w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Clinical
and
laboratory
profile
of
patients
with
sickle
cell
anemia
Phelipe
Gabriel
dos
Santos
Sant’Ana
a,
Ariane
Moreira
Araujo
a,
Cynthia
Teixeira
Pimenta
a,
Mário
Lúcio
Pacheco
Ker
Bezerra
a,
Sílvio
Pereira
Borges
Junior
a,
Viviana
Martins
Neto
a,
Janaina
Sousa
Dias
b,
Aline
de
Freitas
Lopes
b,
Danyelle
Romana
Alves
Rios
a,
Melina
de
Barros
Pinheiro
a,∗aUniversidadeFederaldeSãoJoãoDelRei(UFSJ),Divinópolis,MG,Brazil
bFundac¸ãoCentrodeHematologiaeHemoterapiadoEstadodeMinasGerais(HEMOMINAS),Divinópolis,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received17June2016 Accepted9September2016 Availableonline19October2016
Keywords:
Sicklecellanemia Hydroxyurea HemoglobinS
a
b
s
t
r
a
c
t
Objective:Thisstudyaimedtodescribeandanalyzeclinicalandlaboratorycharacteristics ofpatientswithsicklecellanemiatreatedattheHemominasFoundation,inDivinópolis, Brazil.Furthermore,thisstudyaimedtocomparetheclinicalandlaboratoryoutcomesof thegroupofpatientstreatedwithhydroxyureawiththosepatientsthatwerenottreated withhydroxyurea.
Methods:Clinical and laboratorial data were obtained byanalyzing medical recordsof patientswithsicklecellanemia.
Results:Datafromthemedicalrecordsof50patientswereanalyzed.Mostofthepatients werefemale(56%),agedbetween20and29yearsold.Infections,transfusions, cholecys-tectomy,splenectomyandsystemicarterialhypertensionwerethemostcommonclinical adverseeventsofthepatients.Themostfrequentcauseofhospitalizationwaspainfulcrisis. Themajorityofpatientshadreducedvaluesofhemoglobinandhematocrit(8.55±1.33g/dL and25.7±4.4%,respectively)andincreasedfetalhemoglobinlevels(12±7%).Noneofthe clinicalvariables wasstatisticallysignificant on comparingthetwogroups ofpatients. Amonghematologicalvariablesonlyhemoglobinandhematocritlevelswerestatistically differentbetweenpatientstreatedwithhydroxyureaanduntreatedpatients(p-value=0.005 andp-value=0.001,respectively).
Conclusion:Sickle cellanemia requirestreatment andfollow-up by a multiprofessional team.Acurrenttherapeuticoptionishydroxyurea.Thisdrugreducescomplicationsand improveslaboratorialparametersofpatients.Inthisstudy,theuseofthedrugincreased thehemoglobinandhematocritlevelsofpatients.
©2016Associac¸ ˜aoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthorat:UniversidadeFederaldeSãoJoãoDelRei(UFSJ),CampusCentroOeste/DonaLindu,RuaSebastiãoGonc¸alves
Coelho,400,BlocoD,sala308.1,BairroChanadour,35501-296Divinópolis,MG,Brazil. E-mailaddress:[email protected](M.B.Pinheiro).
http://dx.doi.org/10.1016/j.bjhh.2016.09.007
Introduction
Sickle cell anemia (SCA) is an inherited autosomal reces-sive disease characterizedby the presenceofhomozygous hemoglobinS(HbS).Itiscausedbyasinglenucleotide muta-tion that substitutes glutamic acid for valine in the sixth positionofthe-globingene.1Duringhypoxicconditions,the
redblood cellbecomessickledandthe resultingchange in structurerestrictscirculationcausingobstructionoftheblood flowwithinthecapillariesandearlydestructionofthecell.2
Clinical manifestations of SCA vary from mild, that is, almost asymptomatic, to severe forms that are associated with high mortality rates.3 Clinical manifestations usually
appearafterthreemonthsofage,whentheconcentrationof fetalhemoglobin(HbF)decreases.2Mostsystemsareliable
tovaso-occlusiveprocessespossiblyresultinginmultisystem failure.4–6
Adefinitivecureisnotcurrentlyavailableforpatientswith SCA.Existingtherapiesareonlyfocusedonsymptom manage-mentanddonotalterthenaturalhistoryofthedisease.These therapiesarecomprisedofhydration,preventionofinfections, painmanagement,propernutritionandprecautionsagainst adverse weatherconditions. Thus, additionaltherapies are neededtopreventcomplicationswithoutsubjectingpatients to the increased morbidity and mortality associated with highlyaggressiveapproachessuchashematopoieticstemcell transplantation(HSCT).
