RevPaulPediatr.2016;34(4):408---411
REVISTA
PAULISTA
DE
PEDIATRIA
www.rpped.com.br
ORIGINAL
ARTICLE
Efficacy
and
safety
of
chloral
hydrate
sedation
in
infants
for
pulmonary
function
tests
Gustavo
Falbo
Wandalsen
a,∗,
Fernanda
de
Cordoba
Lanza
a,b,
Márcia
Cristina
Pires
Nogueira
a,
Dirceu
Solé
aaDepartamentodePediatria,EscolaPaulistadeMedicina,UniversidadeFederaldeSãoPaulo(Unifesp),SãoPaulo,SP,Brazil bUniversidadeNovedeJulho,SãoPaulo,SP,Brazil
Received29March2016;accepted23May2016 Availableonline31August2016
KEYWORDS
Chloralhydrate; Hypnotics andsedatives; Infant
Abstract
Objective: Todescribetheefficacyandsafetyofchloralhydratesedationininfantsfor
pul-monaryfunctiontests.
Methods: Allsedationattemptsfor pulmonaryfunctiontests ininfantscarried outbetween
June2007andAugust2014wereevaluated.Obstructivesleepapneaandheartdiseasewere
contraindicationstotheexams.Anthropometricdata,examindication,useddose,outcomes
ofsedationandclinicaleventswererecordedanddescribed.
Results: Thesedationattemptsin277infants(165boys)withamedianageof51.5weeksoflife
(14---182weeks)wereevaluated.Themainindicationforthetestswasrecurrentwheezing(56%)
andthechloralhydratedoserangedfrom50to80mg/kg(orally).Eighteen(6.5%)infantshad
sometypeofclinicalcomplication,withthemostfrequentbeingcoughand/orairwaysecretion
(1.8%);respiratorydistress(1.4%)andvomiting(1.1%).Apreterm infanthadbradycardiafor
approximately15minutes,whichwasresponsivetotactilestimulation.Allobservedadverse
effectsweretransientandtherewasnoneedforresuscitationoruseofinjectablemedications.
Conclusions: Thedatademonstratedthatchloralhydrateattheemployeddosesisasafeand
effectivemedicamentforsedationduringshortproceduresininfants,suchaspulmonary
func-tiontests.Becauseofthepossibilityofsevereadverseevents,recommendationsondosesand
contraindicationsshouldbestrictlyfollowedandinfantsshouldbemonitoredbytrainedstaff.
©2016SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen
accessarticleundertheCCBYlicense(http://creativecommons.org/licenses/by/4.0/).
∗Correspondingauthor.
E-mails:[email protected],[email protected](G.F.Wandalsen).
http://dx.doi.org/10.1016/j.rppede.2016.06.001
2359-3482/©2016SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY
Efficacyandsafetyofchloralhydratesedationininfants 409
PALAVRAS-CHAVE
Hidratodecloral; Hipnóticos esedativos; Lactente
Eficáciaeseguranc¸adohidratodecloralnasedac¸ãodelactentesparatestes defunc¸ãopulmonar
Resumo
Objetivo: Descreveraeficáciaeaseguranc¸adohidratodecloralnasedac¸ãodelactentespara
testesdefunc¸ãopulmonar.
Métodos: Foramavaliadasretrospectivamentetodasastentativasdesedac¸ãoparaexamesde
func¸ãopulmonarem lactentesfeitasentrejunho 2007eagosto2014. Apneiaobstrutivado
sonoecardiopatiaforamcontraindicac¸õesparaosexames.Dadosantropométricos,indicac¸ão
doexame,doseempregada,desfechosdasedac¸ãoeintercorrênciasclínicasforamregistrados
edescritos.
