w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Isokinetic
assessment
of
ankles
in
patients
with
rheumatoid
arthritis
Silvia
Cristina
Gutierrez
Oliveira,
Leda
Magalhaes
Oliveira,
Anamaria
Jones,
Jamil
Natour
∗RheumatologyDiscipline,UniversidadeFederaldeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received21February2014 Accepted2November2014 Availableonline29January2015
Keywords: Ankle
Isokineticassessment Peaktorque
Rheumatoidarthritis
a
b
s
t
r
a
c
t
Introduction:Thefootandankleinrheumatoidarthritisundergohighlydestructivesynovitis withlossofmusclestrength.
Objective:Toevaluatethemusclestrengthofanklesinpatientswithrheumatoidarthritis basedonisokineticdynamometryparameters.
Materialsandmethods: Thirtypatientswithadiagnosisofrheumatoidarthritisinvolvingthe ankle(s)and30healthysubjects(controlgroup)matchedforage,gender,race,bodymass indexandlowerlimbdominancewerestudied.Dorsiflexion,plantarflexion,inversionand eversionwereevaluatedinallsubjectsonanisokineticCybexNormdynamometer.The variableswerecomparedbetweentherheumatoidarthritisandcontrolgroupsandbetween theright andleftankles,andthedorsiflexor/plantar flexorandinvertor/evertormuscle strengthratiowasdetermined.
Results:Patientswithrheumatoidarthritisperformedstatisticallyworseintheisokinetic dynamometrytestforallanklemovements.Themusclestrengthratiobetweendorsiflexors andplantarflexorswasdifferentinthetwogroups.Nosignificantdifferenceswereobserved intheinvertorandevertorratios.Inthetwogroupstheplantarflexormusculaturewas statisticallystrongerthandorsiflexors.
Conclusion:Weconcludethatpatientswithrheumatoidarthritisperformworseinisokinetic dynamometryregardingallanklemovementsthancontrolsubjects,withsimilarisokinetic testresultsbeingobservedfortherightandleftsideinbothgroups,withfewexceptions. Isokineticevaluationposedno additionalrisksuchasimportantpain orinflammatory activitytopatientswithrheumatoidarthritis.
©2014ElsevierEditoraLtda.Allrightsreserved.
Avaliac¸ão
isocinética
do
tornozelo
de
pacientes
com
artrite
reumatoide
Palavras-chave: Tornozelo
r
e
s
u
m
o
Introduc¸ão:Opéeotornozelonaartritereumatoidepassamporsinovitealtamente destru-tiva,comperdadeforc¸amuscular.
∗ Correspondingauthor.
E-mail:[email protected](J.Natour). http://dx.doi.org/10.1016/j.rbre.2014.11.003
Avaliac¸ãoisocinética Picodetorque Artritereumatoide
Objetivo: Avaliaraforc¸amusculardotornozelodepacientescomartritereumatoidecom baseemparâmetrosdadinamometriaisocinética.
Materiaisemétodos: Foramestudados30pacientescomdiagnósticodeartritereumatoide. Oestudoenvolveu30indivíduossaudáveis(grupocontrole)pareadosporidade,sexo,etnia, índicedemassacorporaledominânciademembroinferior.Todososindivíduosforam sub-metidosaavaliac¸ãodaflexãodorsal,flexãoplantar,inversãoeeversãocomodinamômetro isocinéticoCybexNorm.Asvariáveisforamcomparadasentreosgruposartrite reuma-toideecontroleeentreostornozelosdireitoeesquerdo.Foideterminadaarelac¸ãodeforc¸a muscularflexoresdorsais/flexoresplantareseinversores/eversores.
Resultados: Ospacientescomartritereumatoidetiveramresultadosestatisticamentepiores notestededinamometriaisocinéticaparatodososmovimentosdotornozelo.Arelac¸ão deforc¸amuscularentreflexoresdorsaiseflexoresplantaresfoidiferentenosdoisgrupos. Nãoforamobservadasdiferenc¸assignificativasnarelac¸ãoentreinversoreseeversores.Nos doisgrupos,osmúsculosflexoresplantareseramestatisticamentemaisfortesdoqueos flexoresdorsais.