Currently,hydroxyurea (HU) isthe onlymedical modal-itywithprovenefficacyinpatientswithfrequentsymptoms relatedtoSCA.7,8HUisknowntoincreaseHbFlevels,improve
hemoglobinconcentrations and mean corpuscular volume, and reducethe number ofreticulocytes. Another favorable response oftreatment isthat it does not onlyreduce the expression of adhesion molecules, but also decreases the number of receptor proteins located on endothelial cells. Therefore,HUdecreasesvascularadhesionwhichcontributes bydiminishingthenumberofvaso-occlusivecrises.9,10
SCA is an inherited disease with high prevalence and mortality rate.11 However, the literature is scarce on local
epidemiologicalstudiesinBrazil.Hence,this studyaimsto analyzetheclinicalandlaboratorialcharacteristicsofpatients withSCAwholiveinthemacroregionofDivinópolis,Minas GeraistreatedintheHemominasFoundation.Furthermore, thisstudyaimstocomparetheclinicalandlaboratorial out-comesintwogroupsofpatients; those treatedwithHU to thosethatwerenottreatedwithHU.
Methods
Studysampleanddatacollectionprocedure
Aretrospectivestudywascarriedoutbasedoninformation extractedfrommedicalrecords.Thisstudywasconductedat thebloodcenteroftheHemominasFoundationinDivinópolis, Brazil.AllpatientsfromthatmacroregiondiagnosedwithSCA (limitedtothehomozygousHbSS genotype)and followed-upfromAugust2012toAugust2014wereincluded.Initially theplannedsamplewascomposedof57patientsthatis,all casesof SCAat the blood center. However, sevenpatients
were excluded from analysis (fivewere notfollowed-up in theprevioustwoyears,onepatientdiedandonepatientwas transferredtoanotherbloodcenter).
ThisstudywasapprovedbytheResearchEthicsCommittee oftheUniversidadeFederaldeSãoJoãoDelRei,Campus Cen-troOesteDonaLindu(#477.473)andbytheResearchEthics CommitteeoftheHemominasFoundation(#506.674).
Astandardizeddataextractionformwasusedtocollect informationfrompatients’medicalrecords.Alldatacollected refertotheperiodofinterest(August2012toAugust2014).The formcontainedthefollowinginformation:age,dateof diagno-sis,dateofstartingtreatment,adherencetotheinstitutional vaccinationprotocol(protectionagainstinfluenza, meningo-coccusandpneumococcus),clinicalandtherapeuticaspects, andlaboratorytestsresults.Thearithmeticmeanwas calcu-latedfromthelastfivelaboratorytestresultswithintheperiod ofthetrial.
Statisticalanalysis
Descriptivestatisticsareusedtoreportthevariablesof inter-est.Categoricalvariablesarereportedasabsoluteandrelative frequencies.Continuousvariablesarepresentedasmeansand standarddeviationormedianandinterquartilerangeifthe variableshowednon-parametricdistribution.Distributionof thedatawastestedusingtheShapiro–Wilktest.Normally dis-tributeddatawereanalyzedusingtheStudent’st-test,whilst non-parametricdatawereanalyzedusingtheMann–Whitney
Utest.Pearson’schi-squaretestorFisher’sexacttest,as appro-priate,wereusedtoassociateexposurewithoutcomes.These analyses were performed using the Statistical Package for SocialSciences(SPSSInc.,Chicago)version22forWindows. Thelevelofsignificancewassetat5%(p-value<0.05).
Results
Datafromthemedicalrecordsof50patientswereanalyzed. Females, withatotalof28(56%),were predominantinthe sample.Theagerangeofthepatientswas2–54yearswitha meanof25.4±12.9years.Whengroupedbyage,themajority ofthepatientswerebetween20and29years(36%)whilethe over50-year-oldagegroupwasthesmallest(4%).
Theageatdiagnosis wasreportedin30patientrecords, with14(46.7%)patientsdiagnosedatlessthanoneyearof age(median:1.0;interquartilerange:0.0–10.5years)aspartof theNewbornScreeningPrograminMinasGerais.Regarding thenumberofmedicalappointmentsovertheprevioustwo years,50%ofpatientshad17medicalappointmentsormore (interquartilerange:11–32consultations).
