w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Outcomes
in
relapsed
Hodgkin’s
lymphoma
treated
with
autologous
and
allogeneic
hematopoietic
cell
transplantation
at
the
Pontificia
Universidad
Católica
de
Chile
Pablo
Ramirez
∗,
Mauricio
Ocqueteau,
Alejandra
Rodriguez,
Maria
Jose
Garcia,
Mauricio
Sarmiento,
Daniel
Ernst,
Veronica
Jara,
Pablo
Bertin
DepartmentofHematologyOncology,SchoolofMedicine,PontificiaUniversidadCatólicadeChile,Santiago,Chile
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received2December2014 Accepted3February2015 Availableonline14April2015
Keywords: Hodgkindisease Relapse
Hematopoieticstemcell transplantation
a
b
s
t
r
a
c
t
Introduction:Hodgkin’s lymphoma is a highly curable disease. Autologous and reduced intensityallogeneichematopoieticcelltransplantationsarealternativestotreatrelapsed patients.Here,wereportontheresultsofoneserviceusingtheseprocedures.
Methods:Allpatientswhounderwenttransplantationsinourinstitutionbetween1996and 2014wereretrospectivelystudiedanddemographics,toxicitiesandsurvivalratewere ana-lyzed.
Results:Thisstudyevaluated24autologousandfivereducedintensityallogeneic transplan-tations:themedianagesofthepatientswere29and32years,respectively.Atthetimeof autologoustransplantation,tenpatientswereincompleteremission,ninehad chemosensi-tivediseasebutwerenotincompleteremission,threehadrefractorydiseaseandthestatus oftwoisunknown.Intheallogeneicgroup,twowereincompleteremissionandthreehad chemosensitivedisease.The5-yearoverallsurvivalafterautologoustransplantationwas 42%(66%patientswereincompleteremission,37%hadchemosensitivediseasewith incom-pleteremissionand0%hadrefractorydisease)and1-yearoverallsurvivalafterallogeneic transplantationwas80%.Transplant-relatedmortalitywas0%inpatientsconditionedwith theifosfamide/carboplatin/etoposide(ICE),carmustine/etoposide/cyclophosphamide(BEC) andcarmustine/etoposide/cytarabine/melphalan(BEAM)regimens,37%inpatients condi-tionedwithbusulfan-basedregimensand20%inallogeneictransplantations.
Conclusions:Hematopoietic cell transplantation for relapsed Hodgkin’s lymphoma is a potentiallycurativeprocedureespeciallyinpatientsincompleteremissionatthetimeof autologoustransplantations,andpossiblyafterallogeneictransplantations.Furtherstudies arenecessarytoclarifytheroleofallogeneictransplantationsinthetreatmentofrelapsed Hodgkin’slymphoma.
©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthorat:Lira85,Piso4,LaboratoriodeHematologia,Santiago,Chile.
E-mailaddress:[email protected](P.Ramirez). http://dx.doi.org/10.1016/j.bjhh.2015.03.011
Introduction
Hodgkin’sLymphoma (HL) isa highlycurable disease with chemotherapyandradiotherapy.1However,dependingon sev-eralriskfactorsandstageatdiagnosis,2,3agroupofpatients willrelapseduringthefollow-up.Severalstudieshaveshown that in patients with localized disease, depending on the levelofrisk,theprobabilityofrelapsevariesbetween10and 30% after treatment with the adriamycin, bleomycin, vin-blastineanddacarbazineregimen(ABVD)andradiotherapy.2 However, the relapse rate can be as high as 40–50% for patients with advanced disease.3 Several drugs are under study forthe treatment ofrelapsed/refractory patients but untilnow,noneofthemhavebeenabletoinducelong-term remission.4Inthesecases,onlyautologoushematopoieticcell transplantation (autoHCT) hasshowntoinduce long-term remission.
