w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Molecular
and
hematologic
relapses
in
adult
patients
with
acute
promyelocytic
leukemia:
a
cohort
study
Ilana
de
Franc¸a
Azevedo
a,
Michelline
Gomes
Magalhães
b,
Fernanda
Ribeiro
Souto
b,
Washington
Batista
das
Neves
b,
Fárida
Coeli
de
Barros
Correia
Melo
b,
Eduardo
Magalhães
Rego
c,
Raul
Antônio
Morais
Melo
a,b,∗ aUniversidadedePernambuco(UPE),Recife,PE,BrazilbFundac¸ãodeHematologiaeHemoterapiadePernambuco(HEMOPE),Recife,PE,Brazil
cUniversidadedeSãoPaulo(USP),FaculdadedeMedicinadeRibeirãoPreto(FMRP),RibeirãoPreto,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received31August2015
Accepted9September2016
Availableonline21October2016
Keywords:
Acutepromyelocyticleukemia
Relapse Survival Monitoring
a
b
s
t
r
a
c
t
Objective:Toevaluatefactorspredictiveforrelapseinacohortofadultpatientswithacute
promyelocyticleukemiamonitoredbymolecularmethodsduringconsolidationandduring
atleastonemonthofmaintenancetherapy.
Methods:The charts andlaboratory dataof 65 adultpatientswith acutepromyelocytic
leukemia treated according to the International Consortium on Acute
Promyelo-cytic Leukemia 2006 protocol were reviewed. The identification of the promyelocytic
leukemia-retinoicacidreceptor-alphagenerearrangementatdiagnosis,post-induction,
post-consolidation and during maintenance treatment was performed by qualitative and
quantitativereversetranscriptionpolymerasechainreaction.
Results:Eighty-ninepatientswerediagnosedwith acutepromyelocyticleukemia overa
seven-yearperiodandofthese65wereeligiblefortreatmentwiththeprotocol.Among
the45patientswhoreceivedconsolidationandmaintenancetreatment,six(13%)relapsed,
threeofwhompresentedhematologicandthreepresentedmolecular relapse.Thefirst
relapsesoccurredatamedianof39months.Relapsedpatientswerefromallriskgroups
(low,intermediateandhigh)andbothmorphologicaltypes(M3andM3variant)werefound.
Threeofthesepatientsarealiveandinmolecularremissionaftersalvagetreatment.There
werenostatisticallysignificantdifferencesregardinggender,age,riskgroup,morphology,
promyelocyticleukemiabreakpointclusterregion,useofall-transretinoicacid,
develop-mentofdifferentiationsyndromeandnumberofdaystocompleteremissionbetweenthe
patientswhorelapsedandthosewhodidnot.
Conclusion:Ourresultsreinforcetheimportanceofprolongedmonitoringofacute
promy-elocyticleukemiapatientsusingmolecularmethodstodetectrelapseearly.
©2016Associac¸ ˜aoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published
byElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense
(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthorat:Fundac¸ãoHemope–LaboratóriodeBiologiaMolecular,RuaJoaquimNabuco,171-Grac¸as,52011-000Recife,PE,
Brazil.
E-mailaddress:[email protected](R.A.M.Melo).
http://dx.doi.org/10.1016/j.bjhh.2016.09.010
1516-8484/©2016Associac¸ ˜aoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.PublishedbyElsevierEditoraLtda.Thisisan
Introduction
Onceconsideredaleukemiawithpoorprognosis,currentlyby
meansofadequatetreatment,acutepromyelocyticleukemia
(APL) is highly curable, with remission rates of 90% and
disease-freesurvivalatsixyears ofover 80%.1 Despite the
increaseinoverallsurvival,casesofrelapsestilloccur and
need tobe promptly identified, thus allowing pre-emptive
treatmentinthecaseofmolecularrelapsesorre-induction
incasesofhematologicrelapse.2
The International Consortium on Acute Promyelocytic
Leukemia (IC-APL 2006) aimed to deploy a network of
National and International centers to improve diagnosis,
treatment, monitoring of treatment response and support
therapyandasaconsequencethesurvivalofpatientswith
APLindevelopingcountries.Thetreatmentwasbasedonthe
APL2005protocoloftheProgramaEspanholadeHematologia
(PETHEMA)group,adaptedtotherealityoftheparticipating
countries(Brazil,Mexico,Chile,Uruguay)withthe
substitu-tionoftheanthracyclineidarubicinfordaunorubicinwhichis
moreaffordableandiswidelyusedinthetreatmentofother
leukemias.3OftheeightBraziliancentersparticipatinginthe
IC-APL,thecenterofthisstudyistheonlyrepresentativeof
thenortheasternregionandincludedalmostonethirdofthe
patientsofthestudy.
