Arq Neuropsiquiat r 2001;59(4):936-938
THROM BOLYTIC THERAPY FOR ACUTE
EXTRA-CRANIAL ARTERY DISSECTION
Report of t w o cases
Osama O. Zaidat
1, Jose Americo M . Fernandes Filho
1, Gurw ant Singh
1, Jose I. Suarez
1,2ABSTRACT - Ext ra-cranial art erial dissect ion account s f or 10% of st rokes in young people. Inf orm at ion on safet y of t hrombolyt ic administ rat ion in t his group is limit ed. The lit erat ure, how ever, does not favor use of t hrombolyt ics for myocardial ischemia w hen peripheral art erial dissect ion coexist s. Based on t he clinical and radiological f eat ures, t w o pat ient s w ho present ed w it h acut e st roke secondary t o art erial dissect ion w ere considered for t hrombolysis. One of t hem received int ra-venous recombinant t issue plasminogen act ivat or (rtPA), and the other patient received intra-arterial rtPA. There w ere no post thrombolysis complications. This report supports feasibility of administering thrombolytics in acute ischemic strokes resulting from extra-cranial arterial dissection. Future larger studies are necessary to determine the efficacy, safety and long-term outcome in t his pat ient populat ion.
KEY WORDS: t hrombolysis, st roke, dissect ion, int ernal carot id art ery.
Terapia trombolítica em dissecções arteriais cérvico-cefálicas agudas: relato de dois casos
RESUM O - Dissecção arterial cérvico-cefálica corresponde a 10 % dos acidentes vasculares cerebrais (AVC) em jovens. Informação sobre a segurança da administ ração de t rombolít icos nest e grupo é limit ada. A lit erat ura médica, entretanto, não favorece o uso de trombolíticos em isquemia miocárdica na coexistência de dissecção arterial periférica. Baseado nas características clínicas e radiológicas, dois pacientes com AVC agudo secundário a dissecção art erial f oram considerados para t erapia t rom bolít ica. Um deles recebeu rt PA int ravenoso e o out ro pacient e recebeu rt PA int ra-art erial. Não houve com plicações pós-t rom bólise. Est e relat o suport a a possibilidade do tratamento destes pacientes com terapia trombolítica. Estudos maiores são necessários para det erminar a eficácia, segurança e result ados a longo prazo nest a população de pacient es.
PALAVRAS-CHAVE: t rombólise, acident e vascular cerebral, dissecção, art éria carót ida int erna.
From t he Depart ment of Neurology1 & Neurosurgery2, Universit y Hospit als of Cleveland, Case West ern Reserve Universit y, Cleveland,
Ohio, USA. Present ed in part at t he XIX Brazilian Congress of Neurology, Salvador, BA. Oct ober 2000. Received 9 April 2001, received in final from 14 July 2001. Accept ed 25 July 2001.
Osama O. Zaidat, M D University Hospital of Cleveland / Department of Neurology 11100 Euclid Avenue / Fifth Floor Hanna House -Cleveland, OH 44106 USA. FAX 1 216/844-5066 . E-mail: [email protected] ru.edu
St rokes in young adult s result ing from spont
ane-ous dissect ion of t he cervical segm ent of t he ext
ra-cranial carotid artery are being reported w ith
increas-ing frequency
1-8. Ischemia may result from occlusion
of t he int ernal carot id art ery (ICA) and dist al st um p
em bolizat ion t o t he dist al int ra-cranial art eries, and
m ay account f or m ajor m orbidit y and m ort alit y in
young st roke vict ims. Ant icoagulat ion has been used
f or t his condit ion but caut ion has been advised due
t o t he risk of ext ending t he dissect ion
5. The lack of
t herapeut ic opt ions has been a lim it ing f act or f or
t he clinical recovery of st roke vict im s, unt il t he
ad-vent of t hrom bolyt ic t herapy. Experience is lim it ed
in t he use of t hrombolyt ics for acut e ischemic st rokes
result ing from acut e ext ra-cranial art erial dissect ion.
We report our experience w it h t w o pat ient s w ho
received t his t reat m ent .