Tworandomizedstudieshaveshown asignificant bene-fitoffreedomfromsecondfailurebutnotonoverallsurvival (OS)whencomparingchemotherapyalonewithautoHCT.5,6 Ontheother hand,therole ofreduced intensityallogeneic HCT(alloRICHCT)hasbeencontroversialandseveralsmall studiesandcaseserieshavesuggestedapotent graft-versus-lymphoma(GVL)effectandalowerrelapseratecomparedto autoHCT,7althoughnodirectcomparisonsbetweenthetwo proceduresexist.Initialstudieswithmyeloablative condition-ingregimensshowedhightransplant-relatedmortality(TRM) andgraft-versus-hostdisease(GVHD)rates.8,9Morerecently, theuseofRICregimenshasbeenassociatedwithlowerTRM, however,theirroleinthetreatmentofrelapsedHLisnotvery clearyet, withsuggestions fortheir useincasesofrelapse afterauto HCT, failure to harvestautologouscells or early relapsesafter chemotherapy.7 Also,theuse of haploidenti-cal donorshas preliminary shown interesting results with extremelylowtoxicityandlowriskofGVHD,butmaintaining theGVLeffect.10
Herein the results of a cohort of patients with relapsed HL submitted to auto HCT and allo RIC HCT are reported.
Methods
Patients
Aretrospectiveanalysisofthe HCTdatabase atthe Pontif-iciaUniversidadCatolicadeChile,Santiagowasperformed, whichincludedpatientstransplantedbetween1996and2014. Demographic data, as well as date of diagnosis, date of transplant,typeofgraftandconditioningregimen,age, gen-der,remission status attransplant, number of CD34+ cells
infused,time toneutrophiland plateletengraftment, com-plications,cause ofdeath,time toevent (death orrelapse) andOS(timetolastfollow-up ordeath)wereobtained.For patientssubmittedto alloRIC HCT,the typeofGVHD pro-phylaxis,andgradeandtimetothediagnosisofGVHDwere alsoobtained.ThisstudywasapprovedbytheEthics Com-mitteeandbytheMedicalResearchCenterCommitteeofthe Hospital.
Mobilizationandleukapheresis
Two methods were used for autologous cell collection: chemomobilizationandchemotherapyfollowedbyfilgrastim (10g/kg/day)startingonDay+5afterchemotherapyuntilthe dayoftheleukapheresis(usually10–14daysafter chemother-apy) and filgrastim (10g/kg/day) alone for five days. The numberofCD34+ cellsintheperipheralbloodwascounted
byflowcytometrythedaybeforetheprogrammedcollection. Ifthequantitywas>20×106/L,collectionwasperformedto obtain a minimum of 2×106 CD34+ cells/kg. If the CD34+ countwas<20×106/L,adoseofplerixafor(0.24mg/kg)was administeredsubcutaneously9–11hbeforeanothercollection to target a minimumof 2×106 CD34+ cells/kg, withup to fiveconsecutiveleukapheresis.Forallogeneiccollections, fil-grastim(10g/kg/day)wasadministeredforfivedaysbefore collectionwithoutmeasuringtheCD34+cellsthedaybefore
collection.
Definitions
The type of response before the transplant was based on thecriteriaofChesonetal.11,12 dependingonthe availabil-ityofpositronemissiontomography-computedtomography (PET/CT)andthetimeofthetransplant.Theresponseswere categorizedascompleteresponse(CR),incompleteresponse with chemosensitive disease (non-CR CS) and incomplete response refractory tochemotherapy (non-CRR) according tothestratificationproposedbytheCenterforInternational Bloodand MarrowTransplant Research(CIBMTR)13 and the NationalMarrowDonorProgram(NMDP).14
Donor
selection,
conditioning
regimens,
prophylaxis
of
graft-versus-host
disease
and
infectious
diseases,
and
treatment
Afterthe decisiontotransplant wasmade,the majorityof patients insecond CR(CR2) or non-CRCS underwent auto HCTs.Patientsfromwhomitwasimpossibletocollectan ade-quatenumberofCD34+cells,non-CRRpatients,andthosein
thirdormoreremissionwithasuitabledonor(fullymatched or haploidenticalsiblingormatchedunrelateddonor)were recommendedforalloRICHCTs.