Clinicalcharacteristics
Table1–Clinicalcharacteristicsof50patientswith sicklecellanemia.
Characteristic n %
Splenectomy 7 14.0
Cholecystectomy 15 30.0
Systemicarterialhypertension 9 18.0 Chronicrenalfailure 3 6.0 Vaccinationprotocol(n=31) 24 77.4
Transfusions 20 40.0
Infections 26 52.0
1event 17 65.4
≥2events 9 34.6
Hospitalization 21 42.0
1event 16 76.2
≥2events 5 23.8
Priapism(n=22) 5 22.7
Painfulcrisis 30 60.0
Others 7 14.0
Referrals
Cardiology 32 64.0
Ophthalmology 38 76.0
Neurology 9 18.0
Othermedicalspecialties 23 46.0
Medications
Hydroxyurea 15 30.0
Vitamins 50 100.0
Analgesic/anti-inflammatory 26 52.0
Iron-chelating 11 22.0
Antibiotic 9 18.0
Other 16 32.0
Others:stroke,chronichypoxemia,acute chestsyndrome,bone necrosis,proliferativeretinopathy,hematuria.
20-year-old patients adhered to the vaccination protocol. During the study period, 20 patients (40%) received blood transfusions.Previousinfectiouseventswererecordedfor26 patients(52%),with65.4%havingjustoneinfectiousepisode. Thepredominantcausewasupperrespiratorytractinfection (46%),inparticulartonsillitis(20%ofinfections).Twenty-one patients(42%)werehospitalizedmainlyforpainfulcrisesin 43.3%ofallcases(Table1).
Regarding common acute events in SCA, priapism was reported infive (22.7%)men and painful crisisin 30 (60%)
patients(Table1).Patientswerereferredformedical special-ist appointmentsforavarietyofreasons,withthegreatest numberofreferralsbeingmadetoophthalmology(76%)and cardiology(64%)services(Table1).
Pharmacologicaltherapies
HUwasprescribedto15patients(30%)attherecommended initialsingledoseforadultsof15mg/kg/day.9,12 Indications
forHU treatment includedage olderthan three, historyof vaso-occlusive crisesthat required medicalsupport, recur-rent acute thoraciccrises, strokes, recurrent priapism and severepersistentanemiaintheprevious12months.13Even
thoughsixpatientshadaclinicalindicationforHUtreatment, theydidnotstarttreatment.Infourcases,thiswasbecause thepatientswereunabletoattendfrequentmedical appoint-mentsandthereforecouldnotperformperiodiclaboratorial testsrequiredaspertheprotocol.9,12Oftheothertwopatients,
onedidnotreceiveHUasshewastryingtoconceive,andone wasachildwhodidnothaveanadulttotakeresponsibilityfor histreatment.Allpatientstooksomevitamins,suchasfolic acid,andanalgesic/anti-inflammatorydrugswerewidelyused (52%–Table1).
Laboratorialcharacteristics
The descriptive analysis of hematological variables is shown in Table 2. The hematocrit, total hemoglobin, fetal hemoglobin, ferritin and lactate dehydrogenase values are adjusted takinginto account the reference valuesforboth genderandagegroup(Table2).