Conclusão: Ospacientescomartritereumatoidetêmpiordesempenhonadinamometria isocinéticaemtodos osmovimentosdotornozelo doqueosindivíduosdogrupo cont-role.Foramobservadosresultadossemelhantesnotesteisocinéticoparaoladodireitoe esquerdo,emambososgrupos,compoucasexcec¸ões.Aavaliac¸ãoisocinéticanão repre-sentouriscoadicional,comodorimportanteouatividadeinflamatória,empacientescom artritereumatoide.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Rheumatoidarthritis(RA)isachronicinflammatorydisease thatparticularlyinvolvesthesynovialjointsinasymmetric, generallyprogressivemanner.1,2Theanklecomplexandfeet
arecommonlyaffected.Inthelattercase,the metatarsopha-langealjointsaremostfrequentlyinvolved.Rheumatoidfeet and ankles undergo episodes ofhighly destructive synovi-tis,whichmayleadtotendonrupture,subluxation,flatfoot, halluxvalgus,etc.WiththeprogressionofRA,patientsmay experiencelimitationsanddisabilitiesintheactivitiesofdaily living,mainlydue topain,gait abnormalitiesand self-care difficulties.3
The exact quantification of muscle performance has always been a concern of health care professionals. Dur-ingrehabilitation,theobjectiveistoassessthepatientand evaluatetheeffectivenessoftherapeuticexercisesdesigned to help the patient regain muscle strength. Theisokinetic concept of exercise was developed by Perrin in 1960 and isused asan assessmentmethod ofmuscle strength pro-viding measurement to therapeutic effectivenessand it is alsoofhelpinrecoveringstrengthafterinjuriestothe mus-culoskeletal system. One of the advantages of isokinetic exercise over other types is that it allowsthe assessment ofthe maximummusclepotentialthroughoutthe rangeof motion.4
RAcausesmusclestrengthlossinpatientsstemmingfrom jointinflammation,painandedemaaswellasdisuseanda lossoffunction.5–7
Theaimofthepresentstudywastoassessanklemuscle strengthinpatientswithRAusingisokineticdynamometry. Themain isokineticdynamometer parameters were corre-lated with overall functional capacityand, specifically, the functionalcapacityoftheankleandfootjoints.
Materials
and
methods
ThirtypatientswithRAwhofulfilledcriteriaofclassification accordingtotheAmericanCollegeofRheumatology–ACR8
–andhadinvolvementoftheankle(s)wereincludedinthe study.Patientswereconsecutivelyselectedfromthe outpa-tientclinicsoftheFederalUniversityofSaoPaulo(UNIFESP). Thirtyadultswithnolowerlimbdisease,pairedforgender, age,race,lowerlimbdominanceandBMIwithpatientsfrom theRAgroup,wereselectedtothecontrolgroup.
Exclusioncriteriawereanyothertypeoflowerlimbdisease orinjury,ahistoryofjointsurgeryinthelowerlimbs,ankle infiltrations over the previous 3 months, pregnancy, heart disease,uncontrolled hypertension, coagulopathies, antico-agulant therapy,severe jointinstabilityorfibromyalgia and inabilitytoperformthecompletetest.Thestudywasapproved bytheEthicsCommitteeofUNIFESPandallsubjectssigneda termofinformedconsent.
All patients were submitted to an isokinetic test on a Cybex Normisokinetic dynamometer (CybexInternational, Inc.,Ronkonkoma,NY),whichhadbeenpreviouslycalibrated byatrainedphysiotherapist.Theisokinetictestprotocol fol-lowedtheinstructionssuggestedbyPerrin.5Beforethetest,a
warmupfor5minonanergometricbicycle(Metabolic Sys-tem Bike,Cybex– DivisionofLumex, Ronkonkoma,NY)at aspeed of60rpmwasperformed. Theprocedure wasthen explainedtothepatient,whopracticedthemovementstobe testedatthesameangularvelocitiesinordertobecome famil-iarwiththetest.Thesequenceofmovementswasrandomized foreachsubject.Bothlimbswereanalyzedandthetestwas standardizedtostartwiththerightlowerlimb.
supported in the popliteal region. The knee, the ankle to betestedandthelumbarregionwerefixedwitharesistant pad.Thecontralateralfootremainedonasupport.The sub-ject’shandswereplacedonthearmrests.Dorsiflexion/plantar flexion was tested atangular velocities of30◦/s and 60◦/s.
