(India);BPNA,BritishPaediatricNeurologyAssociation;
CPS,CanadianPaediatricSociety;HKES,HongKong EpilepsySociety; LICE,ItalianLeagueAgainstEpilepsy;NCS,NeurocriticalCare
Society;NICE,NationalHealthServiceNationalInstituteofHealthandCareExcellence;PREDICT,PaediatricResearchinEmergency
DepartmentsInternationalCollaborative;SEN,SpanishSocietyofNeurology;WHO,WorldHealthOrganization.Therapies:DZ,diazepam;
Lev,levetiracetam;LZ,lorazepam;MZ,midazolam;Par,paraldehyde;Pent,pentobarbital;PB,phenobarbital;f-PHT,fosphenytoin;PHT,
phenytoin;Pfl,propofol;TH,thiopental;VPA,valproicacid.Routes:b,buccal;im,intramuscular;in,intranasal;io,intraosseous;iv,
intravenous;r,rectal.
this qualitative systematic review of 13 regional/national guidelines,we have found thateach share similar frame-works for practice and time points. Different routes of benzodiazepine administration are feasible in the pre-hospital (EMS) and first phase of ED therapy. The choice of benzodiazepines depends on presence of intravenous access,localavailability,skillsofhealthcareproviders,and the resourcesetting. Valproic acid and levetiractamhave bettersideeffectprofilesthanphenytoinorfosphenytoin. Directcomparisonofeffectivenessandsafetyof different second phasetherapy for SE awaitsfurtherclinical study. Finally,regardingtheuseofanestheticagentsinchildren, mostoftheexperienceandliteratureisinusingmidazolam andthenpentobarbitalbycontinuousinfusion.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.TrinkaE,CockH,HesdorfferD,RossettiAO,SchefferIE,Shinnar S,etal.Adefinitionandclassificationofstatusepilepticus ---reportofILAEtaskforceonclassificationofstatusepilepticus. Epilepsia.2015;56:1515---23.
2.ProvisionalCommitteeonQualityImprovement,Subcommittee onFebrileSeizures.Practiceparameter:theneurodiagnostic evaluationofthechildwithafirstsimplefebrileseizure. Pedi-atrics.1996;97:769---75.
3.HirtzD,AshwalS,BergA, BettisD,CamfieldC,CamfieldD, etal.Practiceparameter:evaluatingafirstnonfebrileseizure inchildren:reportofthequalitystandardssubcommitteeofthe AmericanAcademyofNeurology,TheChildNeurologySociety, andTheAmericanEpilepsySociety.Neurology.2000;55:616---23.
4.MoherD,LiberatiA,TetzlaffJ,AltmanDG,ThePRISMAGroup. Preferredreporting items for systematic reviews and meta-analyses:thePRISMAstatement.PLoSMed.2009;6:e1000097.
5.AppletonR,ChoonaraI,MartlandT,PhillipsB,ScottR, White-houseW.Thestatusepilepticusworkingparty,membersofthe statusepilepticusworkingparty.Thetreatmentofconvulsive statusepilepticusinchildren.ArchDisChild.2000;83:415---9.
6.Babl FE, SheriffN,Borland M,Acworth J, NeutzeJ, Krieser D,etal.Emergencymanagementofpaediatricstatus epilep-ticus inAustralia and NewZealand:practice patternsinthe contextofclinicalpracticeguidelines.JPaediatrChildHealth. 2009;45:541---6.
7.FriedmanJ.Emergencymanagementofthepaediatricpatient withgeneralized convulsivestatusepilepticus.PaediatrChild Health.2011;16:91---104.
8.BrophyGM,BellR,ClaassenJ,AlldredgeB,BleckTP,GlauserT, etal.Guidelinesfortheevaluationandmanagementofstatus epilepticus.NeurocritCare.2012;17:3---23.
9.NationalInstitutefor HealthCareExcellence.Theepilepsies: thediagnosisandmanagementoftheepilepsiesinadultsand childreninprimary andsecondarycare.NICEClinical Guide-lines,No.137;2012.
10.CapovillaG,BeccariaF,BeghiE,MinicucciF,SartoriS,Vecchi M.Treatmentofconvulsivestatusepilepticusinchildhood: rec-ommendationsoftheItalianLeagueAgainstEpilepsy.Epilepsia. 2013;54:S23---34.
11.ShahMI,MaciasCG,DayanPS,WeikTS,BrownKM,FuchsSM, et al. An evidence-based guideline for pediatric prehospital seizuremanagementusingGRADEmethodology.PrehospEmerg Care.2014;S1:15---24.