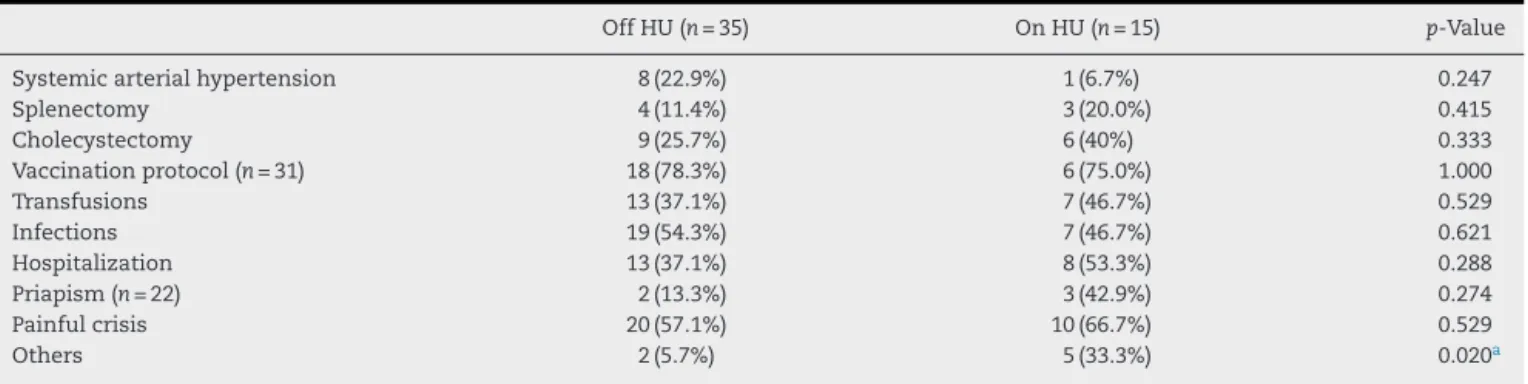
Table3comparestheincidenceofclinicaladverseevents betweenthegroupsthatreceivedHUtothosethatdidnot. Therewasnostatisticallysignificantdifferenceforthemost prevalentclinicalevents.Theincidenceofthecategory ‘oth-ers’,whichincludesthelesscommoneventssuchasstroke, acute chest syndrome, chronic hypoxemia, bone necrosis, proliferativeretinopathyandhematuria,wasstatistically dif-ferentbetweenthetwogroupsofpatientswiththeseevents beingmoreprevalentinindividualsthattookHU(Table3).
Table4showsadescriptiveand comparativeanalysisof hematologicalvariablesbetweenthetwogroups.Hematocrit and hemoglobinlevels were significantlydifferent (p-value 0.005and0.001,respectively).Therewerenosignificant
dif-Table2–Descriptionofhematologicalvariablesof50patientswithsicklecellanemia.
Mean(±standarddeviation) Median(interquartilerange25–75%) Referencea
Hematocrit(%) 25.7±4.4 – 34–49
Hemoglobin(g/dL) 8.55±1.33 – 11.5–17.5
Leukocytes(cell/mm3) – 10.354(8.271–13.846) 3500–12,000
Neutrophil(cell/mm3) – 4.945(3.664–6.914) 1500–8000
Platelets(cell/mm3) 433.418±134.348 – 15,000–400,000
Fetalhemoglobin(%) 12±7 – 0
Serumiron(g/dL) – 129.3(86.0–174.0) 35–160
Totaliron-bindingcapacity(mg/dL) – 307.5(276.5–361.0) 228–428
Ferritin(ng/mL) – 344.0(152.3–771.0) 10.0–300.0
Lactatedehydrogenase(UI/L) – 752.0(541.9–913.0) 150.0–400.0
Table3–Clinicalcharacteristicsof50patientswithsicklecellanemiatreated(onHU)andnottreated(offHU)with hydroxyurea.
OffHU(n=35) OnHU(n=15) p-Value
Systemicarterialhypertension 8(22.9%) 1(6.7%) 0.247
Splenectomy 4(11.4%) 3(20.0%) 0.415
Cholecystectomy 9(25.7%) 6(40%) 0.333
Vaccinationprotocol(n=31) 18(78.3%) 6(75.0%) 1.000
Transfusions 13(37.1%) 7(46.7%) 0.529
Infections 19(54.3%) 7(46.7%) 0.621
Hospitalization 13(37.1%) 8(53.3%) 0.288
Priapism(n=22) 2(13.3%) 3(42.9%) 0.274
Painfulcrisis 20(57.1%) 10(66.7%) 0.529
Others 2(5.7%) 5(33.3%) 0.020a
Others:stroke,chronichypoxemia,acutechestsyndrome,bonenecrosis,proliferativeretinopathy,hematuria. a Statisticallysignificantdifferencep-value<0.05.
Pearson’schi-squaretestorFisher’sexacttest.
Table4–Descriptionofhematologicalvariablesof50patientswithsicklecellanemiatreated(onHU)andnottreated(off HU)withhydroxyurea.