Resultados: Avaliaram-seastentativasdesedac¸ãode277lactentes(165meninos)commediana
de51,5semanasdevida(14-182).Aprincipalindicac¸ãoparaostestesfoisibilânciarecorrente
(56%)eadosedehidratodecloralusadavariouentre50-80mg/kg(viaoral).Dezoito(6,5%)
lactentesapresentaramalgumtipodeintercorrênciaclínicaeforamasmaisfrequentes:tosse
e/ousecrec¸ãonaviaaérea(1,8%);desconfortorespiratórioalto(1,4%)evômitos(1,1%).Um
lactenteprematuroapresentoubradicardiaporcercade15minutos,responsivaaestimulac¸ão
tátil. Todos os efeitos adversos observados foram transitóriose não houve necessidadede
manobrasdereanimac¸ãoeusodemedicac¸õesinjetáveis.
Conclusões: Os dadosdemonstraram que o hidrato decloral, nasdoses empregadas, é um
medicamentoseguroeeficazparaasedac¸ãodelactentesemprocedimentosdecurtadurac¸ão,
como ostestes de func¸ão pulmonar.Devido à possibilidadede eventosadversos graves, as
recomendac¸õesreferentesàdosagemecontraindicac¸õesdevemserseguidasdeformarígidae
oslactentesdevemsermonitoradosporequipetreinada.
©2016SociedadedePediatriadeS˜aoPaulo. PublicadoporElsevier EditoraLtda.Este ´eum
artigoOpenAccesssobumalicenc¸aCCBY(http://creativecommons.org/licenses/by/4.0/).
Introduction
Chloralhydrate(CH)isahypnoticsedativedrugwidelyused in recent decades to sedate children. Although its exact mechanismofactionremainsuncertain,theCHis metabo-lizedtotrichloroethanol,theactivemetaboliteresponsible forthehypnoticeffects.Thehalf-lifeofthismetaboliteis 8---12hinpreschoolers,butcanbeuptofourtimeslongerin newbornsandpreterminfants.1,2
CH is the sedative of choice for pulmonary function tests in infants andhas been used inseveral laboratories for more than25 years.1,3 It is thedrug of choicedue to severalfactors. Itis administeredorally, does notrequire venipuncture and induces adequate sedation degree and durationforpulmonary functionassessmentproceduresto becarriedout.1Additionally,theavailablereference equa-tions for pulmonary function parameters were obtained after sedation with CH and use of other sedatives could hinder comparisons and induce biases.3 In a recent sur-veycarried outat 148 pulmonary functionlaboratories in infants worldwide,79% ofthem usedCHasa sedativefor exams.4
The useofCHfor sedationinyoungchildren, however, is not a consensus and severe adverse events, including deaths, have been reported.2,5 Recently, the Brazilian National Health Surveillance Agency (ANVISA) has banned the sale of CH in the country for lack of evidence of its efficacyandsafety.Theaimofthisarticleistodescribethe experienceofthepulmonaryfunctionlaboratoryininfants treatedattheDisciplineofAllergy,ClinicalImmunologyand Rheumatology of the Department of Pediatrics of Escola
Paulistade Medicina(Unifesp) regarding the use ofCH in necessarysedationforpulmonaryfunctiontests.
Method
This is a retrospective case series, which evaluated all sedationattempts for pulmonary function tests in infants betweenJune2007andAugust2014.Thepulmonary func-tiontestswerecarriedoutininfantsweighing≥4kgandno
historyof respiratoryinfectionintheprevious twoweeks. Onthedayofthepulmonaryfunctiontest,theinfantsthat cametotheservicehadfastedforatleast3handreceived anoraldoseofchloralhydrateafterclinicalevaluation.All testswereperformedwiththeinfantinthesupineposition withslightneckextensionandtestswerecarriedoutwith continuousheartrateandoxygensaturationmonitoring.A physicianandaphysicaltherapisttrainedinemergencycare werepresent in all examinationsand resuscitation equip-mentwasavailableduringalltests.
410 WandalsenGFetal.
(30cm/H2O). Chest and abdomen compression was
main-tained until the end of expiration was visually identified or for a maximum periodof four seconds. Several curves wereobtainedwithincreasingthoracoabdominal compres-sionpressure,untiltherewasnoincreaseinforcedflowand volumevalues.
To evaluate the safety and efficacy of CH in this study, anthropometric data, test indication, CH dose employed (per kg of bodyweight) and sedation outcome wererecorded,aswellassuccessfulsedationandpulmonary functionassessment.Incasesofclinicalcomplications,the natureofthesecomplicationsandrequiredprocedureswere recorded.