CASES
ro-Arq Neuropsiquiat r 2001;59(4) 937
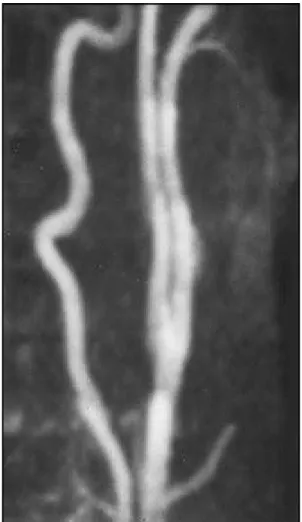
15 at 72 hours and t he pat ient w as discharged in st able condit ion. Nine mont hs lat er he w as independent and able t o w alk w it h braces w it h only som e w ord f inding dif f i-cult y. Follow -up m agnet ic resonance angiography (M RA) show ed part ial recanalizat ion of lef t ICA and M CA. One year lat er M RA of bot h int ra and ext racranial circulat ion w as norm al (Fig 3).
Case 2. 43-year old lef t -handed w om an w it h hist ory of dilat ed cardiom yopat hy present ed w it h lef t gaze pref e-rence and right hem iplegia of t hree hour durat ion. She also had right hom onym ous hem ianopsia, right hem ine-glect and hem ihypest hesia t o prim ary sensat ions (NIHSS of 27). Head CT scan w as norm al. She w as considered f or int ra-art erial t hrom bolysis, as approved by our IRB, since she present ed 3 hours af t er t he onset of sym pt om s. Her f am ily consent ed f or int ra-art erial t hrom bolysis w it h rt PA. Cerebral angiogram show ed lef t ICA dissect ion as w ell as a clot at t he bif urcat ion of t he lef t M CA and proxim al part of ant erior cerebral art ery (ACA). Throm bolysis w as administ ered w it h part ial recanalizat ion. There w ere no post -t hrom bolysis com plica-t ions. Hospi-t al and clinical course w ere unchanged, despit e im provem ent in NIHSS t o 23 on 72 hours exam inat ion. She rem ained dependent w it h se-vere disabilit y at 18 m ont hs f ollow up.
DISCUSSION
St rokes relat ed t o dissect ion of ext ra-cranial
cervi-cal arteries may range betw een 6.2% to 10% in young
adult s (less t han 40 years of age), w it h an est imat ed
annual incidence in t he Unit ed St at es of at least 2.6
per 100,000 persons
3. Abrupt onset of pain usually
localized t o t he head, face or neck is part of t he chief
complaint in more t han 60% of pat ient s
3, 6, and ult
i-m at ely resolve in 95% of pat ient s
8. Horner’s
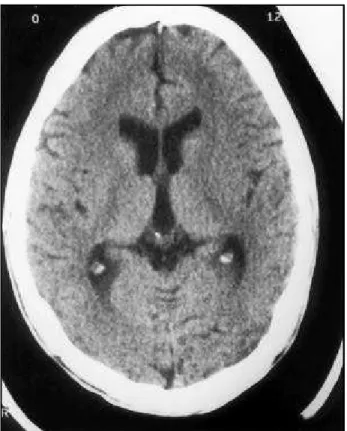
syn-Fig 1. Head CT scan pre thrombolysis w ithout intra-cranial hem-orrhage.
Fig 2. Angiogram demonstrating left internal carotid artery dissection w ith occlusion (left, arrow ). Poor collat-eral flow to left middle cerebral artery (right).
938 Arq Neuropsiquiat r 2001;59(4)
drom e ipsilat eral t o t he dissect ion is present in 14%
t o 58% of affect ed pat ient s
4. Signs of cerebral
is-chem ia are of t en delayed and w ill event ually occur
in 53% t o 90% of t he pat ient s
4. Wit h t he t urning
and ext ension of t he head, ICA is st ret ched over t he
lat eral art icular surf ace and t he pedicle of t he axis
vert ebra, result ing in injury t o t he vessel, and
usu-ally a hem orrhage w it hin t he m edia split s t he vessel
w all
3. Subint im al dissect ions t end t o cause narrow
-ing of t he art erial lum en, and subadvent it ial
dissec-t ions dissec-t end dissec-t o cause ardissec-t erial diladissec-t adissec-t ion
8. Dissect ion
of t en originat es 2 cm dist al t o t he bif urcat ion and
ext ends rost rally a variable dist ance t o t he base of
the skull
3. Exposure of the basement membrane leads
t o plat elet aggregat ion w it h t hrom bus f orm at ion.