Conditioning regimens for auto HCT between 1996 and 2003includedbusulfan/melphalan/thiotepa(BMT)and busul-fan/etoposide/cyclophosphamide(BuEC);in2004theservice started using the ifosfamide/carboplatin/etoposide (ICE), carmustine/etoposide/cyclophosphamide(BEC)and carmus-tine/etoposide/cytarabine/melphalan (BEAM) regimens.Allo RICregimens includedfludarabine/melphalan(FluMel), and fludarabine/cyclophosphamide/totalbodyirradiationwithor withoutpost-transplantcyclophosphamide(asinthecaseof haploidenticaltransplants).
GVHD prophylaxis was made with cyclosporine/ methotrexate, or tacrolimus/methotrexate/post-transplant cyclophosphamide(forhaploidenticaltransplants).
-1untilDay+365,fluconazole(200mgQD)startingonDay -1untilDay+100andsulfametoxazoltrimetoprim(QD)three timesperweekstartingonneutrophilrecoveryuntilDay+365. Allthepatientswere keptinisolationroomswith high-efficiencyparticulateairfiltersandpositivepressureduring theneutropenicphaseofthetransplant.Theyweregivena neutropenicdietandreceivedfilgrastim(300gIV) starting onDay+5untilneutrophilengraftment.
Statistical
analysis
ThestatisticalanalysiswasperformedusingGraphPad ver-sion6.0f(GraphPadSoftware,Inc.LaJolla,CA,USA).Variables arereportedasnumbersandpercentages.OSwasmeasured fromtransplantationuntildeathbyanycause.Patientsaliveat thetimeofanalysiswerecensoredatthelastfollow-update. TRMwasdefinedasdeathwithnoevidenceofprogressionor relapseandwasmeasuredfromthedayoftransplantation. Deathafterdiseaseprogressionwastreatedasacompeting eventinthecalculationofTRM.Survivalcurves(OSandTRM) wereobtainedusingtheKaplan–Meiermethodandwere com-paredwiththeLog-RankTest.
Results
Populationcharacteristics
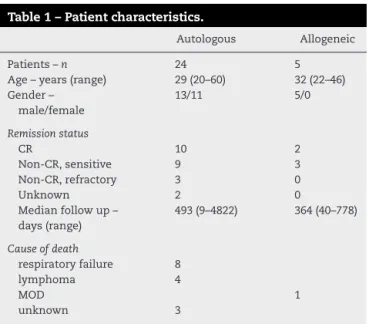
Between1996and201429HCTwereperformedforHL;24auto HCTandfivealloRICHCT.Themedianageforthe24auto HCTpatients, including13men(54%),was29years(range: 20–60years).AtthetimeoftheautoHCT,tenpatientswerein CR,ninewereinnon-CRCS,threeinnon-CRRandthestatus oftwowasunknown.ThemedianageforthealloRICHCT patientswas32years(range:22–46years),andallweremen; twoofthepatientswereinCRandthreewereinnon-CRCS (Table1).
Table1–Patientcharacteristics.
Autologous Allogeneic
Patients–n 24 5
Age–years(range) 29(20–60) 32(22–46)
Gender– male/female
13/11 5/0
Remissionstatus
CR 10 2
Non-CR,sensitive 9 3
Non-CR,refractory 3 0
Unknown 2 0
Medianfollowup– days(range)
493(9–4822) 364(40–778)
Causeofdeath
respiratoryfailure 8
lymphoma 4
MOD 1
unknown 3
CR:completeresponse;MOD:multipleorgandysfunction.
