Thyroid ophthalmopathy revisited*
Oftalmopatia tireoidea revisitadaKarina Freitas Soares Machado1, Marcelo de Mattos Garcia1
Thyroid ophthalmopathy is an autoimmune orbital disorder closely associated with Graves’ disease, although both conditions may also occur isolatedly. Thyroid ophthalmopathy may precede, coincide or follow the thyroid dysfunction onset and may rarely occur in euthyroid and hypothyroid patients. The extraocular muscles are most frequently involved and become enlarged resulting in ophthalmoplegia and proptosis. Other relevant signs include palpebral retraction, conjuctival hyperemia and periorbitary edema. Visual loss may occur in association with compressive optic neuropathy at the orbital apex. Thyroid ophthalmopathy is characterized by inflammation, congestion, hypertrophy and fibrosis involving fat and the orbital muscles. The disease activity is divided into two phases: an acute or inflammatory phase and a second one corresponding to an inactive phase associated with fibrotic changes and fat infiltration of the retrobulbar tissues. The diagnosis is based on clinical findings and imaging methods are indicated in case of doubt or suspicion of optic neuropathy. Computed tomography and magnetic resonance imaging can confirm the diagnosis, allowing the evaluation of the critical region of the orbital apex. Magnetic resonance imaging is the method of choice considering the superior tissue contrast resolution, besides the capacity of evaluating the disease activity by means of long TR sequences and detecting inflammatory changes, with a relevant role in a timely therapeutic planning, which may improve the prognosis.
Keywords: Thyroid ophthalmopathy; Extraocular muscles; Magnetic resonance imaging; Computed tomog-raphy.
A oftalmopatia tireoidea é doença orbitária autoimune intimamente associada com o hipertireoidismo, porém podendo existir separadamente. Pode preceder, coincidir ou suceder o início da disfunção tireoidea, rara-mente ocorrendo em eutireoideos ou hipotireoideos. Os músculos extraoculares são os principais alvos aco-metidos e tornam-se aumentados de volume, determinando oftalmoplegia e proptose. Outros sinais impor-tantes incluem retração palpebral, hiperemia conjuntival e edema periorbitário. Perda visual pode ocorrer se há compressão do nervo óptico no ápice orbitário. A oftalmopatia tireoidea é caracterizada por inflamação, congestão, hipertrofia e fibrose da gordura e músculos orbitários. A atividade da doença é dividida em fase aguda ou inflamatória, seguida pela fase inativa associada com alterações fibróticas e infiltração gordurosa. O diagnóstico é clínico, e quando este é difícil ou se suspeita de neuropatia óptica os métodos de imagem são indicados. A tomografia computadorizada e a ressonância magnética podem confirmar o diagnóstico e avaliar a área crítica do ápice orbitário. A ressonância magnética é superior, em virtude da resolução tecidual e da sua capacidade de avaliar a atividade da doença (mediante sequências com TR longo) e detectar alte-rações inflamatórias, auxiliando o planejamento terapêutico no momento certo, melhorando o prognóstico. Unitermos: Oftalmopatia tireoidea; Músculos extraoculares; Imagem por ressonância magnética; Tomogra-fia computadorizada.
Abstract
Resumo
* Study developed at Axial Centro de Imagem, Belo Horizonte, MG, Brazil.
1. Titular Members of Colégio Brasileiro de Radiologia e Diag-nóstico por Imagem (CBR), São Paulo, SP, MDs, Radiologists at Axial Centro de Imagem, Belo Horizonte, MG, Brazil.
Mailing address: Dr. Marcelo de Mattos Garcia. Avenida Ber-nardo Monteiro, 1472, Funcionários. Belo Horizonte, MG, Bra-zil, 30150-280. E-mail: [email protected] / ce@ axialmg.com.br
Received November 7, 2008. Accepted after revision March 23, 2009.
euthyroid and hypothyroid patients may be affected(3,4). In most of cases, the disease is
self-limited, and if a treatment is indicated, systemic corticoid therapy is the main strat-egy adopted(1).