Thrombi can be clinically occult , ext end and occlude
t he vessel, or em bolize
9,10.
Embolic st rokes in t he t errit ory of ICA are
associa-t ed w iassocia-t h high m orbidiassocia-t y and m orassocia-t aliassocia-t y, associa-t heref ore
ant icoagulat ion in t he presence of carot id
dissec-Fig 3. M RA of ext ra-cranial lef t int ernal carot id art ery reveals normal lumen 1 year later.
t ion seem s t o be a reasonable choice in t he acut e
phase of t he event . Endovascular t reat m ent s, such
as st ent placem ent , are an opt ion f or sym pt om at ic
pat ient s and have been used successfully
11. How ever,
t hey are st ill experiment al. For pat ient s w ho develop
st um p em boli in t he presence of art erial dissect ion,
t he role of t hrom bolyt ics is unclear. We t reat ed t w o
such pat ient s w it h spont aneous ICA dissect ion.
Pa-t ienPa-t one w ho w as only 21 years old received IV Pa-t PA
w it hin 3 hours of t he sym pt om onset , and had no
com plicat ions. Signif icant im provem ent w as seen
w it hin hours aft er t reat m ent and t he pat ient w as
independent at 9 m ont hs. The f irst pat ient w as
yo-unger t han t he second pat ient w ho received int
ra-art erial t PA w it hin 6 hours of t he sympt om onset ,
and w ho f ailed t o show any clinical im provem ent .
Neit her pat ient had com plicat ions relat ed t o t he
administ rat ion of t hrombolyt ic t herapy.
Our report suggest s t hat t hrom bolysis m ight be
feasible for acut e embolic st rokes result ing form
ar-t erial dissecar-t ion w iar-t houar-t causing w orsening of arar-t
e-rial w all t earing. The result s are in agreem ent w it h
Derex et al.
1and Jacobs et al.
9w ho suggest ed t hat
IV rt PA might be safe w hen given w it hin seven hours
and 3 hours of st roke onset respect ively, in presence
of cervicocerebral art ery dissect ion. No conclusion
can be draw n at t his t im e regarding t he saf et y and
ef f icacy of t hrom bolyt ic t herapy in t his clinical set
-t ing. Larger s-t udies are needed -t o clarify -t hese issues.
REFERENCES
1. Derex L, Nighoghossian N, Turjman F, et al. Intravenous tPA in acute ischemic stroke related to internal carotid artery dissection, Neurol-ogy 2000;54:2159-2161.
2. Bogousslavsky J, Despland PA, Regli F, et al. Spontaneous carotid dis-section with acute cortical stroke. Arch Neurol 1987;44:137-140. 3. Stahmer SA. Carotid and vertebral artery dissections. Emergency
Medi-cine Clinics of North America 1997;15:677-699.
4. Ast G, Woimant F, Georges B, et al. Spontaneous dissection of the in-ternal carotid artery in 68 patients. Eur J Med 1993;2:466-472. 5. Adams HP, Aschenbrener CA, Kassell NF, et al. Intracranial
hemor-rhage produced by spontaneous dissecting Intracranial aneurysm. Arch Neurol1982; 39:773-776.
6. Anson J, Crowell RM. Cervicocranial arterial dissection. Neurosurgery 1991;29:89-96.
7. Mokri B, Sundt TM Jr, Houser OW, Piepgras DG. Spontaneous dissec-tion of the cervical internal carotid artery. Ann Neurol1986; 19:126-138.
8. Luken MG III, Ascherl GF Jr, Correll JW, et al. Spontaneous dissecting aneurysms of the extracranial internal carotid artery. Clin Neurosurg 1979; 26:353-375.
9. Jacobs A, Rudolf J, Neveling M, et al. Systemic thrombolytic therapy of cerebro-cervical artery dissections: risk or benefit? [abstract]. Cerebrovas Dis 1999; 9(Suppl 1):100.
10. Rudolf J, Neveling M, Grond M, Schmulling S, et al. Stroke following internal carotid occlusion - a contraindication for intravenous throm-bolysis? Eur J Neurol 1999;6:51-55.