w w w . r b o . o r g . b r
Original
Article
Functional
and
radiographic
evaluation
and
quality
of
life
analysis
after
cementless
total
hip
arthroplasty
with
ceramic
bearings:
minimum
of
5
years
follow-up
夽
,
夽夽
Rafael
Borghi
Mortati
∗,
Rafael
Mota
Marins
dos
Santos,
Lucas
Borghi
Mortati,
Rodrigo
Angeli,
Ramon
Candeloro,
Richard
Armelin
Borger,
Roberto
Dantas
Queiroz
GrupodeQuadril,HospitalServidorPúblicoEstadualdeSãoPauloFranciscoMoratodeOliveira,InstitutodeAssistênciaMédicaao ServidorPúblicoEstadual,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received3April2012
Accepted17October2012
Keywords:
Arthroplasty Hip
Ceramic
Aluminumoxide
a
b
s
t
r
a
c
t
Objective:Theaimofthestudyistoanalyzeandcorrelatefunctionalandradiographicresults
andqualityoflifeinpatientsundergoingcementlesstotalhiparthroplastywithceramic
surface,performedatHospitalServidorPublicodeSaoPaulofrom2001to2006.
Methods:Weretrospectivelyanalyzed35hipstreatedwithcementlesstotalhiparthroplasty
withceramicsurfaceswithaminimumfollow-upof5years.Functionalevaluationwas
basedontheHarrisHipScore(HHS).Radiographicevaluationwasbasedonthemethod
proposedbyCharlesEnghforevaluationoffemoralosseointegrationandonDeLeeand
Charnleyzonesforacetabulum.QualityoflifewasassessedbySF-36questionnaire.
Results:TheHHSpresentedexcellentandgoodresultsin91%ofpatientspostoperatively
(mean of93.14pointsHHS).Asforradiographicevaluation, wefoundexcellent results
in100%ofevaluatedhips(provenosseointegration).SF-36scoreswerenotcomparedto
thecontrolgroupforthefollowingcomponents:pain,vitality,mentalhealthandsocial
aspects.ThedifferencebetweenHHSpreandpostoperativelyhadastatisticallysignificant
correlationwithphysicalfunctioningoftheSF-36.
Conclusion: Totalhiparthroplastywithceramicsurfaceisatreatmentthatenablesfunctional
improvementofthehipandincreasesqualityoflifeofpatientstolevelsclosetothoseof
peoplewithoutjointdiseases.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.Allrightsreserved.
夽Pleasecitethisarticleas:MortatiRB,dosSantosRMM,MortatiLB,AngeliR, CandeloroR,BorgerRA,etal.Avaliac¸ãofuncional,
radiográficaedaqualidadedevidaapósartroplastiatotaldequadrilnãocimentadacomsuperfíciecerâmica-cerâmica:seguimento
mínimodecincoanosdeevoluc¸ão.RevBrasOrtop.2013;48:505–511.
夽夽
WorkperformedatHospitalServidorPúblicoEstadualdeSãoPaulo“FranciscoMoratodeOliveira”,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:rafaelmortati@yahoo.com.br(R.B.Mortati).
2255-4971/$–seefrontmatter©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
Avaliac¸ão
funcional,
radiográfica
e
da
qualidade
de
vida
após
artroplastia
total
de
quadril
não
cimentada
com
superfície
cerâmica-cerâmica:
seguimento
mínimo
de
cinco
anos
de
evoluc¸ão
Palavras-chave:
Artroplastia Quadril Cerâmica
Óxidodealumínio
r
e
s
u
m
o
Objetivo: Analisarecorrelacionarosresultadosfuncionaiseradiográficoseograude
qual-idadedevidaempacientessubmetidosaartroplastiatotaldequadrilnãocimentadacom
superfícieemcerâmicafeitanoHospitalServidorPúblicoEstadualde2001a2006.
Métodos:Fizemosumestudoretrospectivoqueanalisou35quadristratadoscomartroplastia
totaldoquadrilnãocimentadacomsuperfícieemcerâmica,comtempodeseguimento
mínimodecincoanos.Aavaliac¸ãofuncionalbaseou-senoquestionáriodeHarrisHipScore
(HHS),aavaliac¸ãoradiográficabaseou-senométodopropostoporCharlesEnghparaofêmur
esinaisdeintegrac¸ãoósseanaszonasdeDeLeeeCharnleyparaoacetábuloeaavaliac¸ãoda
qualidadevidabaseou-senoquestionárioSF-36(MedicalOutcomes36ItemShort-FormHealth
Survey).