Thyroid ophthalmopathy is the most fre-quent cause of orbital disease in the adult population, responsible for 15% to 28% of cases of unilateral exophthalmia and 80% of cases of bilateral exophthalmia(1,2).
The active phase of the disease is pro-gressive, lasting from several months to few years, usually from one to three years, with the inflammation settling to a more Machado KFS, Garcia MM. Thyroid ophthalmopathy revisited. Radiol Bras. 2009;42(4):261–266.
though both conditions may also occur isolatedly.
The most accepted theory to explain the association between thyroid ophthalmopa-thy and autoimmune ophthalmopa-thyroid disease com-prises a possible cross-reaction of sensi-tized T-lymphocytes and/or antibodies against common antigens for both the thy-roid and the orbita(1).
In a great number of cases, thyroid oph-thalmopathy may occur concomitantly with the onset of hyperthyroidism, but also it may precede or follow the onset of the thy-roid dysfunction(1,2), although in few cases
INTRODUCTION
al-quiescent or inactive phase characterized by the presence of fibrosis(2,5).
This disease is characterized by inflam-mation, congestion, hypertrophy, fat and orbital muscles fibrosis leading to increase in volume of these muscles(1).
Supplementary evaluation is performed with computed tomography (CT) and mag-netic resonance imaging (MRI) which plays a significant role in the demonstration and better characterization of a wide spec-trum of clinical findings.
CLINICAL AND IMAGING FINDINGS
The natural history of the disease is di-vided into an acute or inflammatory, pro-gressive phase histologically associated with lymphocytic infiltration and edema, followed by an inactive and fibrotic phase associated with fibrotic alterations and fat infiltration of retro-orbital tissues, particu-larly the extraocular muscles(4,5).
Usually, signs and symptoms of thyroid ophthalmopathy develop within one year after the thyroid dysfunction onset.
Extraocular muscles are most frequently involved by the immunological phenom-enon and, as a result, they present increase in volume which, in association with abnor-malities in the retro-orbital fat, determines ophthalmoplegia and proptosis(1,6). Other
relevant clinical signs determined by
inflam-matory alterations and/or vascular conges-tion include lower and upper eyelid retrac-tion (Figure 1), conjunctival hyperemia and periorbital edema(1,2), as well as sequelae
resulting from extraocular muscles hyper-trophy, such as visual loss resulting from corneal ulceration secondary to proptosis and optic neuropathy caused by optic nerve compression at the apex of the orbit(1,4,7,8). Nearly always, exophthalmia is bilateral and generally relatively symmetrical. The inferior rectus muscle is most frequently involved, followed by the medial rectus, superior rectus and lateral rectus muscles(1,2).
The disease diagnosis is based on clini-cal findings, and imaging methods are
in-dicated in cases where the diagnosis is du-bious or in the suspicion of optic neuropa-thy(2).
CT and MRI are useful methods for confirming the diagnosis by visualizing the orbital muscles and fat hypertrophy, and evaluating the critical region of the orbital apex(3). Many times, increased orbital fat
volume and resulting proptosis will be ob-served as the sole imaging finding(3) (Fig-ure 2).
Muscles involvement is typically ven-tral, sparing the tendinous insertions (Fig-ure 3), in association with other useful find-ing, i.e., hypodense foci at CT and hyper-intense foci on T2-weighted MRI,
involv-Figure 1. Patient with palpebral retraction at right (A). Note that proptosis is not present on the axial, FSE T2-weighted image (B).
A B
Figure 3. Axial CT image (A) showing the spindle-shaped thickening of the medial rectus muscles, with tendinous insertions sparing. Coronal FSE T2-weighted image (B) demonstrating an evident thickening of the inferior rectus muscle, with subtle hyperintense foci inside (arrows).
A
B
Figure 2. Fast-spin-echo, T2-weighted images in the axial (A) and coronal (B) planes demonstrating proptosis as a result of the increased presence of intraconal orbital fat. There is no involvement of extraocular muscles which present with a normal thickness.