TherecentlypublishedresultsoftheIC-APL3demonstrated
animprovementinearlymortalityratesandoverallsurvival
comparedwithhistorical controls.4 In thepresent study, a
cohortofpatientsdiagnosedwithAPLwasevaluatedforrisk
factorsassociatedwithrelapse.
Methods
Patients
Thisstudy retrospectively analyzed89 adultpatients
diag-nosedwithAPLbetweenJanuary2007andAugust2014atthe
HospitaloftheFundac¸ãodeHematologiaeHemoterapiade
Pernambuco(Hemope),Recife,Brazil.Clinicalandlaboratory
datawereobtainedfromthepatients’charts.Theprojectwas
approvedbytheResearchEthicsCommitteeoftheinstitution
(#028/2006)andwasconductedafterinformed consentwas
obtainedfromthepatients.
Diagnosisandmonitoring
Thediagnosiswasestablishedbyclinical,cytomorphological,
immunophenotypicand molecularcriteria.5 The
identifica-tion of the promyelocytic leukemia-retinoic acid receptor-alpha
(PML-RAR˛) gene rearrangementwas performed byreverse
transcription polymerase chain reaction (nested RT-PCR
and/orRT-qPCR)accordingtotheinternationalBIOMED-1and
BIOMED-2protocols.6,7SamplesforRT-qPCRweresenttothe
reference laboratory of the IC-APL study in the Faculdade
deMedicinadeRibeirãoPretodaUniversidadedeSãoPaulo
(FMRP-USP).
Molecular tests were performed using bone marrow
(BM) samples obtained at initialdiagnosis, post-induction,
post-consolidation (after the thirdcourse ofconsolidation)
and during maintenance. Standard monitoring
recom-mended tests every three and six months, respectively,
during maintenance and after treatment for up to two
years.
Definitions
Complete hematologic remission (CR) and relapse were
definedusingconventionalcriteria.8Hematologicrelapsewas
diagnosedbasedonthepresenceof>20%blastsorabnormal
promyelocytesinthebonemarrowany timeafter
hemato-logicremission.Molecular remission(MR)wasdefinedasa
negativeRT-PCRresultofbonemarrowcellsafterthethird
and lastcycle ofconsolidation.9 Molecularpersistence was
definedasPCRpositivityintwoconsecutiveBMsamples
col-lected within a minimal interval of 15 days afterthe end
ofconsolidation therapy. Molecular relapse was definedas
thereappearanceofthePML-RAR˛-specificbandintwo
con-secutive BM samples collected at an interval of 15 days
atanytimeafterconsolidationtherapy.3,10 Arbitrarily,early
relapsewasdefinedasthatoccurringwithintwoyearsafter
proven CRand late relapse beyond this period.11
Differen-tiation syndrome (DS) was defined according to standard
criteria.12,13
Treatment
Thestandardtreatmentprotocol usedwas theIC-APL2006
with patients being categorized according to the risk of
relapseasdescribedelsewhere.3,9,14,15Thetreatmentoptions
of the relapsed cases included re-induction with all-trans
retinoic acid (ATRA), chemotherapy and arsenic trioxide
(ATO)followedbystemcelltransplantation (SCT)whenever
possible.2,16–18
Statisticalanalysis
StatisticalanalysiswasperformedusingtheStata12.0
soft-ware.Thet-testwasusedtocomparethegroupsregardingage,
daystoCR,andmonthsoffollowup.Fisher’sexacttestwas
usedforcategoricalvariables(gender,riskofrelapse,
morphol-ogyandtypeoftranscript).Relativerisk(RR)wascalculated
witha95%confidenceinterval(95%CI).p-Values<0.05were
consideredstatisticallysignificant.