Eachmovementwas repeatedfive timesatthetwo veloci-ties,withrestintervalsof30sbetweeneachangularvelocity. For the inversion/eversion test, the subject waspositioned inthesamemannerasdescribedfortheprevioustestand thepositionofthedynamometerwaschanged.These move-mentsweretestedatangularvelocitiesof30◦/sand60◦/s,with
eachmovementbeingrepeatedfivetimesateachvelocity.The isokineticdynamometerparametersevaluatedforthe differ-entmovementswerepeaktorque(PT)andpeaktorqueangle (PTA).
Thefollowingparameterswereevaluated:
• Painintheanklesand/orfeet–usingvisualanalogscales (VAS)rangingfrom0to10cmtoevaluatepainatrestand duringgait.9
• Functionalcapacity–assessedusingtheHealthAssessment Questionnaire–HAQ.10,11
• Functionalcapacityoftheankle–footcomplex–theFoot FunctionalIndex (FFI) is a specific questionnaireon the foot.12,13
• Rangeofmotion–usingtheEPM-ROMscalethatisaspecific questionnaireonrangeofmotion,14andtheROMforankle
wasmeasuredusingagoniometer.
Statisticalanalysis
Average quantitativevariableswere comparedbetweenthe twogroupsbytheStudent’st-testfortwoindependent sam-ples.TheMann–Whitneytestwasonlyusedfortheisokinetic data. The correlation between quantitative variables was determinedusingPearson’scorrelationcoefficient.15A
signif-icancelevelof˛<0.05or5%wasacceptedforalltests.
Results
In the RA group the participants were 2 men and 28 women(23Caucasiansand7non-Caucasians)withan aver-age age of 50.6±1.8 years and body mass index (BMI) of 26.87±0.93kg/m2andthecontrolgroupwascomposedby2
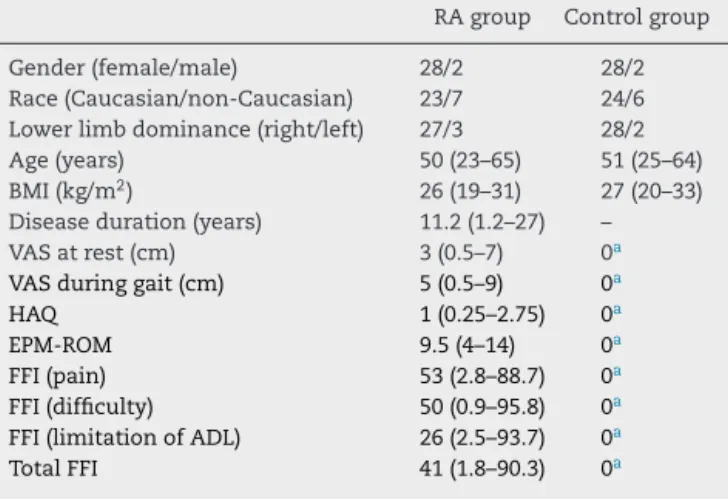
menand28 women(24Caucasians and6non-Caucasians) withanaverageageof50.5±2.1yearsandBMIof27.17±0.75. Table 1displays the sample characteristics. Thegroups were homogenous in terms of age, gender, race, weight, height,BMIandlowerlimbdominance.However,statistically significantdifferencesbetweengroupswereobservedinthe scoresofVASforankleand/orfootpain,HAQ,EPM-ROMand FFI.
RegardingtheankleROMwefoundastatisticallydifference betweengroupswiththeRAgroupshowingadecreaseinthe ROMofanklesforallmovements(Table2).
Isokinetic assessment of dorsiflexion and plantar flex-ionofthe two anklesatangular velocities of30 and 60◦/s
revealedsignificantlylowerPTvaluesintheRAgroupfor prac-ticallyallparametersanalyzed.Intheisokineticassessment
Table1–Characteristicsofthepatientsandcontrol subjects.