A
ing the muscle bellies, probably because of inflammatory infiltrate (Figure 3).
Other imaging findings in the active or inflammatory phase of the disease include lacrimal gland hypertrophy and prolapse (Figure 4), palpebral edema, anterior dis-placement of the orbital septum. Optic nerve stretching and orbital bone wall re-modeling(1,3,9–11).
Extraocular muscles thickening can also be observed in other diseases that should be eventually considered in the differential
diagnosis; among them, orbital pseudo-tumor and lymphoproliferative processes. In these cases, unilateral involvement is most frequently observed without sparing the tendinous insertions(12). Additionally,
the clinical condition is usually associated with pain. Most rarely, orbital amyloidosis and metastatic neoplastic process can be mentioned, the latter being usually second-ary to breast neoplasm, in general with a nodular pattern(12).
Axial images are utilized to estimate the
proptosis degree, the volumetric increase of the medial and lateral rectus muscles (Fig-ure 5) and the relation between these muscles and the optic nerve. The optic nerve compression at the orbital apex also is best evaluated in the axial plane with the aid of coronal and sagittal images(10) (Figure 6).
The coronal plane is best for evaluating the inferior and superior recti muscles and the superior oblique muscle (Figure 7)(7,13).
The tomographic images are acquired in the axial and coronal planes, the first one
Figure 6. Sagittal CT image showing the optic nerve stretching resulting from prop-tosis and compression in the region of the orbital apex (arrow). Note the thickening of the inferior rectus muscle and the superior muscle complex.
Figure 7. Coronal FSE T2-weighted image demonstrating thickening of the extraocular muscles, including the superior oblique muscle.
Figure 5. Axial FSE T2-weighted image demonstrating thickening of the medial and lateral recti muscles.
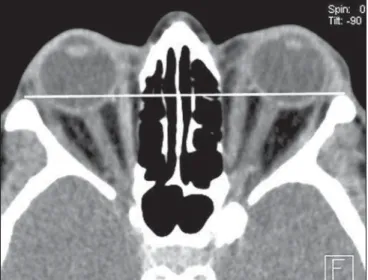
with an approximate angle of –10° to –15° in relation to the orbitomeatal plane, and the latter almost perpendicular to the axial plane. It is important to note that the risk for thyrotoxicosis should be taken into con-sideration in the utilization of computed tomography with iodinated contrast agents(4). The normal positioning of the
ocular globe is determined by a straight line connecting the zygomatic processes, utiliz-ing the median portion of the globe as a reference (interzygomatic line). The mea-surement of the ocular globe positioning is based on the distance between the inter-zygomatic line and the posterior margin on the median portion of the ocular globe in
the axial plane (Figure 8). The superior rec-tus muscle and the elevator muscle of the upper eyelid are measured in conjunction, considering that they cannot be easily dis-tinguished from each other, thus compris-ing the superior muscle group (Figure 9). Vertical diameters of the superior muscle
group and inferior rectus muscle can be best obtained in the coronal and sagittal planes (Figure 10). The horizontal diam-eters of the lateral and medial recti muscles are measured with higher reliability in the axial plane(14) (Table 1).
Figure 9. Coronal CT image demonstrating the measurement of the inferior rectus muscle and superior muscle complex.
Figure 10. SagittalCT image demonstrating the measurement of the inferior rectus muscle and superior muscle complex.
Positioning of the ocular globe in relation to the interzygomatic line (mm)
Medial rectus muscle thickness (mm)
Lateral rectus muscle thickness (mm)
Inferior rectus muscle thickness (mm)
Superior rectus muscle thickness (mm)
Normal
9.4 (5.9 to 12.8)
3.1 to 5.0
1.7 to 4.4
3.0 to 6.1
3.2 to 5.6
Table 1 Normal orbital measurements(13).
MRI is the best imaging method for evaluating the orbital structures because of its better tissue resolution and absence of ionizing radiation(15).