Results
Eighty-nine patients were diagnosed with APL during the
periodandofthese,65wereeligiblefortreatmentusingthe
IC-APL2006protocol.Themedianageatinitialdiagnosisofthe
relapsedpatientswas37.5years(range:24–46years).
Hemato-logicremissionwasachievedwithamedianof32days(range:
27–56days).
As themainpurpose ofthis study wasto evaluate
fac-tors predictive for relapse, analysis was restricted to the
45 patients who achieved remission and who were
moni-tored duringconsolidationand maintenance.Therefore, 20
rev
bras
hema
tol
hemoter.
2
0
1
7;
3
9(1)
:46–51
Table1–Mainfeaturesofrelapsedpatientsfromatotalof65casesofacutepromyelocyticleukemiaoftheFundac¸ãoHemope.
Case Age(years) Gender Risk Morphology Transcript
type
ATRAin
induction
phase(days)
Hematologic remission
(days)
Relapse Salvage
treatment
Status (months)
Phase Type Place Time
(months)
1 39 M I C bcr1 29 27 PT Late Molecular 35 ATRA+CT+ATO+AutoSCT Death(42)
2 24 F I C bcr2 31 56 Mn Early Hematologic 24 ATRA+ATO Death(44)
3 46 M H C bcr1 29 32 PT Late Molecular 48 ATO+AutoSCT Death(71)
4 36 M L C bcr3 30 26 PT Late Molecular 43 ATRA+CT+ATO+AutoSCT Alive(64)
5 29 F H C bcr1 32 31 Mn Early Hematologic 21 ATRA+ATO+AutoSCT Alive(28)
6 40 M H V bcr1 27 44 PT Late Hematologic 47 ATRA+ATO Alive(49)
M:male;F:female;L:low;I:intermediate;H:high;C:LMA-M3classical;V:LMA-M3variant;PT:posttreatment;Mn:maintenance;ATO:arsenictrioxide;ATRA:all-transretinoicacid;autoSCT:
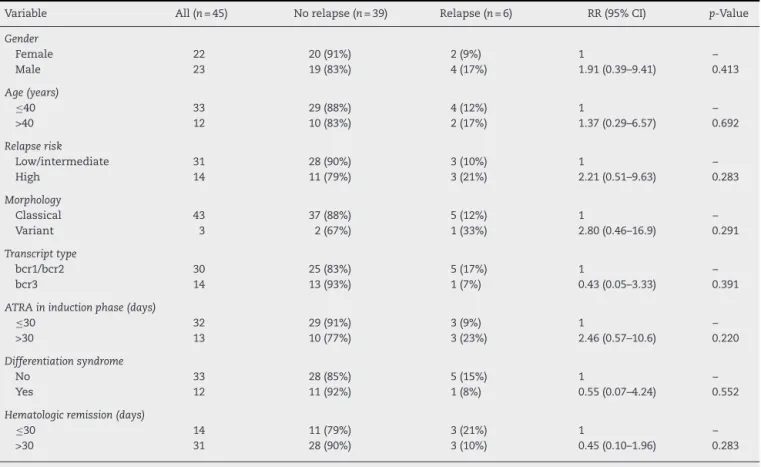
Table2–Analysisof45patientswithacutepromyelocyticleukemiatreatedatFundac¸ãoHemopeconsideringthe cumulativeincidenceofrelapse.
Variable All(n=45) Norelapse(n=39) Relapse(n=6) RR(95%CI) p-Value
Gender
Female 22 20(91%) 2(9%) 1 –
Male 23 19(83%) 4(17%) 1.91(0.39–9.41) 0.413
Age(years)
≤40 33 29(88%) 4(12%) 1 –
>40 12 10(83%) 2(17%) 1.37(0.29–6.57) 0.692
Relapserisk
Low/intermediate 31 28(90%) 3(10%) 1 –
High 14 11(79%) 3(21%) 2.21(0.51–9.63) 0.283
Morphology
Classical 43 37(88%) 5(12%) 1 –
Variant 3 2(67%) 1(33%) 2.80(0.46–16.9) 0.291
Transcripttype
bcr1/bcr2 30 25(83%) 5(17%) 1 –
bcr3 14 13(93%) 1(7%) 0.43(0.05–3.33) 0.391
ATRAininductionphase(days)
≤30 32 29(91%) 3(9%) 1 –
>30 13 10(77%) 3(23%) 2.46(0.57–10.6) 0.220
Differentiationsyndrome
No 33 28(85%) 5(15%) 1 –
Yes 12 11(92%) 1(8%) 0.55(0.07–4.24) 0.552
Hematologicremission(days)
≤30 14 11(79%) 3(21%) 1 –
>30 31 28(90%) 3(10%) 0.45(0.10–1.96) 0.283
RR:relativerisk;CI:cumulativeincidence.