12.MishraD,SharmaS,SankhyanN,KonankiR, KamateM, Kan-hereS,etal.Consensusguidelinesonmanagementofchildhood convulsivestatusepilepticus.IndianPediatr.2014;51:975---90.
13.Osborne A, Taylor L, Reuber M, Grunewald RA, Parkinson M, Dickson JM. Pre-hospital care after a seizure: evidence base and United Kingdom management guidelines. Seizure. 2015;24:82---7.
14.WorldHealthOrganization(WHO).Guideline:updateson pae-diatricemergency triage,assessmentand treatment:careof criticallyillchildren.Geneva:WHO;2016.
guide-linecommitteeoftheAmericanEpilepsySociety.EpilepsyCurr. 2016;16:48---61.
16.Mercade CerdaJM,Toledo ArganiM,Mauri LlerdaJA, Lopez GonzalezFJ,SalasPuigX,SanchoRiegerJ.TheSpanish Neu-rologicalSocietyofficialclinicalpracticeguidelinesinepilepsy. Neurologia.2016;31:121---9.
17.Fung EL, Fung BB. Review and update of the Hong Kong epilepsy guideline on status epilepticus. Hong Kong Med J. 2017;23:67---73.
18.McIntyreJ,RobertsonS,NorrisE,AppletonR,WhitehouseWP, PhillipsB,etal.Safetyandefficacyofbuccalmidazolamversus
rectaldiazepamforemergencytreatmentofseizuresin chil-dren:arandomisedcontrolledtrial.Lancet.2005;366:205---10.
19.McMullan J, Sasson C, Pancioli A, Silbergleit R. Midazolam
versus diazepam for the treatment of status epilepticus in childrenandyoungadults:ameta-analysis.AcadEmergMed. 2010;17:575---82.
20.SilbergleitR,DurkalskiV,LowensteinD,ConwitR,PancioliA, PaleschY,etal.Intramuscularversusintravenoustherapyfor prehospitalstatusepilepticus.NEnglJMed.2012;366:591---600.
21.ChamberlainJM,OkadaP,HolstiM,MahajanP,BrownKM,Vance C,etal.Lorazepamvsdiazepamforpediatricstatusepilepticus: arandomizedclinicaltrial.JAMA.2014;311:1652---60.
22.Chin RF, Neville BG, Peckham C, Wade A, Bedford H, Scott RC.Treatmentofcommunity-onset,childhoodconvulsive sta-tusepilepticus:aprospective,population-basedstudy.Lancet Neurol.2008;7:696---703.
23.CrawleyJ,WaruiruC,MithwaniS,MwangiI,WatkinsW,Ouma D, et al. Effect of phenobarbital on seizure frequency and
mortalityin childhood cerebralmalaria:a randomised, con-trolledinterventionstudy.Lancet.2000;355:701---6.
24.MalamiriRA,GhaempanahM,KhosroshahiN,NikkhahA, Bavar-ianB, Ashrafi MR.Efficacyand safetyofintravenous sodium valproateversus phenobarbitalin controllingconvulsive sta-tus epilepticus and acute prolonged convulsive seizures in children:arandomisedtrial.EurJPaediatrNeurol.2012;16: 536---41.
25.AgarwalP,KumarN,ChandraR,GuptaG,AntonyAR,GargN. Randomizedstudyofintravenous valproateandphenytoin in statusepilepticus.Seizure.2007;16:527---32.
26.MisraUK,KalitaJ,MauryaPK.Levetiracetamversuslorazepam instatusepilepticus:arandomized,openlabeledpilotstudy.J Neurol.2012;259:645---8.
27.WilksR,TaskerRC.Intensive caretreatmentofuncontrolled statusepilepticusinchildren:systematicliteraturesearchof midazolam and anesthetictherapies. Pediatr CritCare Med. 2014;15:632---9.
28.Tasker RC, Vitali SH. Continuous infusion, general anesthe-siaandotherintensivecaretreatmentforuncontrolledstatus epilepticus.CurrOpinPediatr.2014;26:682---9.
29.Tasker RC, Goodkin HP, Sanchez Fernandez I, Chapman KE, Abend NS, Arya R, et al. Refractory status epilepticus in children:intentiontotreatwithcontinuousinfusionsof mida-zolam and pentobarbital. Pediatr Crit Care Med. 2016;17: 968---75.