Resultados:OquestionárioHHSapresentouresultadosconsideradoscomoexcelentesebons
em91%dospacientesnopós-operatório(médiade93,14pontosHHS).Quantoàavaliac¸ão
radiográfica,em100%dosquadrisoperadostivemososteointegrac¸ãoósseacomprovada.
OsescoresdoSF-36nãoforamestatisticamentesignificantesemrelac¸ãoaogrupocontrole
paraosseguintescomponentes:dor,vitalidade,aspectossociaisesaúdemental.Avariac¸ão
entreoHHSpréepós-operatóriosecorrelacionacomacapacidadefuncionalnoSF-36.
Conclusão: Aartroplastiatotalcomsuperfíciedecerâmicaéumaoperac¸ãoquepossibilita
amelhoriafuncionaldoquadrileoaumentodaqualidadedevidadopacienteparaníveis
próximosaosdapopulac¸ãosemdoenc¸asdaarticulac¸ão.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier
EditoraLtda.Todososdireitosreservados.
Introduction
Themoderneraoftotalhiparthroplastybeganaround1958,
withSirJohnCharnley.Thisisanexcellenttreatmentmethod
forpainrelief andfunctionalimprovementamongpatients
withdegenerativehipdisease.1
Theunresolvedchallengeinhiparthroplastyistodevelop
contact surfaces that are able to withstand the higher
demands of younger and more active patients.2 Ceramics
startedtobeusedasprosthesesinthe1970sbyBoutinapud
Lustyetal.3 Betterresultshavealsobeenachievedthrough
improvementsintheceramicmanufacturingprocess.4
Theceramicsurfacescurrentlyinusearemadeofalumina
and/orzircon (Fig.1).Theyareextremelyhardand
scratch-resistant,andtheyprovidebetterlubricationandresistance
towear,incomparisonwithothersurfaces.5
Fig.1–Ceramicsurfacesmadeofaluminaandzircon.
Theaimofthepresentstudywastoanalyzethequalityof
lifeandfunctionalandradiographicresultsfromcementless
hiparthroplastywithceramicsurfaces.
Materials
and
methods
A retrospective study was conducted at Hospital Servidor
PúblicoEstadualdeSãoPaulo,inwhichpatientswere
clini-callyandradiographicallyevaluatedbetween2000and2006.
Inallcases,thepatientssignedafreeandinformedconsent
form.
Theinvestigationwasconductedonallthepatientswith
jointdegenerationwhoweretreatedsurgicallybymeansof
cementless hip arthroplasty withceramic surfaces. In this
sample,ethnicity,sexandsocialconditionwerenottakeninto
consideration.
Forty hips were selected. Five cases were subsequently
excluded:threethatwerelostfromthefollow-upandtwothat
didnotattendassessments.Inthepresentstudy,25patients
wereevaluated(35hips),comprising13menand12women
ofmeanage52years(range:36–66)andwithmeanlengthof
postoperativefollow-upofsixyearsandfourmonths.
Allthepatientswereevaluatedbeforeandafterthe
oper-ation bymeans of theHHS questionnaire,radiographically
according to the biological fixation of the acetabular and
femoralcomponentsandbymeansoftheSF-36questionnaire,
adaptedforthePortugueselanguage.
The HHS questionnaire, which was described in 1969
(Annex1),rangesfrom0to100points,withtheclassifications
Table1–ClassificationofHarrisHipScore questionnaire.6
HarrisHipScore Points
Excellent 90–100
Good 80–89
Moderate 70–79
Insufficient <70
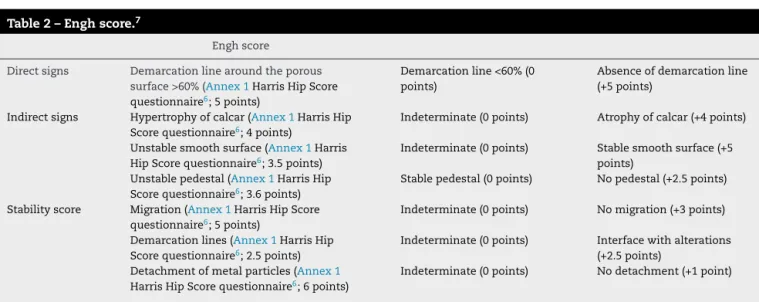
With regard to radiographic analysis, given that bone growth is the main stabilizer for cementless prostheses, weevaluatedthebiologicalfixationinaccordancewiththe methodproposedbyCharlesEngh(asshowninTable2)forthe
femoralcomponent,whichclassifiesthefixationasconfirmed
bonegrowth(morethan6points),probablebonegrowth(from
0to6points),stablefibrousencapsulation(0to10points)and,
lastly,unstable(lessthan10points).7Fortheacetabular
com-ponents,thecriterionforgoodboneintegrationthatweused
wastheabsenceorprogressionofaradiolucentline>2mm
intheDeLeeandCharnleyzones,absenceofmovementor
migrationofthecomponent,absenceofscrewbreakageand
absenceofmetalparticles.8Toevaluatethemigrationofthe
components,acomparativeassessmentofradiographs
pro-ducedwithatleastaone-year intervalbetween themwas
necessary.