Transplantprocedure
Transplant characteristics are shown in Table2. Of all the
patientssubmittedtoautoHCT,12(50%)received condition-ing regimens based on busulfan. The rest of the patients (n=12)wereconditionedwiththeICE,BECorBEAMregimens. PatientssubmittedtoalloRICHCTwereallconditionedwith RICregimensasmentionedintheMethodssection.
The CD34+ cell doses in auto HCT and allo RIC HCT
were 2.87×106cells/kg (range: 1.51–16.9×106cells/kg) and 6.6×106cells/kg (range: 3.5–12×106cells/kg), respectively. MediannumberofapheresisrequiredfortheminimumCD34+
celldosewastwo(range:1–4)inautoHCTandoneinalloRIC HCT.
Themediantimetoneutrophilengraftmentwas11days (range:6–28days)with12days(range:8–29days)forplatelet engraftment inpatientswho underwentautoHCT. Patients submittedtoalloRICHCThadamediantimetoneutrophil engraftmentof13days(range:10–17days)with13days(range, 10–22days)toplateletengraftment.
Table2–Transplantcharacteristics.
Autologoustransplantation
Conditioningregimen
Bu/Mel/Tio 9
Bu/Eto/Cy 3
ICE 7
BEC 4
BEAM 1
CD34celldose–×106/kg(range) 2.87(1.51–16.9)
Numberofcollections–n(range) 2(1–4) Neutrophilengraftment–days(range) 11(6–28) Plateletengraftment–days(range) 12(8–29)
Allogeneictransplantation
Donor
Sibling6/6 2
Sibling3/6 1
Unrelated8/8 2
Conditioningregimen
Flu/Mel 2
Flu/Cy/TBI 2
Flu/Cy/TBI/Cy 1
CD34celldose–×106/kg(range) 6.6(3.5–12)
Numberofcollections–n(range) 1(1) Neutrophilengraftment–days(range) 13(10–17) Plateletengraftment–days(range) 13(10–22)
GVHDprevention–n
CS/MTX 4
TAC/MTX 1
GVHD–n(%)
Acute 2(40%)
chronic 1(33%)
Time after transplant (days)
% of patients
Overall survival
Allogeneic n=5 Autologous n=24 0 1000
0 20 40 60 80 100
2000 3000 4000 5000 6000
Figure1–Overallsurvivalafterautologousandallogeneic transplantation.
Graft-versus-hostdisease
InthealloRICHCTgroup,twooffivepatients(40%)hadGrade 2acuteGVHDoftheskin.Fromthreeevaluablepatients,one hadlocalizedchronicGVHD(33%)oftheliver,whichwas ade-quatelycontrolledbystandardimmunosuppression.
Survival
Median follow-up time in patients submitted to auto HCT was429days(range;9–4837days).Therewere11deathsdue mainly torespiratory failure and HL relapse (Table1). The 5-yearOS andprogressionfreesurvivalwere42%and 33%, respectively(Figure1).OS,accordingtoremissionstatus,was 66%inCRpatients,37%innon-CRCSand0%innon-CRR disease(p-value=0.03;Figure2).
Medianfollow-uptimeinpatientssubmittedtoalloRIC HCTwas364days(range:40–778days).Therewasonedeath shortly after transplant (Table 1). The 1-year OS was 80%
Time after transplant (days)
CR: Complete response; Non-CR CS: Incomplete response with chemosensitive disease; Non-CR R: Incomplete response refractory to chemotherapy
% of patients
No CR, refractory n=3
No CR, sensititve n=9 CR n=10
0 0 20 40 60 80 100
2000 4000 6000
Figure2–Overallsurvivalaccordingtoremissionstatusin autologoustransplantation.
CR:Completeresponse;Non-CRCS:Incompleteresponse withchemosensitivedisease;Non-CRR:Incomplete responserefractorytochemotherapy.