OffHU(n=35) OnHU(n=15) p-Value
Hematocrit(%)a 24.6±4.1 28.3±4.1 0.005c
Hemoglobin(g/dL)a 8.15±1.22 9.44±1.14 0.001c
Leukocytes(cell/mm3)b 10,502(8361–14,776) 9370(7518–13,600) 0.121
Neutrophil(cell/mm3)b 5118(4000–7005) 3760(3016–6689) 0.494
Platelets(cell/mm3)a 431,541±149,615 437,547±96,969 0.869
Fetalhemoglobin(%)a 11±5 14±9 0.212
Serumiron(g/dL)b 127.5(80.2–171.3) 151.5(106.7–175.0) 0.438 Totaliron-bindingcapacity(mg/dL)b 313.3(277.3–368.0) 296.0(273.0–352.5) 0.398
Ferritin(ng/mL)b 326.0(114.0–677.6) 528.5(250.0–1240.2) 0.201
Lactatedehydrogenase(UI/L)b 752.0(663.5–958.0) 781.5(438.5–897.7) 0.557
HU:hydroxyurea.
a Meanvalue±standarddeviation(Student’st-test).
b Median(interquartilerange25–75%)(Mann–WhitneyUtest). c Statisticallysignificantdifferencep-value<0.05.
ferencesbetweenthegroupsinrespecttotheothervariables (Table4).
Discussion
According to the results ofthis study, most patients were female,predominantlyagedbetween20and29yearsofage andhad been diagnosedataround theage ofone.Similar findingswerereportedinotherstudiesfromBrazil;the major-ityofcaseswerewomenandwereagedbetween18and30 years.14 OnestudyconductedinParanáshoweda
predomi-nanceoffemaleswithagenderratioof2:1inchildrenwith SCA.15Inanationalstudyofpatientswithsicklecelldisease,
theaverage ageatdiagnosis was8.4years.14 Inthis study,
themedianageatdiagnosiswasoneyear,whichmeetsthe currentnationalexpectationssetbytheNationalProgramof NeonatalScreeningbytheBrazilianHealthMinistryin2001.
Regarding the clinical characteristics,the rate of chole-cystectomies was high (30%) in this sample compared to the generalpopulation. This number is dueto the greater riskoftheseindividuals developing gallstones,whichis in accordance withwhat hasbeen previouslyreported inthe literature,estimated at50%.16,17 Splenectomy was another
procedure commonlyperformedinthepatients ofthe cur-rentstudy(14%).Thissurgicalprocedureisaimedatreducing deathsfromrecurrentepisodesofacutesplenicsequestration; it sometimes improves nutritional status and hematologi-callevelsrelatedtochronichypersplenism.Accordingtothe literature, the prevalence of acute splenic sequestration is estimatedataround 7.5–30%.18,19 Althoughnotall patients
investigatedinthisstudywerereferredforsurgery,therate ofsplenectomyinthisstudywaswithintheexpectedrange.
Nine of the 50 patients studied had systemic arterial hypertension(18%). Perhapsthisfinding isduetothe high prevalenceofthisdiseaseamongBrazilianadultsingeneral (20%).20 Although experimental and clinical studies report
theimpactofnitricoxidedepletiononthe pathogenesisof pulmonaryhypertensioninSCA,nostudiescorrelatearterial hypertensiontoSCA.21
beenreportedasoneofthemostfrequentcomplicationsin individualswithSCA.2
Mostpatients(77.4%)weresubmittedtothevaccination protocol.Theliteratureexplainsthisfindingbytheearly diag-nosis of SCA and screening programs, which enables the follow-upofchildrenwithSCAwithearlyantibiotic prophy-laxisandimmunizationagainstencapsulatedbacteria.2
Painfulcrisesin42%ofpatientswerethecommonest rea-sonforhospitalizationduringthetwoyearsofthisstudy.Pain, themostimpactingpresentationofthedisease,istheresultof obstructionofthemicrocirculationcausedbysickledredblood cells.Itfrequentlyhappenswithoutprodromesandaffectsthe patients’qualityoflife.22
Ophthalmology and cardiology diseases were the two most common motives for patient referrals (76% and 64% ofpatients, respectively). Previous studies haveshown the importance of ophthalmic evaluations in patients with SCA in order to prevent advanced eye disorders.23
Car-diomegaly, myocardial ischemia, biventricular dysfunction andpulmonaryhypertensionarethemostfrequentclinical complicationsrelatedtocardiovascularchangesinsicklecell disease.Theymayoccurduetochronichemolyticanemia,or secondarytopulmonarydisordersor toironoverloadfrom bloodtransfusions.24
Theliteratureshowsfavorableoutcomeswiththeuseof HU,suchasincreasesinhemoglobin,meancorpuscular vol-ume, number of leukocytes, neutrophils and platelets.25,26
Oncomparingthetwogroups,increasesinhemoglobinand hematocritvalueswerestatisticallysignificantinthisstudy.