Alltestswereperformedafterobtainingwrittenconsent fromparents and/or guardians and after approval of the InstitutionalReview BoardofUniversidadeFederal de São Paulo(Unifesp).
Results
A total of 277 infants were assessed (165 males), witha medianageof51.5weeks(range14---182).Theindications forthetestswere:prematurityand/orlowbirthweightin74 (27%),recurrentwheezingand/orlungdiseasein156(56%), sickle-cellanemiain13(5%)andothersin34(12%)infants. CH dose ranged from 50 to 80mg/kg (orally), with a medianof70mg/kg.Thisdoseusuallyinducessleepquickly (inapproximately20min)andmaintainsitforapproximately 50min.Oftheattemptedassessments,itwasnotpossibleto performthepulmonary functiontestin32(12%)cases:18 (6.5%)duetoproblemsinsedation(9infantsdidnotsleep and9awakenedtoosoon),10(4%)duetoclinicalproblems and4 (1%) dueto technicaldifficulties. Clinicalproblems thatpreventedtheassessmentfrombeingperformedwere cough(2infants);respiratorydistress(1);vomiting(3); pres-enceofairwaysecretions(1);decreaseinperipheraloxygen saturation (SpO2) (1); bradycardia (1) and upper airway
obstruction(1).
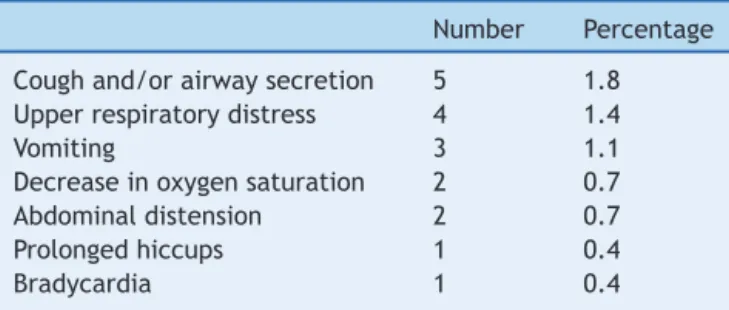
In the 245 pulmonary function tests performed, clini-calevents wereobservedduring theexamination in eight infants(3%).Thus,ofthe277sedationattempts,18(6.5%) infantsshowedsometypeofclinicalcomplicationafterCH administration.The observedadverseevents areshownin
Table1.
The actionsrequired inthese caseswereupperairway aspiration, cervical repositioning and oxygen supplemen-tation. The child that had bradycardia was a preterm infant, born at 27 weeks of gestation weighing 770g,
Table1 Adverseeventsobservedafteradministrationof
chloralhydratein277infants.
Number Percentage
Coughand/orairwaysecretion 5 1.8
Upperrespiratorydistress 4 1.4
Vomiting 3 1.1
Decreaseinoxygensaturation 2 0.7
Abdominaldistension 2 0.7
Prolongedhiccups 1 0.4
Bradycardia 1 0.4
and a chronological age of 11 months at the time of the examination.Aftersedationwith75mg/kgofCH,theheart rate decreased for about 15min, not lower than 65bpm, beingresponsivetotactilestimulation.
All adverse events observed during the 277 sedation attempts were transient, with spontaneous improvement after the end of CH action. There were no cases that required ventilation and resuscitation maneuvers, use of injectablemedicationsorhospitalization.
Discussion
CH-induced sedation is considered of moderate intensity and, therefore, it is recommended that it be performed underthesupervisionofphysiciansandhealthprofessionals trainedinlife support,withavailable resuscitation equip-mentandinfantmonitoring.