The protocol for examination with MRI in the author´s institution is comprised of spin-echo T1-weighted sequences in the axial and coronal planes, multiechoes T2-weighted sequence in the coronal plane, and short time inversion recovery (STIR) sequence in the coronal plane. Paramag-netic contrast-enhanced images are ac-quired with T1-weighted sequence with fat-suppression in the axial, coronal and sagittal oblique planes(16).
Normal extraocular muscles are charac-terized by low signal intensity on T1-Figure 8. Axial CT image
weighted sequences and low to intermedi-ate signal intensity on T2-weighted se-quences, with well-defined margins. There is a marked contrast enhancement, related to the great vascular supply to the extraocu-lar muscles (Figure 11)(1).
The T1-weighted sequence offers a bet-ter contrast resolution for evaluating the re-gion and measurement of the extraocular muscles(17), while the physiopathological
condition of these muscles is best evaluated on T2-weighted sequences(16).
Because of the capability to evaluate the water contents of tissues by means of long TR-weighted sequences with and without fat-suppression (respectively T2-weighted and STIR), MRI is a useful method for approaching the disease activity, identify-ing inflammatory and edematous alter-ations involving the muscles through an increase in the signal intensity on T2-weighted sequences, which is critical to achieve a good outcome of the anti-inflam-matory treatment whose effectiveness only can be achieve in the active phase of the disease(1,3,5–8,17,18). This information
cor-roborates the MRI’s superiority over other imaging methods in the follow-up of the disease progression.
Some authors describe a correlation be-tween the pattern of muscle involvement on T2-weighted sequences and the reversi-bility of diplopia. In cases where the
sig-nal intensity was uniformly increased, a better response to the treatment was ob-served, but, when the signal intensity was heterogeneous, the diplopia tended to be irreversible(19).
Hypertrophy of the extraocular muscles is observed and increase in their signal in-tensity on T2-weighted images indicates the edematous or inflammatory phase of the disease(18). On the other hand,
de-creased signal intensity of these muscles on T1- and T2-weighted sequences suggests the presence of chronic fibrotic alterations. Hyperintense intramuscular foci on T1- and T2-weighted sequences are suggestive of chronic fat degeneration(1,3,5), which also
can be identified at CT through hypoattenu-ating areas corresponding to fat infiltration (Figure 12). These latest findings indicate chronic, non-congestive phase of the dis-ease with restricted ocular motion second-ary to extraocular muscles fibrosis and sub-sequent loss of elasticity(3) in association
with volume decrease in these muscles(5)
corresponding to lack of response to the clinical treatment.
Surgical orbital decompression or ra-diotherapy may be indicated in the setting of compressive optic neuropathy to prevent a significant vision loss(12). The surgical
procedure is aimed at achieving orbital en-largement by means of a partial bone re-moval from one of the four orbital walls,
depending on the required decompression degree(20).
On images of all the extraocular muscles, the paramagnetic contrast enhancement has shown to be significantly decreased in pa-tients with thyroid ophthalmopathy at the edematous phase, while on T2-weighted images the signal intensity was increased, thus inferring a decrease in the vascular supply in the acute phase of this disease which, in the future, with the development of additional studies and improvement of MRI techniques, will probably allow the prediction of the severity, type of therapy and prognosis for the disease(1).
CONCLUSION
Imaging methods (CT and MRI) play a significant role as an aid in the evaluation of patients with endocrine ophthalmopathy, especially those with signs of optic neur-opathy, and in the demonstration of the wide spectrum of findings involving the orbital structures, both in the inflammatory and fibrotic phases of the disease.
MRI plays the most relevant role in the differentiation of the disease phases, allow-ing the detection of inflammatory signs indicative of the disease activity, which is important for selecting the patients eligible for anti-inflammatory therapy, with a great influence on the prognosis. Additionally, Figure 11. Axial SE T1-weighted image with fat suppression after
paramagnetic contrast injection: note the marked contrast uptake in all of the extraocular muscles.