Toanalyzequalityoflife,weusedtheSF-36.Thisisformed
by36 items that encompass eight components: functional
capacity,physicalaspects,pain,generalstateofhealth,
vital-ity, socialaspects,emotionalaspectsand mentalhealth. It
presentsafinalscorefrom0to100,inwhichzerocorresponds
totheworstgeneralstateand100tothebeststateofhealth.9
The results from the SF-36 questionnaire among the
patients underevaluation were compared with the results
fromacontrolgroupwithcharacteristicssimilartothoseof
oursample.Thecontrolgroupwasestablishedfromamong
healthy patients seen at the internal medicine outpatient
clinic, and was composed of 20 patients (10 men and 10
women)ofmeanage50years.
Theresultsobtainedwereexpressedasmeansand
min-imum and maximum values (quantitative variables) or by
absolutefrequenciesandpercentages(qualitativevariables).
TocomparetheHHSfrombeforetoaftertheoperation,the
Wilcoxontestwasused.Spearman’scorrelationwasusedto
investigatewhethertherewasanyrelationshipbetweenthe
SF-36andtheHHS.Thesignificancelevelusedwas5%.
Results
Beforetheoperation,themeanscorewasfoundtobe46points
(insufficient),asshowninTable3.Inthefinalevaluation,the
mean scorewas93points(excellent).Resultsconsideredto
beexcellentorgoodwerepresentedby91.4%ofthepatients
(Table4).
Accordingtotheradiographicassessmentmethodfor
con-firming bonegrowth proposed by Engh,all ofour patients
presentedprovenbonegrowth(meanof17points)(Table5).
Fortheacetabulum,wedidnotfindanysignsofmigrationor
movementofthecomponents.Likewise,therewereno
break-agesofscrews,noradiolucentlinesthatwereprogressiveor
greaterthan2mm,andnometalparticles.
Innocasewasthereanysqueaking,loosening,signofwear,
osteolysis,debrisorbreakageofceramic(eitheratthetimeof
implantingthecomponentorlateron).
The means for the eight components of the SF-36 are
expressedinTable6.
A comparison of the results between male and female
patientsisshowninTable7.
CorrelationbetweenthepostoperativeHHSandSF-36did
notshowstatisticalsignificanceforanycomponentofthe
SF-36.However,therewasasignificantrelationshipbetweenthe
change in the HHSfrom before toafterthe operation and
thepatients’functional capacity.Therewasnorelationship
betweenthepreoperativeHHSandtheSF-36.
Discussion
Theresultsfromarthroplastyaretraditionallyexpressedas
ratesofmorbidity-mortality,postoperativecomplicationsand
prosthesiswear.However,withtheimprovementofimplants
andsurgicaltechniques,thesemeasurementsarelosingtheir
relevanceandmaynotreflecttherealbenefitsforpatients.
Table2–Enghscore.7
Enghscore
Directsigns Demarcationlinearoundtheporous surface>60%(Annex1HarrisHipScore questionnaire6;5points)
Demarcationline<60%(0 points)
Absenceofdemarcationline (+5points)
Indirectsigns Hypertrophyofcalcar(Annex1HarrisHip Scorequestionnaire6;4points)
Indeterminate(0points) Atrophyofcalcar(+4points)
Unstablesmoothsurface(Annex1Harris HipScorequestionnaire6;3.5points)
Indeterminate(0points) Stablesmoothsurface(+5 points)
Unstablepedestal(Annex1HarrisHip Scorequestionnaire6;3.6points)
Stablepedestal(0points) Nopedestal(+2.5points)
Stabilityscore Migration(Annex1HarrisHipScore questionnaire6;5points)
Indeterminate(0points) Nomigration(+3points)
Demarcationlines(Annex1HarrisHip Scorequestionnaire6;2.5points)
Indeterminate(0points) Interfacewithalterations (+2.5points)
Detachmentofmetalparticles(Annex1 HarrisHipScorequestionnaire6;6points)
Table3–Significantfunctionalimprovementaftertheoperation,inrelationtobeforetheoperation(p<0.05),accordingto
theHarrisscore.