RAgroup Controlgroup
Gender(female/male) 28/2 28/2
Race(Caucasian/non-Caucasian) 23/7 24/6 Lowerlimbdominance(right/left) 27/3 28/2
Age(years) 50(23–65) 51(25–64)
BMI(kg/m2) 26(19–31) 27(20–33)
Diseaseduration(years) 11.2(1.2–27) –
VASatrest(cm) 3(0.5–7) 0a
VASduringgait(cm) 5(0.5–9) 0a
HAQ 1(0.25–2.75) 0a
EPM-ROM 9.5(4–14) 0a
FFI(pain) 53(2.8–88.7) 0a
FFI(difficulty) 50(0.9–95.8) 0a
FFI(limitationofADL) 26(2.5–93.7) 0a
TotalFFI 41(1.8–90.3) 0a
Data were presented as median (minimum–maximum); RA,
rheumatoidarthritis;VAS,visualanalogscaleforpain;HAQ,Health AssessmentQuestionnaire;EPM-ROM,goniometryscale;FFI,Foot FunctionalIndex;ADL,activitiesofdailyliving.
a pstatisticallysignificant.
ofinversion,significantlyhigherPTvalueswereobservedin thecontrolgroupfornearlyallvariablestested(Table3).
Comparison of the right and left sides in each group revealedsimilarPTvaluesforallmovementsstudied,except foreversionat30◦/s,whichwashigherontheleftsideinthe
RAgroup,andplantarflexionat30◦/s,whichwashigheron
therightsideinthecontrolgroup(Table3).
NosignificantdifferenceinPTAwasobservedbetweenthe RAandcontrolgroups.
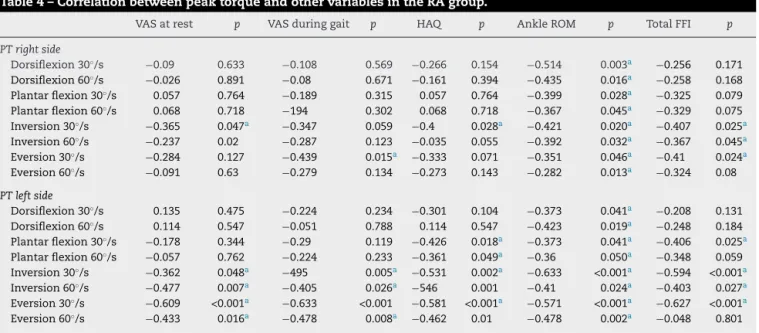
WeaktomoderatecorrelationswereobservedbetweenPT andtheHAQ,VAS(restandgait)andFFIscores.Incontrast,no satisfactorycorrelationswereobservedbetweenPTofankle movementsandage,diseaseduration,BMIorEPM-ROMscores (Table4).
Noneofthepatientsreportedexperiencingpainduringor aftertheisokinetictest.
Discussion
Previous studies have demonstrated that isokinetic dynamometry is a safe and reproducible procedure for
Table2–Rangeofmotionforanklemovements.
RAgroup Controlgroup p
DorsiflexionR 15.53(0.83) 19.6(0.3) <0.001a
DorsiflexionL 15.13(0.90) 19.6(0.3) <0.001a
PlantarflexionR 37.46(2.08) 42.1(0.3) 0.03a
PlantarflexionL 36.13(2.04) 44.2(0.7) <0.001a
InversionR 22.73(1.54) 37.9(2.0) <0.001a
InversionL 21.66(1.33) 40.5(1.0) <0.001a
EversionR 18.06(1.12) 21.4(1.0) 0.01a
EversionL 18.26(1.12) 22.0(0.9) 0.01a
Data werepresentedasmean (standarderror); RA,rheumatoid arthritis;R,right;L,left.
Table3–Peaktorqueforankles.
PTrightside PTleftside
RAgroup Controlgroup p RAgroup Controlgroup p
Dorsiflexion30◦/s 14.2(2.4) 20.9(2.1) 0.005a 12.0(1.9) 20.6(2.1) <0.001a
Dorsiflexion60◦/s 10.4(1.8) 17.7(1.8) 0.001a 8.3(1.4) 18.0(1.9) <0.001a
Plantarflexion30◦/s 20.3(2.19) 47.7(4.43) <0.001a 17.9(2.47) 43.0(3.99) <0.001a
Plantarflexion60◦/s 13.1(1.41) 36.9(3.81) <0.001a 10.8(1.80) 34.7(3.24) <0.001a
Inversion30◦/s 8.5(0.8) 17.8(1.2) <0.001a 8.4(0.7) 17.9(1.4) <0.001a
Inversion60◦/s 6.5(0.7) 13.4(1.1) <0.001a 7.1(0.6) 14.8(1.1) <0.001a
Eversion30◦/s 9.4(0.7) 16.2(0.9) <0.001a 7.1(0.7) 16.3(1.1) <0.001a
Eversion60◦/s 7.6(0.6) 13.3(0.7) <0.001a 6.2(0.6) 13.2(0.8) <0.001a
Datawerepresentedasmean(standarderror);PT,peaktorque;RA,rheumatoidarthritis.