MRI is the method of choice in the thera-peutic follow-up of these patients for evaluating the response translated into re-versal of inflammatory signs and conse-quential development of fibrosis and hy-pertrophy of extraocular muscles.
REFERENCES
1. Cakirer S, Cakirer D, Basak M, et al. Evaluation of extraocular muscles in the edematous phase of Graves ophthalmopathy on contrast-enhanced fat-suppressed magnetic resonance imaging. J Comput Assist Tomogr. 2004;28:80–6. 2. El-Kaissi S, Frauman AG, Wall JR.
Thyroid-as-sociated ophthalmopathy: a practical guide to classification, natural history and management. Intern Med J. 2004;34:482–91.
3. Mafee MF. Orbit: embryology, anatomy and pa-thology. In: Som PM, Curtin HD, editors. Head and neck imaging. 4th ed. St Louis: Mosby; 2003. p. 529–654.
4. Fung S, Malhotra R, Selva D. Thyroid orbito-pathy. Aust Fam Physician. 2003;31:615–20. 5. Yokoyama N, Nagataki S, Uetani M, et al. Role
of magnetic resonance imaging in the assessment of disease activity in thyroid-associated ophthal-mopathy. Thyroid. 2002;12:223–7.
6. Kahaly GJ. Recent developments in Graves’ oph-thalmopathy imaging. J Endocrinol Invest. 2004; 27:254–8.
7. Hosten N, Sander B, Cordes M, et al. Graves oph-thalmopathy: MR imaging of the orbits. Radiol-ogy. 1989;172:759–62.
8. Mayer EJ, Fox DL, Herdman G, et al. Signal in-tensity, clinical activity and cross-sectional areas on MRI scans in thyroid eye disease. Eur J Radiol. 2005;56:20–4.
9. Nugent RA, Belkin RI, Neigel JM, et al. Graves orbitopathy: correlation of CT and clinical find-ings. Radiology. 1990;177:675–82.
10. So NMC, Lam WWM, Cheng G, et al. Assessment of optic nerve compression in Graves’ ophthalmo-pathy. The usefulness of a quick T1-weighted se-quence. Acta Radiol. 2000;41:559–61. 11. Rothfus WE, Curtin HD. Extraocular muscle
en-largement: a CT review. Radiology. 1984;151: 677–81.
12. Parmar H, Ibrahim M. Extrathyroidal manifesta-tions of thyroid disease: thyroid ophthalmopathy. Neuroimaging Clin N Am. 2008;18:527–36. 13. Szucs-Farkas Z, Toth J, Balazs E, et al. Using
mor-phologic parameters of extraocular muscles for diagnosis and follow-up of Graves’ ophthalmo-pathy: diameters, areas, or volumes? AJR Am J Roentgenol. 2002;179:1005–10.
14. Ozgen A, Ariyurek M. Normative measurements
of orbital structures using CT. AJR Am J Roentgenol. 1998;170:1093–6.
15. Prummel MF, Gerding MN, Zonnevedl FW, et al. The usefulness of quantitative orbital magnetic resonance imaging in Graves’ ophthalmopathy. Clin Endocrinol (Oxf). 2001;54:205–9.
16. Majos A, Pajak M, Grzelak P, et al. Magnetic reso-nance evaluation of disease activity in Graves’ ophthalmopathy: T2-time and signal intensity of extraocular muscles. Med Sci Monit. 2007;13 Suppl 1:44–8.
17. Lennerstrand G, Tian S, Isberg B, et al. Magnetic resonance imaging and ultrasound measurements of extraocular muscles in thyroid-associated oph-thalmopathy at different stages of the disease. Acta Ophthalmol Scand. 2007;85:192–201.
18. Ohnishi T, Noguchi S, Murakami N, et al. Ex-traocular muscles in Graves ophthalmopathy: usefulness of T2 relaxation time measurements. Radiology. 1994;190:857–62.
19. Aydin K, Güven K, Sencer S, et al. A new MRI method for the quantitative evaluation of ex-traocular muscle size in thyroid ophthalmopathy. Neuroradiology. 2003;45:184–7.