Radiographicscore Minimumvalue Maximumvalue Mean pvalue
Beforeoperation(points) 21 65 46 <0.05
Afteroperation(points) 76 100 93
Table4–Absolutefrequenciesandpercentagesof resultsfromHarrisHipScorequestionnaire.
HarrisHipScore Absolutefrequency Relativefrequency
Excellent 24 68.6%
Good 8 22.8%
Moderate 3 8.6%
Insufficient 0 0%
Total 35 100%
Table5–Quantitativeresultsfromradiographicscore.
Radiographic score
Minimum value
Maximum value
Mean
Points 8 24 17
Thereisnowincreasinginterestamongresearchersin trans-forming the concepts of quality of life and joint function intoaquantitativemeasurementthatcouldbeusedin clini-caltrialsforcomparisonsbetweenpopulationsanddifferent diseases.9–11Inourstudy,weobservedasignificant
improve-ment in function, in comparing the HHS from before the
operation(46points)toaftertheoperation(93points).
Ourresultswereconsistentwiththestudy publishedby
Lustyetal.,3whoevaluated222arthroplastyprocedureswitha
minimumfollow-upoffiveyearsandmeanscoreof97points.
Yooetal.8evaluated93hipswithameanscoreof97points
accordingtotheHHS(meanlengthoffollow-upoffiveyears).
Hamadoucheetal.4evaluated45patientswhounderwent
the Boutinoperation,witha meanfollow-up of19.8years,
andfoundthat75%ofthecaseshadexcellentorgoodresults.
Table6–SF-36scoresofthepatientsandcontrolgroup.
SF-36 Groups Mean pvalue
Functionalcapacity Control 89.29 0.0007
Case 60.8
Limitationduetophysicalaspects Control 92.86 0.0175
Case 48
Pain Control 80.29 0.1754
Case 62.76
Generalstateofhealth Control 76.14 0.0071
Case 50.08
Vitality Control 75.71 0.1611
Case 62.4
Socialaspects Control 91.07 0.3702
Case 79.5
Limitationduetoemotionalaspect Control 100 0.023
Case 54.67
Mentalhealth Control 85.14 0.0921
Case 71.04
Table7–SF-36scoresofthemaleandfemalepatients.
SF-36 Sex Mean pvalue
Functionalcapacity Female 56.67 0.4059
Male 64.62
Limitationduetophysicalaspects Female 39.58 0.5382
Male 55.77
Pain Female 64.25 0.8517
Male 61.38
Generalstateofhealth Female 45.42 0.4371
Male 54.38
Vitality Female 59.58 0.6495
Male 65
Socialaspects Female 76.04 0.3702
Male 82.69
Limitationduetoemotionalaspect Female 61.11 0.4696
Male 48.72
Mentalhealth Female 68 0.4696
Fig.2–Radiographoftotalhiparthroplastywithceramic
surfaces,showingconfirmedboneintegration.
Amongourpatients,91.4%hadresultsthatwereconsidered
excellentorgood,althoughourmeanlengthoffollow-upwas
sixyearsandfourmonths.
Allthehipsevaluatedpresentedconfirmedbonegrowthfor
thefemoralandacetabularcomponents(Fig. 2),whichwas
alsoinlinewiththeliterature.Yooetal.evaluated93hips
withaminimumfollow-upoffiveyearsandobservedthatall
thehipsevaluatedpresentedconfirmedbonegrowthforboth
componentsoftheprosthesis.8
Regardingqualityoflife,severalstudieshaveshownhigher
scoresfor physicalhealth, suchas inrelation topain and
functional capacity, after hip arthroplasty. The largest and
fastestincreaseoccurredinrelationtopainscores,and
great-estprogresswas seenover thefirst sixmonths.When the
improvementinqualityoflifeislow,comorbiditiesshouldbe
takenintoconsideration.10–12
WilklundandRomanus13demonstratedthatpatientswho
underwenttotalhiparthroplastypresentedaquality-of-life
indexvaluesimilartothatofacontrolgroupwiththesame
ageandsexdistribution.
