rev bras ortop.2016;51(1):96–99
w w w . r b o . o r g . b r
Case
Report
Tendon
of
the
long
head
of
the
biceps
originating
from
the
rotator
cuff
–
An
uncommon
anatomical
variation:
case
report
夽
Carlos
Vicente
Andreoli
∗,
Leonardo
Roure
Esteves,
Eduardo
Figueiredo,
Paulo
Santoro
Belangero,
Alberto
de
Castro
Pochini,
Benno
Ejnisman
UniversidadeFederaldeSãoPaulo(Unifesp),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received31December2014
Accepted14January2015
Availableonline21December2015
Keywords:
Tendons Shoulder
Rotatorcuff
a
b
s
t
r
a
c
t
Anatomicalvariationsattheoriginofthebicepstendonhavebeendescribedbyseveral
authors,butoccurrencesofanorigininthesupraspinatusarerare.Itisunclearwhether
thisvariationmightcontributetowardpathologicalconditionsoftheshoulder.Ourobjective
herewastodescribeacaseofananatomicalvariationintheoriginofthetendonofthelong
headofthebiceps.
The clinicalinformation, preoperative images and arthroscopicimages relating to a
patientwithanaberrantoriginofthelongheadofthebiceps,whichwasobservedduring
shoulderarthroscopy,werereviewed.
Inthiscasestudy,theoriginofthebicepswasfoundintherotatorcuff,withoutany
originfromthesupraglenoidtubercleorupperlabrum.Thisvariantdidnotseemto
con-tributetowardthepathologicalconditionoftheshoulder,andstandardtreatmentforthe
concomitantconditionwassufficientfortreatingit.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.Allrightsreserved.
Tendão
da
cabec¸a
longa
do
bíceps
originado
do
manguito
rotador
–
Uma
variac¸ão
anatômica
incomum:
relato
de
caso
Palavras-chave:
Tendões Ombro
Bainharotadora
r
e
s
u
m
o
Asvariac¸õesanatômicasnaorigemdotendãodobícepsforamdescritasporváriosautores,
masaocorrênciadesuaorigemnosupraespinhalérara.Nãoestáclaroseessavariac¸ão
podecontribuirparacondic¸õespatológicasdoombro.Nossoobjetivoédescreverumcaso
deumavariac¸ãoanatômicadaorigemdacabec¸alongadotendãodobíceps.
夽
WorkperformedintheDisciplineofSportsMedicine,DepartmentofOrthopedicsandTraumatology,EscolaPaulistadeMedicina
(EPM),UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](C.V.Andreoli).
http://dx.doi.org/10.1016/j.rboe.2015.12.004
rev bras ortop.2016;51(1):96–99
97
Informac¸õesclínicas,imagenspré-operatóriaseimagensartroscópicasforamrevisadas
apartirdeumpacientequeteveumaorigemaberrantedacabec¸alongadobícepsobservada
duranteaartroscopiadoombro.
Nesteestudodecaso,aorigemdobícepsfoiencontradanomanguitorotador,semorigem
dotubérculosupraglenoidaloulabrumsuperior.Essavariantenãoparececontribuirparaa
patologiaombroeotratamentopadrãodepatologiaconcomitantefoisuficiente.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier
EditoraLtda.Todososdireitosreservados.
Introduction
Aseriesofdescriptionsoftheoriginofthetendonofthelong
headofthebicepshavebeenmade.Mostofthesestudieshave
describedanorigininthesupraglenoidtubercle.1,2 Recently,
many reports from anatomical dissections and findings of
arthroscopyhaveshownthatthetendonveryfrequently
ori-ginatesfromthesupraglenoidtubercleandtheupperglenoid
labrum.2
Vangsnesset al.2 observed that in around 50% oftheir
patients,thetendonofthelongheadofthebicepsoriginated
fromtheupperlabrumandinaround50%fromthe
supra-glenoidtubercle.
During normalembryo development, the tendon ofthe
bicepsdevelopsfromtheshouldercapsuleandcanbefoundas
anindependentstructureinfetusesagedaroundnineweeks.