inductionorconsolidation.Sixpatientsoutof45(13%) pre-sentedmolecular(three)orhematologic(three)relapse.The first relapse among the patients occurred at a median of 39months(range:21–48months)followinginitialtreatment. Medianfollow-upofthesixpatientsfromdiagnosiswas46.5 months(range:28–71months)andmeannumberof sequen-tialsamplesanalyzedduringmonitoringwas12perpatient (range:5–21months).
Themainfeaturesofthesixrelapsedcasesareshownin Table1.FourpatientsachievedMRaftersalvagetreatmentand
weresubjectedtoautologous(auto)-SCT(Cases1,3,4and5);
twoofthesearealiveandinMR.Onepatient(Case6)wasin
consolidationphaseofthetreatmentuntiltheclosingofthis
article.
Twopatients hadasecond relapse, onepatient(Case 2)
twelvemonthsafterthe first hematologic relapse whilein
salvagetreatmentwaitingforauto-SCT.Thispatienthadno
humanleukocyteantigen(HLA)-compatibledonor andwas
treatedwithATOwithout achievinga thirdremission. The
otherpatient(Case1)presentedasecondhematologicrelapse
fourteenmonthsafterthefirstmolecularrelapse.Hewas
sub-mittedtoATOtreatmentfollowedbyauto-SCT,butrelapsed3
monthslateranddied.
Table2showsthemainclinicalandlaboratorialfeaturesof
patientswithorwithoutrelapse.Nosignificantdifferencewas
observedbetweenthetwogroupsofpatientsregardinggender,
age,riskofrelapse,morphology,PMLbreakpoint,durationof
ATRAtreatmentduringinduction,frequencyofevolutionof
DSandnumberofdaystoCR.
Discussion
The13%incidenceofrelapseinthisstudywith45patients
fromasinglecenterisconsistentwithotherworks.Cassinat
etal.19 reportedarelapserateof14.6%among260patients
withAPLinamulticenterstudyinFrance.Moreover,Karim
etal.20inastudywith26patients,founda11.5%relapserateof
bothmolecularandofthecentralnervoussystem(CNS).Inthe
matched-pairanalysesofthePETHEMALPA-2005and
IC-APL-2006studies,21relapserateswere7.4%and5%,respectively.No
CNSrelapsewasdetectedinthisseries.AllPETHEMA/Gruppo
ItalianoMalattieEmatologicheMalignedell’Adulto(GIMEMA)
riskgroupswererepresentedamongrelapsedpatientswith
proportionssimilartootherstudies.22,23Theonlypatientwith
lowriskforrelapsehadabcr3PMLvariationwhichis
consid-eredofadverseprognosticfactor.24
Theresultsofthisstudyareconsistentwithpublisheddata
regardingage andgenderofthe relapsedAPLpatients.11,22
Bothmorphologicaltypes(M3andM3v)were foundamong
relapsedpatients. Inoneofthe threecasesofhematologic
relapse,therewasachangeinmorphologyfromvariant(M3v)
to classical type(M3).Morphological changes atrelapse in
APL may not be a rare event, and the leukemic cells can
showvariablemorphologicalfeaturesatthetimeofrelapse,
whichcouldresultinmisdiagnosisasadifferenttypeofacute
myeloidleukemiaaspointedoutbyYoshiietal.23Thisauthor
recommendsacomprehensiveapproachtothediagnosisand
The overall incidence of DS reported in the LPA series
variesfrom7.8%to48%.25,26 Inthecurrentseries,onecase,
thatpresentedwithDSduringtheinitialtreatment,suffered
hematologicrelapse but is alive.The EuropeanAPL Group
reportedanincreasedriskofrelapseindependentofwhite
bloodcellcountinpatientsdevelopingDS.27 Thépotetal.28
suggestedthatthetotaldurationoftreatmentwithATRAof
lessthan21daysduringtheinductionphasewasassociated
withgreaterrates ofrelapse ofleukemia.Inthisseries, all
patientswhorelapsedweretreatedwithATRAformorethan
21 days with an averageof 30 days.27–29 Nocase of
resis-tancetoATRAwasidentifiedasalltreatedpatientsachieved
remission.