Inthepresentstudy,theSF-36scoreswerenotstatistically
significantinrelationtothecontrolgroupforthecomponents
ofpain,vitality,socialaspectsandmentalhealth.
NilsdotterandLohmander14didnotfindanydifferencesin
SF-36scoresbetweenmenandwomenaftertheoperation.In
thesamestudy,whenthepatientswereseparatedintotwo
groups(older and younger than 72 years), it was observed
thatthequality-of-lifescoresshowedsimilarimprovements,
exceptinrelationtophysicalcapacity.Theauthorsproposed
thatthemultiplecomorbiditiesofmoreelderlypatientsmight
explainthis.
Liebermanet al.15 attempted toestablish arelationship
betweentheHHSandtheSF-36.Theyfoundastrong
correla-tionbetweentheHHSandphysicalhealthcomponentsamong
menofallagesandamongwomenovertheageof65years.
Therewasapoorcorrelationwiththementalhealth
compo-nent,particularlyamongwomenyoungerthan65 years.In
comparisonwiththescoreforthenormalpopulation
subdi-videdaccordingtogenderandage,menundertheageof65
yearshadlowerphysicalhealthscores.Amongwomenofall
ages, thephysicalcomponentswere lowerthan inthe
nor-malpopulationofthesameageandsex,andthemostevident
differencewasamongwomenundertheageof65years.
Inthepresentstudy,therewerenosignificantdifferences
betweenthegenders.Theagerangeofthepatientsevaluated
wasnarrowandtheywereconsideredtoberelativelyyoung
fortotalhiparthroplasty.
Therelativelyyoungageofthepatientsevaluatedinthis
study,togetherwiththehighdemandsand expectationsof
these individuals, explainsthe difference insome
compo-nentsoftheSF-36thatwasfoundinrelationtothenormal
population,despitethegreatfunctionalimprovementshown
bytheHHS.
Conclusion
Weconductedafunctional,radiographicand quality-of-life
evaluationonpatientswithceramicimplants.Throughthese
implants,wehopedtoattendtoyoungerandolderpatients
withhigherdemands,andtoachievegreatersurvivalofthe
implant.Ourstudyallowstheinferencethatarthroplastywith
ceramicsurfacesisasurgicalprocedure thatenables
func-tionalimprovementofthehipandprovidesincreasedquality
oflifeforpatients,attaininglevelsclosetothoseofthe
popu-lationwithoutjointdiseases.
Thelimitationsofthisstudythatshouldbetakeninto
con-sideration are thatthis was aretrospective study and that
assessmentsonthepatientswereonlydoneonceafterthe
operation.
Theinitialresultshaveencouragedustocontinuewiththis
method,albeitwiththeprovisothatfurtherstudies willbe
neededinrelationtothismaterial,withalongerfollow-up.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Appendix
A.
HarrisHipScoreinstrument
I.Pain(44possible)
A)Noneorunknown44
B)Slight,occasional,withoutcompromisingactivities40
C)Mild,doesnotaffectpracticeofordinaryactivities;
rarely,moderatepainafterpracticingunusualactivities;
canusesimpleanalgesic30
E)Severe,activitiesgreatlylimited10
Appendix(Continued)
II.Function(47possible)
A)Gait(wayofwalking)(33possible)
1.Claudication(limping)
a)None11
b)Mild8
c)Moderate5
d)Severe0
2.Support
a)None11
b)Stickforlongwalks7
c)Stickformostofthetime5
d)Onecrutch3
e)Twosticks2
f)Twocrutches0
g)Unabletowalk0
(specifythereason: )
3.Distancecapableofwalking
a)Unlimited11
b)Sixblocks8
c)2–3blocks5
d)Onlyinsidethehome2
e)Bedandchair0
B)Activities(14possible)
1.Goingupanddownstairs
a)Usuallywithoutholdingontobannister4
b)Usuallyholdingontobannister2
c)Insomemanner1
d)Unabletogoupordownstairs0
Appendix(Continued)
2.Puttingonshowsandsocks
a)Easily4
b)Withdifficulty2
c)Unabletodoit0
3.Sitting
a)Sittingcomfortablyonanordinarychairforonehour5
b)Sittingonahighchairforhalfanhour3
c)Unabletositcomfortablyonanychair0
4.Takingpublictransport1
III.Thepatientisconsiderednottohavepointsof
deformity(4)whenthefollowingarepresented:
A)Contractureinflexionremainslessthan30◦
B)Contractureinfixedadductionislessthan10◦
C)Contractureinfixedinternalrotationinextensionis
lessthan10◦
D)Discrepancyinleglengthslessthan3.2centimeters
IV.Rangeofmotion(thevaluefortheindexiscalculated
bymultiplyingthedegreesofmovementpossiblein
eachrangebytherespectiveindex)
A.Flexion
0–45◦
×1.0
45–90◦
×0.6
90–100◦
×0.3
B.Abduction
0–15◦×0.8
15–20◦
×0.3
Morethan20◦
Appendix(Continued)
C.Externalrotationinextension
0–15×0.4
Morethan15◦
×0
D.Internalrotationinextension
Any×0
E.Adduction
0–15◦
×0.2
Todeterminethegeneralscoreforrangeofmotion,
multiplythegeneralscoreforrangeofmotionand
multiplythesumoftheindexvaluesby0.05.Register
theTrendelenburgtestaspositive,leveledorneutral.