Therewerenosignificantdifferencesbetweenthepatients receivingHUcomparedtothosewhowerenotbeingtreated withHU withregard to painfulcrises, infections, hospital-izations and number of transfusions, unlike other studies thatindicatedanimprovementintheseclinicaloutcomes.19
However,itisimportanttohighlightsomepointsthatcould contributetothisdifference,particularlyinrelationtoclinical andlaboratoryoutcomes.Bydefinition,patientswhorequired HUwereatamoreseverestageofthediseaseastheymetthe clinicalcriteriafortheuseofHU.Incontrast,thegroupthat didnotreceiveHUwascomprisedofclinicallyheterogeneous patients.Perhapsthepatientswhodidnotusethemedication presentedwithamilderformofthediseaseandtherefore,did notmeetthecriteriaforusingthemedication.Despitethis, sixpatientshadclinicalindicationstostarttreatmentwithHU butdidnotastheydidnotattendmedicalappointments fre-quentlyenoughasdemandedbytheprotocol.Thus,thegroup notreceivingthemedicationwascomprisedofpatientswith variedclinicalpresentations.Acomparisonbetweenagroup withclinicalindicationsthatistakingHUandagroup with-outclinicalindicationswhodidnottakeHUwouldprovide amoreaccurate ideaofthebenefitsofthe drug. However, methodologicalissuessuchasthetotalnumberofpatients andthecross-sectionaldesignofthestudyprecludedefinitive conclusions.
Thisstudyhassomelimitationsthatneedtobe acknowl-edged.Thepopulationinvestigatedwasveryspecificandwas notrandomlyselected.Therefore,thissamplemaynotbe rep-resentativeofthepopulation,affectingthegeneralizationof theresults.Furthermore,theheterogeneityofpatients,and therelativelysmallsamplesizepresentedachallengesince
it was not possibleto perform sub-group analyses. Future studiesshouldinvestigatealargersampletoovercomethis limitation.Additionally,the patients’medicalrecords could notbelinkedtorecordsfromotherhealthcarefacilities,such ashospitals.Insummary,morestudiesareneeded, particu-larlythosethatfocusongroupingpatientswithsimilarclinical presentationspriortocomparison.
Conclusion
Sickle cell anemia requires treatment and follow-up by a multiprofessional team. A current therapeutic option is hydroxyurea.Thisdrugreducescomplicationsandimproves laboratorialparametersofpatients.Inthisstudy,theuseof thedrugincreasedthehemoglobinandhematocritlevelsof patients.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
We acknowledge the support by Universidade Federal de São João Del Rei (UFSJ), Programa Institucional de Bolsas de Iniciac¸ão PIBIC, Fundac¸ão de Amparo à Pesquisa do estadode MinasGerais(FAPEMIG),Bolsade Iniciac¸ão Cien-tíficaPIBIC;ConselhoNacionaldeDesenvolvimentoCientífico e Tecnológico – CNPq/Brazil (Processo: 442189/2014-1); and Fundac¸ãoHemominas–HemonúcleoRegionaldeDivinópolis, inthecityofDivinópolis,MinasGerais,Brazil.
r
e
f
e
r
e
n
c
e
s
1.StypulkowskiJB,ManfrediniV.Changesinhemostasisin sicklecelldiseasepatients.RevBrasHematolHemoter. 2010;32(1):56–62.
2.DiNuzzoDV,FonsecaSF.Anemiafalciformeeinfecc¸ões.J Pediatr(RioJ).2004;80(5):347–54.
3.GalizaNetoGC,PitombeiraMdS.Aspectosmolecularesda anemiafalciforme.JBrasPatolMedLab.2003;39(1):51–6.
4.EmburyS,BennettJ,PlumF.Ceciltratadodemedicina interna.20aed.RiodeJaneiro:GuanabaraKoogan;1997.
5.CostaFF,FertrinKY.Clinicalmanifestationsandtreatmentof adultsicklecelldisease.In:Sicklecellanemia.Springer InternationalPublishing;2016.p.285–318.
6.SerjeantGR.Thenaturalhistoryofsicklecelldisease.Cold SpringHarbPerspectMed.2013;3(10):a011783.
7.ANVISA.ManualdeDiagnósticoeTratamentodeDoenc¸as Falciformes.Brasília:ANVISA;2001.