Current studies have shown high rates of hematologic
relapsecomparedtomolecularrelapse.3,11,22 Inthecurrent
series,threerelapsesweremolecularandthreehematologic.
Molecular monitoring ofthe PML-RAR˛ transcriptis useful
to anticipate overt hematologic relapse10 with the IC-APL
2006protocolrecommendingtestseverythreemonthsforat
leasttwoyearsaftercompletingtreatment.3Thisapproachis
importantbecausethemajorityoftherelapsesinthisstudy
occurredduringthisperiodwithamedianof44.5months.In
thisregard,twocasesofhematologicrelapseinthisseriesdid
notstrictlyfollowthemonitoringprotocol.Althoughthemean
numberofsamplesanalyzedperpatientwashigherthanthat
reportedbyCassinatetal.,19whoanalyzedanaverageofsix
samplesperpatient(range: 1–28),thereisaneedformore
strictmonitoring.
Proposedmodalitiesoftherapyinthesalvagesettingfor
APLpatientsincludestreatmentor retreatmentwithATRA,
ATO,orboth,cytotoxicchemotherapy,autoorallogeneicSCT
andenrollmentinaclinicaltrial.2,16–18,29Patientstreatedwith
salvage chemotherapyalone havelower survivalcompared
tothosesubmittedtoSCT.17Auto-SCTshouldbeperformed
whenthepatientachievesMR,butmayincreasetheriskofa
newrelapse.Patientssubmittedtoauto-SCThavehigherrates
ofoverallanddisease-freesurvivalthanthosewhoundergo
allogeneicSCT.17AllogeneicSCTisindicatedwhenthepatient
does not achieve molecular response after consolidation.
Thesepatientsseemtohavemoreprolongedremissionsand
lessincidenceofnewrelapse,butahigherdeathratedueto
graft-versus-hostdisease(GVHD).
The protocol for relapsed patients included ATRA and
IdarubicinplusATOfollowedbyauto-SCT,afterconfirmation
ofthe MR.Four patientsdid notreceive anthracycline due
toclinicalconditions,includingonepatientwhohadaheart
attackatthetimetherelapsewasdiagnosed.
The IC-APL 2006 protocol used in the present study
significantlyreducedearlymortalityandimprovedthe
over-all survival of APL patients3 when compared to historical
controls.4 Increasedknowledgeoftheoutcome inthe
sub-populationoftreatedpatientsthatexhibitrelapseiscrucial
tounderstandingthepathophysiologyofAPLandtoimprove
survival.22 In the real-world circumstances of the
health-caredeliverysystem,costsandavailabilitybecomeissuesfor
patientsand clinicians,and showthe importanceofsingle
centerresults.Thisstudyisthefirsttoreportonmolecular
andhematologicrelapseinacohortofBrazilianAPLpatients
submittedtotheIC-APL2006protocol.
Conclusion
There were no differences in clinical-biological variables
betweenpatients withorwithout relapse. Thedataofthis
studyalsoshowtheefficacyofthetreatmentprotocolusedfor
APLandtheimportanceofprolongedmonitoringusing
molec-ular methodsto detect relapse earlier inorder to improve
survivalofthissubgroupofpatients.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
ThisstudywassupportedbytheAmericanSocietyof
Hema-tology andFundac¸ãode AmparoàCiência eTecnologiado
Estado de Pernambuco–FACEPE.The authors thank Ulisses
RamosMontarroyosforstatisticalsupport.
r
e
f
e
r
e
n
c
e
s
1.SanzMA,MartínG,GonzálezM,LeónA,RayónC,RivasC, etal.Risk-adaptedtreatmentofacutepromyelocytic leukemiawithall-trans-retinoicacidandanthracycline monochemotherapy:amulticenterstudybythePETHEMA group.Blood.2004;103(4):1237–43.