a pstatisticallysignificant.
theassessmentofknees,shoulders andankles inpatients withRAandjuvenilerheumatoidarthritis.6,7,16,17Thesafety
ofthisprocedurewasconfirmedinthepresentstudy,asnone ofthepatientsreportedexperiencingpainduringorafterthe isokinetictest.
TheresultsfoundforROMforankleshowthatthereisa differencebetweenRApatientsandhealthcontrolsandthe moderatecorrelationfoundbetweenthisparameterandthe PTforallmovementsshowsthedirectinfluencebetweenROM andthestrengthofanklemuscles.
Nostandardizationfortheisokineticassessmentofankle strengthisavailable.Differencesinpositions,angular veloc-ities, populations and the isokinetic parameters analyzed hinder the comparison of our resultswith those obtained inother studies.Functionalstandardizationofankle isoki-netictestsisgenerallydifficult.18–21 Furthermore,inclinical
practice, the extended-knee position is contraindicated in patientspresenting involvementofother lower limbjoints withpoorstretchinthehamstrings,orincasesofinvolvement
of the sciatic nerve. Therefore, weused a supine position inthepresentstudywith80◦ hipflexionand30◦ knee
flex-ion. As this position was indicated by the manufacturer ofthe dynamometer, it providesmaximum comfortto the patient.
Inthepresentstudy,PTofallmovementswassignificantly lower in theRAgroup. For the rightlower limb(dominant side), highest PTat angularvelocities of 30 and 60◦/s was
observedforplantarflexion,followedbydorsiflexion,eversion andinversion,whereasfortheleftlowerlimb(non-dominant side)thehighestvalueswereobtainedforplantarflexion, fol-lowedbydorsiflexion,inversionandeversion.Inthecontrol group,highestPTwasobservedforplantarflexionfollowed bydorsiflexion,inversionandeversioninbothlowerlimbs. Allpatientshadstrongerplantarflexorthandorsiflexor mus-culatureinbothankles.Regardinginversionandeversionin theRAgroup,theevertorswerestrongerthantheinvertors inthedominantlegandtheinvertorswerestrongerthanthe evertorsinthenon-dominantlimb.Incontrast,inthecontrol
Table4–CorrelationbetweenpeaktorqueandothervariablesintheRAgroup.
VASatrest p VASduringgait p HAQ p AnkleROM p TotalFFI p
PTrightside
Dorsiflexion30◦/s −0.09 0.633 −0.108 0.569 −0.266 0.154 −0.514 0.003a −0.256 0.171
Dorsiflexion60◦/s −0.026 0.891 −0.08 0.671 −0.161 0.394 −0.435 0.016a −0.258 0.168
Plantarflexion30◦/s 0.057 0.764 −0.189 0.315 0.057 0.764 −0.399 0.028a −0.325 0.079
Plantarflexion60◦/s 0.068 0.718 −194 0.302 0.068 0.718 −0.367 0.045a −0.329 0.075
Inversion30◦/s −0.365 0.047a −0.347 0.059 −0.4 0.028a −0.421 0.020a −0.407 0.025a
Inversion60◦/s −0.237 0.02 −0.287 0.123 −0.035 0.055 −0.392 0.032a −0.367 0.045a
Eversion30◦/s −0.284 0.127 −0.439 0.015a −0.333 0.071 −0.351 0.046a −0.41 0.024a
Eversion60◦/s −0.091 0.63 −0.279 0.134 −0.273 0.143 −0.282 0.013a −0.324 0.08
PTleftside
Dorsiflexion30◦/s 0.135 0.475 −0.224 0.234 −0.301 0.104 −0.373 0.041a −0.208 0.131
Dorsiflexion60◦/s 0.114 0.547 −0.051 0.788 0.114 0.547 −0.423 0.019a −0.248 0.184
Plantarflexion30◦/s −0.178 0.344 −0.29 0.119 −0.426 0.018a −0.373 0.041a −0.406 0.025a
Plantarflexion60◦/s −0.057 0.762 −0.224 0.233 −0.361 0.049a −0.36 0.050a −0.348 0.059
Inversion30◦/s −0.362 0.048a −495 0.005a −0.531 0.002a −0.633 <0.001a −0.594 <0.001a
Inversion60◦/s −0.477 0.007a −0.405 0.026a −546 0.001 −0.41 0.024a −0.403 0.027a
Eversion30◦/s −0.609 <0.001a −0.633 <0.001 −0.581 <0.001a −0.571 <0.001a −0.627 <0.001a
Eversion60◦/s −0.433 0.016a −0.478 0.008a −0.462 0.01 −0.478 0.002a −0.048 0.801
RA,rheumatoidarthritis;PT,peaktorque;VAS,visualanalogscaleforpain;HAQ,HealthAssessmentQuestionnaire;ROM,rangeofmotion;FFI, FootFunctionalIndex.