Interruptionstodevelopmentorabnormalitiesoveritscourse
mayresultinvariationsfromthenormalanatomy.3
Therehavebeenseveraldescriptionsofanomalousorigins
ofthe tendon ofthe biceps, but their clinical implications
remainmostlyunknown.Thesereportscomefrom
inciden-talfindingsduringarthroscopicsurgeryandincludeaberrant
intra-articularorigins,extra-articularoriginsandagenesis.3–6
Theaimofthisarticlewastodescribeararevariationinthe
originofthelongheadofthebicepsandtheassociatedclinical
condition.
Case
report
Thepatientwasa43-year-oldmalemanualworkerwhohad
presentedpaininhisrightshoulder(dominantarm)fortwo
years,withprogressiveworseningwhileperforminghiswork.
Atthe timewhenhissymptomsbegan, hesought medical
adviceandwas diagnosedwithshoulderimpactsyndrome
(stage1,accordingtotheNeerclassification),basedon
physi-calexaminationandultrasonographyontheshoulder.Hewas
treatedwithan anti-inflammatorydrug (meloxicam,15mg
orallyfor10days)andwasreferredforphysiotherapeutic
reha-bilitation.Hecompleted50physiotherapysessions,witha50%
improvementofthepain.
One year after the first treatment, magnetic resonance
imagingshowedalesionthataffected40%ofthe
supraspina-tustendon.Theconservativetreatmentwascontinued,using
aninjectablecorticosteroid(threeintramuscularinjectionsof
dexamethasone,every15days)andphysiotherapeutic
reha-bilitation. After two years of treatment, he still presented
Fig.1–Coronalslicefrommagneticresonanceimaging,
highlightingtheanomalousoriginofthelongheadofthe
biceps.
positiveimpactmaneuvers(NeerandHawkins),withoutpain
on palpation of the bicipital groove, and with a negative
O’Brien test. Aradiographic examination showed atype II
acromion(Biglianiclassification).
A second magnetic resonance image revealed a bursal
lesionoccupying80%ofthethicknessofthesupraspinatus
tendon(Fig.1).Becauseofthepersistentpainandthepresence
ofalesionofthesupraspinatustendon,arthroscopicrepairof
therotatorcuffwasindicated.Duringthearthroscopic
proce-dure,avariationintheanatomicaloriginofthetendonofthe
longheadofthebicepswasobserved,suchthattheoriginwas
inthelowersurfaceofthesupraspinatustendon(Figs.2–4).
Thetendonofthebicepswasstableuponpalpationanddid
not present any signs ofinflammationor fibrillation along
itspath.Bursectomyandacromioplastywereperformedand
thelesionofthesupraspinatustendonwasrepairedusingan
absorbableanchor.
Noprocedurewasperformedonthetendonofthebiceps.
Thepatientreturnedtoworkfivemonthsaftertheoperation
andwasseentobeasymptomaticandperforminghisworkin
anormalmannerafter14monthsoffollow-up.
Discussion
Hymanand Warren7 describedanextra-articular originfor
thelongheadofthebicepsinthesupraspinatus.Kimetal.6
98
rev bras ortop.2016;51(1):96–99Fig.2–Arthroscopicimageshowingtheoriginofthelong
headofthebicepsonthelowersurfaceofthe
supraspinatustendon.
thebiceps,intherotatorcuff.InthevariantdescribedbyLang
etal.,8thebicepsoriginatedintherotatorheadwithoutan
annexgoingtotheupperlabrumandthiscasepresenteda
par-tialarticularlesionoftherotatorcuff.Theseauthorsobserved
thatthe biceps wasnotdiseased andthey thereforeleft it
intact.Theyreportedthatcompleteresolutionofthe
symp-tomswasachievedthrougharthroscopicrepairoftherotator
cuff.
Other intra-articular variants that have been described
includeabifurcatedoriginofthebicepsinthesupraglenoid
tubercleandposterosuperiorlabrum,atendonofthebiceps
bifiduswithasingleorigininthesupraglenoidtubercleand
atendonofthebicepsthatwentthroughthesupraspinatus
tendon.9 OgawaandNaniwa10 raisedthehypothesisthatif
thetendonofthebicepspassesthrough thesupraspinatus
tendon,thismaycontributetowardtearingoftherotatorcuff.