Time after transplant (days)
Auto: autologous hematopoietic cell transplantation; Allo RIC: reduced intensity allogeneic hematopoietic cell transplantation
% of patients
0 0 10 20 30 40 50
2000
Auto (ICE, BEC, BEAM) n=12 Allo RIC n=5
Auto (busulfan) n=12
4000 6000
Figure3–Transplant-relatedmortality.
Auto:autologoushematopoieticcelltransplantation;Allo RIC:reducedintensityallogeneichematopoieticcell transplantation.
(Figure1)andoffourevaluablepatients,onerelapsed (pro-gressionfreesurvival:75%).
Transplant-relatedmortality
Ofthepatientsconditionedwithbusulfanandsubmittedto autoHCT,four(37%)diedduetotransplant-related complica-tions(Figure3).OfthepatientswhounderwentalloRICHCT, oneoutoffivepatients(20%)diedduetotransplant-related complications(Figure3)
Discussion
HLisahighlycurablediseasewithchemotherapyand radio-therapy,butpatientswhorelapseorhaverefractorydisease areatherapeuticchallenge.Afterrelapse,thestandard
treat-mentisautoHCT5,6,15,16withabouthalfofthepatientsbeing
curedwiththisprocedure.Thisbenefithasbeenshownonly infreedomfromtreatmentfailurebutnotinOS.Ithasbeen suggestedthatthisisduetothepatientsinthe chemother-apyarm,whosubsequentlyreceivedanautoHCTwhenthey relapsedafterchemotherapy.Inourcohort,morethan60%of theautoHCTpatientswerelivingfiveyearsaftertransplant. However,theremissionstatusatthetimeofthetransplantis importantsincepatientsnotinCRhadsignificantlyworseOS thanCRpatients.SimilardatawerereportedbyLazarusetal. wherepatientsinCRhadanOScloseto80%comparedto60% inpatientswithpartialresponseand40%inthosewith refrac-torydisease.17 Inarecentpublication byJostling etal., the authorsalsoshowedthattheOSwascloseto80%inpatients withoutriskfactorscomparedto10%inpatientswiththree riskfactorsatthetimeoftransplant.18
cancers with total body irradiation, this procedure is not includedinthepreparationfortransplantinourservice.19In ourgrouptherewasnostandardcriteriontoselectaspecific conditioningregimen,howeverrecently,theBEAMregimenis beingusedmoreoftenduetotheresultsofJostlingetal.18
AlloRICHCTwasperformedinthefewpatientsconsidered tobeathigh-risk, andwhohad failedtheCD34+ collection
orfor whombad disease control wasanticipated using an autoHCT.18 Consideringthedismalresultswith myeloabla-tive regimens mainly related to high TRM,20 only allo RIC HCTwasperformed.Althoughnorandomizedstudies com-parethesetwotypesoftransplants,severalcaseseriesand registryanalysessuggest thatinadvanceddiseasepatients the OS could beover 60% and the TRM lower than 10%.16 Moreover,the evidence suggests that the GVLeffect could besignificant,especiallyinpatientstransplantedearlyafter relapse.21,22Inthecurrentseries,althoughthenumberofallo RICHCTpatientswaslow(n=5),TRMwaslowand1-yearOS was80%,whichissimilartootherstudies.23,24Similarly,the incidenceofacuteandchronicGVHDinthispopulation,even thoughthenumberofpatientsislow,isinagreementwith previousreports.Despite thefact thattheresultswithallo RICHCTareencouraging,itsspecificroleinthemanagement ofrelapsedHLisnotclearanditisrecommendedtoinclude thesepatientsinclinicaltrials,wheneverpossible.25Recently, aPhaseIIstudysuggestedthathaploidenticaldonorscould offerbetterresultsthanmatchedsiblingdonors,withverylow TRMandGVHDrisk,andwithoutevidenceofanylossofthe GVLeffect10thusopeninganewalternativeforthesepatients. Themainproblemsofthecurrentstudyareits retrospec-tivenatureandthelownumberofpatients.However,thisis thefirsttransplantseriesforHLfromChileandthedataisin linewithinternationalseries.ApreviousstudybyPugaetal.26 reportedresultsonengraftmentandmucositisinthefirstten autoHCTperformedinthepublichealthsystem,wherethey includedsevenpatientswithHLwithdifferentresponserates beforetransplant.TheydidnotreportonOSorTRMsono comparisonscanbemade.