group,theinvertorswerestrongerthantheevertorsinboth legs.
Studyingnormalsubjects, someauthorsreportedhigher PTvaluesforplantarflexionanddorsiflexion22,23thanthose
observedinthepresentstudyforthecontrolgroup,butthe plantarflexor/dorsiflexor ratio was similar. Dorsiflexion PT valuessimilartothoseobtainedhereforthe controlgroup were reportedbyHombäck etal. whoused thesame knee andhipangles,butwiththesubjectinthesittingposition,19
whereasSuzukietal.obtainedlowervalues.20However,inall
thesestudiescited,especiallythoseevaluatingplantar flex-ion,thesubjectwaspositionedwiththekneeextended.These variationsinkneeanglemayhaveinfluencedthedifferences indorsiflexorandplantarflexorPTobservedbetweenthese studies andthe present investigation.Howeverwehave to becautiousdoingthiscomparisonbecausethesamplefrom thesestudieswereveryheterogeneous,forexampleHomback etal.studiedyoungmenandwomen,19Suzukiet al.
stud-iedelderlywomen20whileHorstmannetal.studiedsedentary
men.23
Wennerbergevaluateddorsiflexionandplantarflexionin athletesusingthesamepositiontechniqueusedinthepresent study.Onaverage,athletespresentedhigherdorsiflexionand plantarflexionPTthanthatobservedamongthecontrol sub-jects. Analysis of the literature demonstrates that normal subjectshaveexhibitedhigherinvertorandevertorPTthan thatobservedinthecontrolgroupofourstudyaswell.24
Stud-ies involving normalsubjects and athletes haveconfirmed thatinvertorsarestrongerthanevertors.23,25–27Ourpatients
withRAhadmorestrengthintheevertorsthaninvertorsof therightlowerlimb(dominant).Thiscanbeexplainedbythe involvementofthesubtalarjointinthedominantleg,which affectstheinvertormusculature.Forbothgroups,theankle invertorsoftheleft leg(non-dominant)were strongerthan theevertors.
No studies analyzing ankle isokinetic dynamometry in patients with RA have been availableuntil now. Bröstrom etal.studieddorsiflexionandplantarflexionmusclestrength inadolescentswithpolyarticularjuvenilerheumatoid arthri-tisandhealthyage-matchedcontrols,usingpronationwith extensionofthekneesasthepositionforassessment. Con-centric PT of the two movements was significantly lower inthearthritisgroupcomparedtothecontrolgroup. More-over, the plantar flexor musculature was stronger than the dorsiflexor musculature. The authors suggested that a decrease in muscle strength may affect functions in daily activities,suchas gait,and reducelevels ofphysical activ-ity, but they did not use any instrument to verify these correlations.16
The variations in PT values reported in different stud-ies may be attributed to differences in positions, angular velocities and number of repetitions used for isokinetic dynamometry. We have to take into account too that RA patients have presence of inflammation, secondary osteoarthritis,limited ROM, involvementof multiplejoints andallofthesecaninfluencetheresultsintheisokinetictest. Standardizationoftheisokinetictestingmethodforpatients with diseases that affect the ankle–foot complex, normal subjectsand athletesisnecessaryforcomparisonsofsuch studies.