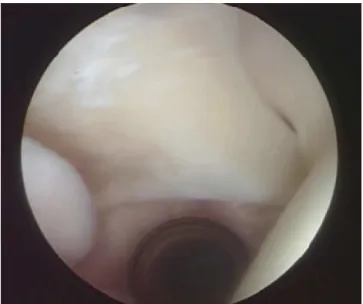
Fig.3–Anotherarthroscopicview,withtheprobeatthe
insertionofthebiceps.
Fig.4–Arthroscopicviewsof:(1)humeralhead;(2)upper
labrum;(3)originofthelongheadofthebiceps.
Enad4 presented two patients with a Y-shaped
bifur-catedorigininthesupraglenoidtubercleandposterosuperior
labrum.Therewasnoconnectionwiththerotatorcuff.Both
ofthesepatientsweretreatedforconditionsofsubacromial
impact and acromioclaviculararthrosis,bymeans ofdistal
decompression withdistalexcision ofthe clavicle.The
ori-ginofthebicepswasnotinflamedanddidnotappeartobe
diseased,anditwasleftintactinbothcases.
There is a consistent association between congenital
absence ofthe long head ofthe biceps and glenohumeral
instability,andstudieshaveshownthatthelongheadofthe
bicepshasastabilizingrole.8–10Specifically,thelongheadof
thebicepsactsasadepressoroftheheadofthehumerusand
adynamicstabilizerfortheglenohumeraljoint.
Ourcasereportandmostotherpublishedreportsoncases
ofabnormalintra-articularoriginsforthelong headofthe
bicepssuggest thattheseanatomicalvariationsare benign,
withoutanyevidencethatthesefindingsarepathological.
Inthisreportonararecase,wefoundadifferent
anatomi-caloriginforthelongheadofthebiceps,inwhichitoriginated
from the lower surface ofthe supraspinatus tendon,
with-out originatinginthesupraglenoidtubercleorintheupper
labrum.
Thisvariantdidnotappeartocontributetowardthe
patho-logicalconditionoftheshoulderandconcomitantstandard
treatmentfortheconditionwassufficienttoachieveaclinical
improvement.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
rev bras ortop.2016;51(1):96–99
99
2. VangsnessCTJr,JorgensonSS,WatsonT,JohnsonDL.The originofthelongheadofthebicepsfromthescapulaand glenoidlabrum–ananatomicalstudyof100shoulders.J BoneJointSurgBr.1994;76(6):951–4.
3. AudenaertEA,BarbaixEJ,VanHoonackerP,BerghsBM. Extraarticularvariantsofthelongheadofthebicepsbrachii: areminderofembryology.JShoulderElbowSurg.2008;17 Suppl.1:114S–7S.
4. EnadJG.Bifurcateoriginofthelongheadofthebiceps tendon.Arthroscopy.2004;20(10):1081–3.
5. KimKC,RheeKJ,ShinHD.Alongheadofthebicepstendon confluentwiththeintra-articularrotatorcuff:arthroscopic andMRarthrographicfindings.ArchOrthopTraumaSurg. 2009;129(3):311–4.
6.KimKC,RheeKJ,ShinHD,KimYM.Bicepslongheadtendon revisited:acasereportofsplittendonarisingfromsingle origin.ArchOrthopTraumaSurg.2008;128(5):495–8.
7.HymanJL,WarrenRF.Extra-articularoriginofbicepsbrachii. Arthroscopy.2001;17(7):E29.
8.LangJE,VinsonEN,BasamaniaCJ.Anomalousbicepstendon insertionintotherotatorcable:acasereport.JSurgOrthop Adv.2008;17(2):93–5.
9.GhalayiniSR,BoardTN,SrinivasanMS.Anatomicvariations inthelongheadofbiceps:contributiontoshoulder dysfunction.Arthroscopy.2007;23(9):1012–8.