Itis knownthat theCH canreduce upper airway mus-cle tone and increase the chance of collapse in infants with some degree of upper airway obstruction, such as those with pharyngeal and palatine tonsil hypertrophy, obstructive sleep apnea and craniofacial abnormalities.1 Forthis reason,suchconditionscontraindicatepulmonary function test performance in our laboratory. Similarly, examinations are not carried out in infants with heart diseaseduetothepotentialcardiacdepressionand induc-tion of conduction disorders caused by CH, which causes arrhythmias.1
Somecommentsaboutourdataareimportant.Overall, ourfindingsreinforcedatafromotherservicesand demon-stratethesafetyandefficacyofCHasasedativetobeused forproceduresininfants.8---10
TheCHdoseusedbyus(50---80mg/kg)wassimilartothat employedbyother investigators4andsedationfailurewas observedinonly6.5%oftheattempts.Higherdosesofthe sedativeand/orrepeateddosescouldreducethenumberof failures,but areassociatedwithincreasedrisk ofadverse events.1 West etal. evaluated the efficacy and safety of CHininfantsandpreschoolersforophthalmicprocedures.9 Usingadose of80mg/kgofCH,theyobservedinadequate sedation in 7.2% of children. An additional dose of up to 40mg/kgwasadministeredincasesoffailure,withsedation failurebeingreducedto3.3%.9
In our service, we observed an incidence of 6.5% of adverseevents.Theobservedadverseeventsandtheir fre-quency weresimilarto thosedescribed by other authors, that is: paradoxical reactions (1.3%); decrease in SpO2
(1%); vomiting(0.5%) andbradycardia (0.1%).9 The report of anotherlarge case series,by Avlonitouetal. compiled adverse eventsaftersedationwithCHfor hearingtestsin 1903childrenupto14yearsofage(568childrenundersix monthsofage).8Inthisstudy,theyobservedhyperactivity in8%ofcases,vomitingin11%,mildrespiratorydiscomfort 0.5%andapneain0.2%ofthecases.8
Efficacyandsafetyofchloralhydratesedationininfants 411
The safetyof CH(80mg/kg) hasalsobeen studied in a groupof1095children(agedbetweenonemonthandthree years)sedatedforechocardiograms.11Inthisriskgroup, con-sistingmostlyofpatientswithheartdisease,10.8%hadsome adverseevent,suchasdecreaseinSpO2(5.9%),hypercapnia
(6.6%), airwayobstruction (1.4%),apnea (0.3%), hypoten-sion(0.4%)and vomiting(0.4%).Of theassessedchildren, 24%showeda decreaseinheart rate≥20%, butonly 1.4%
decreased heart rate below the normal range for age.11 Majorinterventionssuchasface-maskventilationand vol-umeexpansion werenecessary in fivecases (<0.5%),with trachealintubationinoneofthem.11
Areviewofadverseeventreportsassociatedwith seda-tioninNorth-American childrenidentified95severe cases reportedbytheendofthe1990s.5Ofthese,20wererelated totheuseofCH,with13casesleadingtodeathor perma-nentneurologicaldamage.Amongthesemoreseverecases, CHwasadministeredaloneinsevenpatientsandin combi-nationwithotherdrugsinsix.5CHoverdosewasidentified in fourcases and ninehad pre-existingclinical problems, suchastracheomalacia,tracheostomy,geneticsyndromes, congenitalheartdefectsandcerebralpalsy.5
Despite the existence of these severe adverse event reports,CHhasbeenadministeredforpulmonary function tests in a large number of studies involving thousands of infants with respiratory problems, with a low incidence of adverse events and no report of death or permanent sequelae.1
Severalothersedativedrugoptionsforinfantsare avail-able,eachshowingspecificadvantagesanddisadvantages. Midazolamisashort-durationbenzodiazepinethatiswidely usedinclinical practice,especiallyintravenously. In addi-tiontotheneedforvenousaccess,midazolamcanalsocause respiratorydepressionandhypotension.12Themain advan-tageofmidazolamis theavailabilityofanantagonistable toreverse its effects.12 More recently, the intranasal for-mulationofmidazolamhasbeendeveloped,whichismore convenient for outpatientprocedures,but withless seda-tiveaction.Dexmedetomidineisaselective␣2-adrenergic agonist capableof inducingsedation and slightanalgesia, used in several diagnostic procedures.13 It is preferably administeredintravenously, witha smallfailurerate, and its most common adverse effects are bradycardia and blood pressure changes.13,14 The effect of dexmedetomi-dineontherespiratorysystemissmalland,unlikeCH,the sedative seems to be safe in children withupper airway obstructivedisorders,butstudiesinyoungchildrenarestill limited.14
Inconclusion,thedataobtainedinourserviceare sim-ilar to those observed by other authors and demonstrate that CH, at the assessed doses, is a safe and effective drug for infant sedation during short procedures,such as pulmonary functiontests. Duetothe possibilityofsevere adverse events, dose recommendations and contraindica-tionstotheuseofCHshouldbestrictlyfollowed.Sedation withCHshouldalwaysbecarriedoutbytrainedstaff,under medicalsupervision andcontinuous monitoring ofinfants.