Musclestrengthasymmetryforsomemovements,which didnotnecessarilycoincidewithlowerlimbdominance,was observed in both the RA and control groups. Most of the patientswithRAandcontrolswereright-footed,withno sig-nificant difference between groups. However, a significant differencewasobservedwhencomparingevertorPT,which washigherontheleftsideintheRAgroupat30◦/s.Inthe
con-trolgroup,plantarflexorPTwashigherontherightat30◦/s.
Astudyinvolvingnormalsubjectswithrightlowerlimb dom-inance demonstratedsignificantlygreater isometricplantar strengthinthislegcomparedtothenon-dominant(left)leg.25
Inthepresentstudy,wetestedisokineticPT,whichdoesnot appeartoberelatedtolimbdominance,i.e.,musclestrengthis thesame,althoughapredominantinvolvementofoneorthe othersideisobservedinsomepatients,whichisinagreement withsomestudies.6,7,28,29
Inthepresentstudy,nosignificantdifferenceinPTAwas observedbetweentheRAandcontrolgroups.Studying dorsi-flexionandplantarflexionPTAinnormalsubjects,Horstmann et al. reported higher values than those observed in the presentcontrolgroup.However,torqueaccelerationtimewas significantlyhigher inthecontrolgroupforall movements andangularvelocitiestested.23Thus,patientswithRArequire
moretimetoreachPTA,whichisthesameasthatofnormal subjects,andoncereached,PTislower.
Muscleweaknessnexttoaninflamedjointistheresultof muscleinactivity,asatrophyhasadirecteffectonthepatient’s musclestrength.30,31PatientswithRAtreatedwith
corticoste-roidsforlongperiodsmaypresentatrophyduetoinactivity and theuseofthesedrugs,whichcauseareductioninthe volumeoftypeIImusclefibers.32,33
Inthepresentstudy,mostpatients(76.6%)concomitantly usedcorticosteroids.Asthenumberofpatientswhodidnot usethesedrugswasverylow,nostatisticalanalysiswas pos-sible.Thesefindingsagreewithsomestudiesthatconducted isometricandisokineticassessmentsofthejointsofpatients withRAorJRAandfoundthatthesepatientsinfactloseupto 75%oftheirmusclestrength.6,7,29
Weobservedonlyweaktomoderatecorrelationsbetween PTandFFIscores.Thissuggeststhatextensiveanklestrength isnotnecessarilyrequiredforgoodfunctionalcapacity. Max-imum strength is not needed for the execution of daily activities.SpecificallyregardingtheHAQ,nogoodcorrelations withtheisokineticanklevariables wereobserved.Thiswas likelyduetothefactthattheHAQisaglobalquestionnairethat involvesthejointsoftheentirebodyandactivitiesforwhich othermusclegroupsofthelowerandupperlimbsare funda-mental.Itshouldbenotedthatinvolvementoftheanklesand feetaswellaslimitationsanddisabilitiesresultingfromthe involvementofthekneesandhipsinterferewithlowerlimb activitiesinpatientswithRA.Thismayexplainthelackof sat-isfactorycorrelationsbetweentheisokineticassessmentand thequestionnairesused.
Althoughnoimportantcorrelationsbetweenankle mus-clestrength and functionaldisability were observedinthe presentstudy,someinvestigationshavereportedgait abnor-malities inpatients with sometypeof involvementofthe ankle–footcomplexasthatobservedinpatientswithRA.Such abnormalities includea reductionin the propulsion phase andgaitvelocity,anincreaseinthenumberofstepsand a reductioninsteplength,eventsthatmarkedlyincreaseenergy expenditure. Similar to the present study, Shih et al. also observedadecreaseinankle dorsiflexorand plantarflexor torqueintraumaticarthritisandconcludedthat this alter-ationwasresponsibleforthereducedpropulsionphaseofgait inpatients.4
Weobservedsignificantdifferencesintheratiooftheankle dorsiflexor to plantarflexor musculature between the two groups. Thisfinding suggests thatthe reductionofmuscle strengthobservedinpatientswithRAishigherintheplantar flexorsthandorsiflexors.Incontrast,nosignificantdifferences wereobservedintheinvertortoevertorratios, demonstrat-ingaproportionallossofmusclestrengthintheinvertorand evertormusculatureinRA.Thesefindingssuggestthatboth dorsiflexorsandplantarflexorsshouldbestrengthenedduring ankleandfootrehabilitationofpatientswithRA,withspecial emphasisontheplantarflexormusculatureandproportional strengtheningoftheinvertorandevertormuscles.