Conclusions
TheresultswithautoHCTinthisstudyaresimilartoprevious reports,especiallyemphasizingthehighcurabilityinpatients inCRbeforetransplantation.Also,theresultswithallo RIC HCTareencouragingregardingOSandTRMandareinline withinternationalseriesrememberingthatthefollow-upand numberofpatientsisstilllow.Otherstudieswillbenecessary tobetterestablishtheroleofalloRICHCTinthetreatmentof relapsedHL.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. SjöbergJ,HalthurC,KristinssonSY,LandgrenO,NygellUA, DickmanPW,etal.ProgressinHodgkinlymphoma:a
population-basedstudyonpatientsdiagnosedinSweden from1973–2009.Blood.2012;119(4):990–6.
2.ArmitageJO.Early-stageHodgkin’slymphoma.NEnglJMed. 2010;363(7):653–62.
3.HasencleverD,DiehlV.Aprognosticscoreforadvanced Hodgkin’sdisease.InternationalPrognosticFactorsProjecton AdvancedHodgkin’sDisease.NEnglJMed.
1998;339(21):1506–14.
4.YounesA.Noveltreatmentstrategiesforpatientswith relapsedclassicalHodgkinlymphoma.HematologyAmSoc HematolEducProgram.2009:507–19.
5.LinchDC,WinfieldD,GoldstoneAH,MoirD,HancockB, McMillanA,etal.Doseintensificationwithautologous bone-marrowtransplantationinrelapsedandresistant Hodgkin’sdisease:resultsofaBNLIrandomisedtrial.Lancet. 1993;341(8852):1051–4.
6.SchmitzN,PfistnerB,SextroM,SieberM,CarellaAM,Haenel M,etal.Aggressiveconventionalchemotherapycompared withhigh-dosechemotherapywithautologoushaemopoietic stem-celltransplantationforrelapsedchemosensitive Hodgkin’sdisease:arandomisedtrial.Lancet. 2002;359(9323):2065–71.
7.BriceP.ManagingrelapsedandrefractoryHodgkin lymphoma.BrJHaematol.2008;141(1):3–13.
8.GajewskiJL1,PhillipsGL,SobocinskiKA,ArmitageJO,GaleRP, ChamplinRE,etal.Bonemarrowtransplantsfrom
HLA-identicalsiblingsinadvancedHodgkin’sdisease.JClin Oncol.1996;14(2):572–8.
9.MilpiedN,FieldingAK,PearceRM,ErnstP,GoldstoneAH. Allogeneicbonemarrowtransplantisnotbetterthan autologoustransplantforpatientswithrelapsed Hodgkin’sdisease.EuropeanGroupforBloodandBone MarrowTransplantation.JClinOncol.1996;14(4): 1291–6.
10.RaiolaA,DominiettoA,VaraldoR,GhisoA,GalavernaF, BramantiS,etal.UnmanipulatedhaploidenticalBMT followingnon-myeloablativeconditioningand
post-transplantationCYforadvancedHodgkin’slymphoma. BoneMarrowTransplant.2014;49(2):190–4.
11.ChesonBD,PfistnerB,JuweidME,GascoyneRD,SpechtL, HorningSJ,etal.Revisedresponsecriteriaformalignant lymphoma.JClinOncol.2007;25(5):579–86.
12.ChesonBD,HorningSJ,CoiffierB,ShippMA,FisherRI, ConnorsJM,etal.Reportofaninternationalworkshopto standardizeresponsecriteriafornon-Hodgkin’slymphomas. NCISponsoredInternationalWorkingGroup.JClinOncol. 1999;17(4):1244.