r
e
f
e
r
e
n
c
e
s
1. SchwartsmannCR,BoschinLC.Quadrildoadulto.In:Herbert S,BarrosFilhoTEP,XavierR,PardiniJuniorA,editors. Ortopediaetraumatologia:princípioseprática.4.ed.Porto Alegre:Artmed;2009.p.407–42.
2. AlbuquerqueH,AlbuquerquePC.Artroplastiatotaldoquadril comprótesenãocimentada.RevBrasOrtop.
1993;28(8):589–96.
3. LustyPJ,TaiCC,Sew-HoyRP,WalterWL,WalterWK,ZicatBA. Third-generationalumina-on-aluminaceramicbearingsin cementlesstotalhiparthroplasty.JBoneJointSurgAm. 2007;89(12):2676–83.
4.HamadoucheM,BoutinP,DaussangeJ,BolanderME,SedelL. Alumina-on-aluminatotalhiparthroplasty:aminimum18.5 yearfollow-upstudy.JBoneJointSurgAm.2002;84(1):69–77.
5.HeiselC,SilvaM,SchmalzriedTP.Bearingsurfaceoptionsfor totalhipreplacementinyoungpatients.JBoneJointSurgAm. 2003;85(7):1366–79.
6.HarrisWH.Traumaticarthritisofthehipafterdislocation andacetabularfractures:treatmentbymoldarthroplasty.An end-resultstudyusinganewmethodofresultevaluation.J BoneJointSurgAm.1969;51(4):737–55.
7.CarvalhoPI,CarvalhoFilhoA,AvelarAD.Avaliac¸ão radiológicadafixac¸ãobiológicadoscomponentesfemorais nãocimentadosnasprótesestotaisdequadrilsegundo CharlesEngh.RevBrasOrtop.1993;28(6):375–83.
8.YooJJ,KimYM,YoonKS,KooKH,SongWS,KimHJ.
Alumina-on-aluminatotalhiparthroplasty:afive-year minimumfollow-upstudy.JBoneJointSurgAm. 2005;87(3):530–5.
9.CiconelliRM,FerrazMB,SantosW,MeinãoI,QuaresmaMR. Traduc¸ãoparaalínguaportuguesaevalidac¸ãodo
questionáriogenéricodeavaliac¸ãodequalidadedevida SF-36.RevBrasReumatol.1999;39(3):143–50.
10.EthgenO,BruyèreO,RichyF,DardennesC,ReginsterJY. Health-relatedqualityoflifeintotalhipandtotalknee arthroplasty:aqualitativeandsystematicreviewofthe literature.JBoneJointSurgAm.2004;86(5):963–74.
11.BusijaL,OsborneRH,NilsdotterA,BuchbinderR,RoosEM. MagnitudeandmeaningfulnessofchangeinSF-36scoresin fourtypesoforthopedicsurgery.HealthQualLifeOutcomes. 2008;6:55.
12.BaumannC,RatAC,OsnowyczG,MainardD,DelagoutteJP, CunyC,etal.Doclinicalpresentationandpre-operative qualityoflifepredictsatisfactionwithcareaftertotalhipor kneereplacement?JBoneJointSurgBr.2006;88(3):366–73.
13.WilklundI,RomanusB.Acomparisonofqualityoflifebefore andafterarthroplastyinpatientswhohadarthrosisofthe hipjoint.JBoneJointSurgAm.1991;73(5):765–9.
14.NilsdotterAK,LohmanderLS.Ageandwaitingtimeas predictorsofoutcomeaftertotalhipreplacementfor osteoarthritis.Rheumatology(Oxford).2002;41(11):1261–7.