2.SeftelMD,BarnettMJ,CoubanS,LeberB,StorringJ,AssailyW, etal.ACanadianconsensusonthemanagementofnewly diagnosedandrelapsedacutepromyelocyticleukemiain adults.CurrOncol.2014;21(5):234–50.
3.RegoEM,KimHT,Ruiz-ArgüellesGJ,UndurragaMS,Uriarte MdelR,JacomoRH,etal.Improvingacutepromyelocytic leukemia(APL)outcomeindevelopingcountriesthrough networking,resultsoftheInternationalConsortiumonAPL. Blood.2013;121(11):1935–43.
4.JácomoRH,MeloRA,SoutoFR,deMattosER,deOliveiraCT, FagundesEM,etal.Clinicalfeaturesandoutcomesof134 Brazilianswithacutepromyelocyticleukemiawhoreceived ATRAandanthracyclines.Haematologica.2007;92(10):1431–2.
5.VardimanJW,ThieleJ,ArberDA,BrunningRD,BorowitzMJ, PorwitA,etal.The2008revisionoftheWorldHealth Organization(WHO)classificationofmyeloidneoplasmsand acuteleukemia:rationaleandimportantchanges.Blood. 2009;114(5):937–51.
6.vanDongenJJ,MacintyreEA,GabertJA,DelabesseE,RossiV, SaglioG,etal.StandardizedRT-PCRanalysisoffusiongene transcriptsfromchromosomeaberrationsinacuteleukemia fordetectionofminimalresidualdiseaseReportofthe BIOMED-1ConcertedAction:investigationofminimal residualdiseaseinacuteleukemia.Leukemia. 1999;13(12):1901–28.
7.GabertJ,BeillardE,vanderVeldenVH,BiW,GrimwadeD, PallisgaardN,etal.Standardizationandqualitycontrol studiesof“real-time”quantitativereversetranscriptase polymerasechainreactionoffusiongenetranscriptsfor residualdiseasedetectioninleukemia–aEuropeAgainst Cancerprogram.Leukemia.2003;17(12):2318–57.
8.ChesonBD,BennettJM,KopeckyKJ,BüchnerT,WillmanCL, EsteyEH,etal.RevisedRecommendationsofthe
responsecriteria,treatmentoutcomes,andreporting standardsfortherapeutictrialsinacutemyeloidleukemia.J ClinOncol.2003;21(24):4642–9.
9. SanzMA,LoCocoF,MartínG,AvvisatiG,RayónC,BarbuiT, etal.Definitionofrelapseriskandroleofnonanthracycline drugsforconsolidationinpatientswithacutepromyelocytic leukemia:ajointstudyofthePETHEMAandGIMEMA cooperativegroups.Blood.2000;96(4):1247–53.
10.LoCocoF,DiverioD,AvvisatiG,PettiMC,MeloniG,Pogliani EM,etal.Therapyofmolecularrelapseinacute
promyelocyticleukemia.Blood.1999;94(7):2225–9.
11.LouY,SuoS,TongY,TongH,QianW,MengH,etal.Outcomes andprognosticfactorsoffirstrelapsedacutepromyelocytic leukemiapatientsundergoingsalvagetherapywith intravenousarsenictrioxideandchemotherapy.Ann Hematol.2014;93(6):941–8.
12.MontesinosP,SanzMA.Thedifferentiationsyndromein patientswithacutepromyelocyticleukemia:experienceof thePethemagroupandreviewoftheliterature.MediterrJ HematolInfectDis.2011;3(1):e2011059.
13.RegoEM,DeSantisGC.Differentiationsyndromein promyelocyticleukemia:clinicalpresentation,pathogenesis andtreatment.MediterrJHematolInfectDis.
2011;3(1):e2011048.
14.SanzMA,MontesinosP,RayónC,HolowieckaA,delaSernaJ, MiloneG,etal.Risk-adaptedtreatmentofacute
promyelocyticleukemiabasedonall-transretinoicacidand anthracyclinewithadditionofcytarabineinconsolidation therapyforhigh-riskpatients:furtherimprovementsin treatmentoutcome.Blood.2010;115(25):5137–46.