Specialattentionshouldbegiventoinfantsbelongingtorisk groups,suchaspreterminfants.
Funding
Thisstudydidnotreceivefunding.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.StocksJ,SlyPD,TepperRS,MorganWJ.Infantrespiratory func-tiontesting.NewYork:Wiley-LissInc;1996.
2.AllegaertK,DanielsH,NaulaersG,TibboelD,DevliegerH. Phar-macodynamicsofchloralhydrateinformerpreterminfants.Eur JPediatr.2005;164:403---7.
3.Ren C, Robinson P, Ranganathan S. Chloral hydrate seda-tionforinfantpulmonary functiontesting.PediatrPulmonol. 2014;49:1251---2.
4.Peterson-Carmichael SL, Rosenfeld M, AscherSB, Hornik CP, AretsHG,DavisSD,etal.Surveyofclinicalinfantlungfunction testingpractices.PediatrPulmonol.2014;49:126---31.
5.CotéCJ,KarlHW,NottermanDA,WeinbergJA,McCloskeyC. Adversesedationeventsinpediatrics:analysisofmedications usedforsedation.Pediatrics.2000;106:633---44.
6.Stocks J, Godfrey S, Beardmore C,Bar-Yishay E, Castile R. ERS/ATSTaskForceonStandardsforInfantRespiratoryFunction Testing.EuropeanRespiratorySociety/AmericanThoracic Soci-ety.Plethysmographicmeasurementsoflungvolumeandairway resistance.ERS/ATSTaskForceonStandardsforInfant Respira-toryFunctionTesting.EuropeanRespiratorySociety/American ThoracicSociety.EurRespirJ.2001;17:302---12.
7.AmericanThoracicSociety,EuropeanRespiratorySociety. State-ment:raisedvolumeforcedexpirationsininfants:guidelinesfor currentpractice.AmJRespirCritCareMed.2005;172:1463---71. 8.Avlonitou E,Balatsouras DG,MargaritisE, GiannakopoulosP, Douniadakis,TsakanikosM.Useofchloralhydrateasasedative forauditorybrainstemresponsetestinginapediatric popula-tion.IntJPediatrOtorhinolaryngol.2011;75:760---3.
9.West SK, Griffiths B, Shariff Y, Stephens D, Mireskandari K. Utilisationofanoutpatientsedationunitinpediatric ophthal-mology: safetyand effectiveness ofchloral hydrate in 1509 sedationepisodes.BrJOphthalmol.2013;97:1437---42. 10.LitmanRS,SoinK,SalamA.Chloralhydratesedationinterm
andpreterminfants:ananalysisofefficacyandcomplications. AnesthAnalg.2010;110:739---46.
11.HeisteinLC,RamaciottiC,ScottWA,CourseyM,SheeranPW, LemlerMS.Chloralhydratesedationforpediatric echocardiog-raphy:physiologicresponses,adverseevents,andriskfactors. Pediatrics.2006;117:e434---41.
12.Macias CG, Chumpitazi CE. Sedation and anesthesia for CT: emergingissuesforprovidinghigh-qualitycare.PediatrRadiol. 2011;41Suppl.2:S517---22.
13.CallahanP,PintoSJ,KurlandG,CainJG,MotoyamaEK,Weiner DJ. Dexmedetomidine for infantpulmonary function testing. PediatrPulmonol.2015;50:150---4.