13.CenterforInternationalBloodandMarrowTransplant Research(CIBMTR).Availablefrom:www.cibmtr.org[cited 02.12.14].
14.NationalMarrowDonorProgram®(NMDP).Availablefrom: www.bethematch.org[cited02.12.14].
15.EichenauerDA,EngertA,AndréM,FedericoM,IllidgeT, HutchingsM,etal.Hodgkin’slymphoma:ESMOClinical PracticeGuidelinesfordiagnosis,treatmentandfollow-up. AnnOncol.2014;25Suppl.3:iii70–5.
16.BartlettNL.TherapiesforrelapsedHodgkinlymphoma: transplantandnon-transplantapproachesincluding immunotherapy.HematolAmSocHematolEducProgram. 2005;24:5–51.
17.LazarusHM,LoberizaFRJr,ZhangMJ,ArmitageJO,BallenKK, BasheyA,etal.AutotransplantsforHodgkin’sdiseaseinfirst relapseorsecondremission:areportfromtheautologous bloodandmarrowtransplantregistry(ABMTR).BoneMarrow Transplant.2001;27(4):387–96.
18.JostingA,MüllerH,BorchmannP,BaarsJW,MetznerB, DöhnerH,etal.Doseintensityofchemotherapyinpatients withrelapsedHodgkin’slymphoma.JClinOncol.
19.SuredaA,ArranzR,IriondoA,CarrerasE,LahuertaJJ, García-CondeJ,etal.Autologousstem-celltransplantation forHodgkin’sdisease:resultsandprognosticfactorsin494 patientsfromtheGrupoEspanoldeLinfomas/Transplante AutologodeMedulaOseaSpanishCooperativeGroup.JClin Oncol.2001;19(5):1395–404.
20.PeniketAJ,RuizdeElviraMC,TaghipourG,CordonnierC, GluckmanE,deWitteT,etal.AnEBMTregistrymatched studyofallogeneicstemcelltransplantsforlymphoma: allogeneictransplantationisassociatedwithalowerrelapse ratebutahigherprocedure-relatedmortalityratethan autologoustransplantation.BoneMarrowTransplant. 2003;31(8):667–78.
21.GreavesPJ,GribbenJG.Demonstrationofdurablegraftversus lymphomaeffectsinHodgkin’slymphoma.JClinOncol. 2011;29(8):952–3.
22.PeggsKS,KayaniI,EdwardsN,KottaridisP,GoldstoneAH, LinchDC,etal.Donorlymphocyteinfusionsmodulate relapseriskinmixedchimerasandinducedurablesalvagein relapsedpatientsafterT-cell-depletedallogeneic
transplantationforHodgkin’slymphoma.JClinOncol. 2011;29(8):971–8.
23.SuredaA,CanalsC,ArranzR,CaballeroD,RiberaJM,BruneM, etal.Allogeneicstemcelltransplantationafterreduced intensityconditioninginpatientswithrelapsedorrefractory Hodgkin’slymphoma.ResultsoftheHDR-ALLOstudy–a prospectiveclinicaltrialbytheGrupoEspanolde Linfomas/TrasplantedeMedulaOsea(GEL/TAMO)andthe LymphomaWorkingPartyoftheEuropeanGroupforBlood andMarrowTransplantation.Haematologica.
2012;97(2):310–7.
24.SarinaB,CastagnaL,FarinaL,PatriarcaF,BenedettiF,Carella AM,etal.Allogeneictransplantationimprovestheoverall andprogression-freesurvivalofHodgkinlymphomapatients relapsingafterautologoustransplantation:aretrospective studybasedonthetimeofHLAtypinganddonoravailability. Blood.2010;115(18):3671–7.
25.KuruvillaJ,KeatingA,CrumpM.HowItreatrelapsedand refractoryHodgkinlymphoma.Blood.2011;117(16): 4208–17.