15.PagnanoKB,RegoEM,RohrS,ChauffailleMdeL,JacomoRH, BittencourtR,etal.Guidelinesonthediagnosisand treatmentforacutepromyelocyticleukemia:Associac¸ão BrasileiradeHematologia,HemoterapiaeTerapiaCelular GuidelinesProject:Associac¸ãoMédicaBrasileira–2013.Rev BrasHematolHemoter.2014;36(1):71–92.
16.TallmanMS,AndersenJW,SchifferCA,AppelbaumFR, FeusnerJH,WoodsWG,etal.All-transretinoicacidinacute promyelocyticleukemia:long-termoutcomeandprognostic factoranalysisfromtheNorthAmericanIntergroupprotocol. Blood.2002;100(13):4298–302.
17.PemmarajuN,TanakaMF,RavandiF,LinH,
BaladandayuthapaniV,RondonG,etal.Outcomesinpatients withrelapsedorrefractoryacutepromyelocyticleukemia treatedwithorwithoutautologousorallogeneic hematopoieticstemcelltransplantation.ClinLymphoma MyelomaLeuk.2013;13(4):485–92.
18.SoignetSL.Clinicalexperienceofarsenictrioxideinrelapsed acutepromyelocyticleukemia.Oncologist.2001;6Suppl. 2:11–6.
19.CassinatB,deBottonS,KelaidiC,AdesL,ZassadowskiF, GuillemotI,etal.Whencanreal-timequantitativeRT-PCR
effectivelydefinemolecularrelapseinacutepromyelocytic leukemiapatients?(ResultsoftheFrenchBelgianSwissAPL Group).LeukRes.2009;33(9):1178–82.
20.KarimF,ShaikhU,AdilSN,KhurshidM.Clinical characteristics,outcomeandearlyinductiondeathsin patientswithacutepromyelocyticleukaemia:afive-year experienceatatertiarycarecentre.SingaporeMedJ. 2014;55(8):443–7.
21.SanzMA,MontesinosP,KimHT,Ruiz-ArgüellesGJ,Undurraga MS,UriarteMR,etal.All-transretinoicacidwith
daunorubicinoridarubicinforrisk-adaptedtreatmentof acutepromyelocyticleukaemia:amatched-pairanalysisof thePETHEMALPA-2005andIC-APLstudies.AnnHematol. 2015;94(8):1347–56.
22.LuJ,HuangX,BaoL,JiangH,ZhuH,JiangB.Treatment outcomesinrelapsedacutepromyelocyticleukemiapatients initiallytreatedwithall-transretinoicacidandarsenic compound-basedcombinedtherapies.OncolLett. 2014;7(1):177–82.
23.YoshiiM,IshidaM,YoshidaT,OkunoH,NakanishiR, HorinouchiA,etal.Clinicopathologicalfeaturesofacute promyelocyticleukemia:anexperienceinoneinstitute emphasizingthemorphologicalandimmunophenotypic changesatthetimeofrelapse.IntJClinExpPathol. 2013;6(10):2192–8,eCollection2013.
24.Castro-MujicaMdelC,Sullcahuamán-AllendeY.Subtipos molecularesdePML/RAR␣enpacientesconleucemia promielocíticaaguda.RevPeruMedExpSaludPublica. 2013;30(1):37–40.
25.SuYC,DunnP,ShihLY,KuoMC,ChangH,WuJH,etal. Retinoicacidsyndromeinpatientsfollowingthetreatmentof acutepromyelocyticleukemiawithall-transretinoicacid. ChangGungMedJ.2009;32(5):535–42.
26.ElemamO,AbdelmoetyD.Acutepromyelocyticleukemia, studyofpredictivefactorsforDifferentiationSyndrome, singlecenterexperience.JEgyptNatlCancInst. 2013;25(1):13–9.
27.deBottonS,ChevretS,CoiteuxV,DombretH,SanzM,San MiguelJ,etal.Earlyonsetofchemotherapycanreducethe incidenceofATRAsyndromeinnewlydiagnosedacute promyelocyticleukemia(APL)withlowwhitebloodcell counts:resultsfromAPL93trial.Leukemia.2003;17(2):339–42.
28.ThepotS,GardinC,ChevretS,deBottonS,RaffouxE,Guerci A,etal.ImpactofATRAdurationduringtheinduction treatmentofnewlydiagnosedAPL.ASHAnnuMeetAbstr. 2008;112(11):39.