8.RodgersGP.Hydroxyureaandotherdisease-modifying therapiesinsicklecelldisease.UpToDate;2015.Available from: http://www.uptodate.com/contents/hydroxyurea-and-other-disease-modifying-therapies-in-sickle-cell-disease
[cited21.03.16].
9.Brasil.MinistériodaSaúde.ProtocoloClínicoeDiretrizes Terapêuticas–Doenc¸aFalciforme.PorteriaSAS/MSn◦55,de
29dejaneirode;2010.
StudyofHydroxyureainSickleCellAnemia.NEnglJMed. 1995;332(20):1317–22.
11.LoureiroMM,RozenfeldS.Epidemiologiadeinternac¸õespor doenc¸afalciformenoBrasil.RevSaúdePública.
2005;39(6):943–9.
12.Brasil.MinistériodaSaúde.SecretariadeAtenc¸ãoàSaúde. DepartamentodeAtenc¸ãoEspecializada.Doenc¸afalciforme: Condutasbásicasparatratamento.DepartamentodeAtenc¸ão Especializada.Brasília:MinistériodaSaúde;2012.
13.Brasil.MinistériodaSaúde.SecretariadeAtenc¸ãoàSaúde. DepartamentodeAtenc¸ãoHospitalaredeUrgência.Doenc¸a falciforme:Hidroxiureia:usoeacesso/MinistériodaSaúde, SecretariadeAtenc¸ãoàSaúde,DepartamentodeAtenc¸ão HospitalaredeUrgência.1ed.,1.reimpr.Brasília:Ministério daSaúde;2014.
14.FelixAA,SouzaHM,RibeiroSBF.Aspectosepidemiológicose sociaisdadoenc¸afalciforme.RevBrasHematolHemoter. 2010;32(3):203–8.
15.WatanabeAM,PianovskiMA,NetoJZ,LichtvanLC,
Chautard-Freire-MaiaEA,DomingosMT,etal.Prevalênciada hemoglobinaSnoEstadodoParaná,Brasil,obtidapela triagemneonatal.CadSaúdePública.2008;24(5): 993–1000.
16.GumieroAP,Bellomo-BrandãoMA,Costa-PintoEA.Gallstones inchildrenwithsicklecelldiseasefollowedupataBrazilian hematologycenter.ArqGastroenterol.2008;45(4):313–8.
17.WalkerTM,HambletonIR,SerjeantGR.Gallstonesinsickle celldisease:observationsfromTheJamaicanCohortstudy.J Pediatr.2000;136(1):80–5.
18.DuncanN,TennantI,Crawford-SykesA,BarnettA,Scarlett M,DundasS,etal.OpensplenectomyinJamaicanchildren withsicklecelldisease.WestIndianMedJ.2006;55(1):37–41.
19.TopleyJM,RogersD,StevensM,SerjeantGR.Acutesplenic sequestrationandhypersplenisminthefirstfiveyearsin homozygoussicklecelldisease.ArchDisChild.
1981;56(10):765–9.
20.PassosVM,AssisTD,BarretoSM.Hipertensãoarterialno Brasil:estimativadeprevalênciaapartirdeestudosdebase populacional.EpidemiolServSaúde.2006;15(1):35–45.
21.BunnHF,NathanDG,DoverGJ,HebbelRP,PlattOS,RosseWF, etal.Pulmonaryhypertensionandnitricoxidedepletionin sicklecelldisease.Blood.2010;116(5):687–92.
22.LoboC,MarraVN,SilvaRM.Crisesdolorosasnadoenc¸a falciforme.RevBrasHematolHemoter.2007;29(3):247–58.
23.DavidRC,MoraesJúniorHV,RodriguesMP.Alterac¸ões oculareseeletrorretinográficasnadoenc¸afalciforme.Arq BrasOftalmol.2011;74(3):190–4.
24.GualandroSF,FonsecaGH,GualandroDM.Complicac¸ões cardiopulmonaresdasdoenc¸asfalciformes.RevBrasHematol Hemoter.2007;29(3):291–8.
25.Silva-PintoAC,AnguloIL,BrunettaDM,NevesFI,BassiSC, SantisGC,etal.Clinicalandhematologicaleffectsof hydroxyureatherapyinsicklecellpatients:asingle-center experienceinBrazil.SaoPauloMedJ.2013;131(4):238–43.