Oneofthelimitationsofourstudyisthatwedonot evalu-atethediseaseactivityandthedosageofthemedicationsused wasnotevaluated tooandboth ofthese parameterscould influenceourresults.
WeconcludethatpatientswithRAperformworsein isoki-neticdynamometrythancontrolsubjectsregardingallankle movementsandsimilarisokinetictestresultswereobserved fortherightandleftsideinbothgroups,withfewexceptions. WeakcorrelationswerefoundbetweenPTandfootfunction andpain.Theisokineticassessmentcausednoadditionalrisk suchasexcessive painorinflammatoryactivity inpatients withRA.
Conflict
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. HalbergP,ApplelboomT.Rheumatoidarthritis/history.In: HochbergMC,SilmanAJ,SmolenJS,WeinblattME,Weisman MH,editors.Rheumatology,vol.l,3rded.Spain:Mosby;2003. p.753–6.
2. O’DellJR,ImbodenJB,HellmannDB,StoneJH.Current rheumatologydiagnosis&treatment.NewYork:Lange MedicalBooks;2004.p.145–50.
3. BàlintGP,KordaJ,HangodyL,BálintP.Footandankle disorders.BestPractResClinRheumatol.2003;17:87–111. 4. PerrinDH.Isokineticexerciseandassessment.Champaign:
HumanKineticPublishers;1993.
5. ShihLY,WuJJ,LoWH.Changesingaitandmaximumankle torqueinpatientswithanklearthritis.FootAnkle. 1993;14:97–103.
6. WatanabeSH,SilvaAC,AndradeMS,NatourJ.Isokinetic evaluationoftherheumatoidshoulderAnnualEuropean
CongressRheumatology–Estocolmo.AnnRheumDis. 2002;61:161.
7.MeirelesSM,OliveiraLM,AndradeMS,SilvaAC,NatourJ. Isokineticevaluationofthekneeinpatientswithrheumatoid arthritis.JointBoneSpine.2001;69:566–73.
8.ArnettFC,EdworthSM,BlochDA,McsaneDJ,CooperNS, HealeyLA,etal.TheAmericanRheumatismAssociation1987 revisedcriteriafortheclassificationofrheumatoid.Arthritis Rheum.1998;31:315–24.
9.FerrazMB,QuaresmaMR,AquinoLR,AtraE,TugwellP, GoldsmithCH.Reliabilityofpainscalesintheassessmentof literateandilliteratepatientswithrheumatoidarthritis.J Rheumatol.1990;17:1022–4.
10.FriesJF,SpitzP,KrainesRG,HolmanHR.Measurementof patientoutcomeinarthritis.ArthritisRheum.1980;23:137–45. 11.FerrazMB,OliveiraLM,AraujoPM,AtraE,TugwellP.
Crossculturalreliabilityofthephysicalabilitydimensionof thehealthassessmentquestionnaire.Rheumatology. 1990;17:813–7.
12.Budiman-MakE,ConradKJ,RoachKE.Thefootfunctional index:ameasureoffootpainanddisability.JClinEpidemiol. 1991;44:561–70.
13.OliveiraLM,AlvesACM,MizuzakiJ,NatourJ.Adaptac¸ãoe validac¸ãoparaalínguaportuguesadoTheFootFunction Index(FFI).RevBrasReumatol.2002;42Suppl.1:PO63. 14.FerrazMB,OliveiraLM,AraújoPMP,AtraE,WalterSD. EPM-ROMscale:anevaluativeinstrumenttobeusedin rheumatoidarthritistrials.ClinExpRheumatol.1990;8:491–4. 15.ConoverWJ.Practicalnonparametricstatistics.2nded.New
York:JohnWiley&Sons,Inc.;1980.
16.BroströmE,NordlundMM,CresswellAG.Plantarand dorsiflexorstrengthinprepubertalgirlswithjuvenile idiopathicarthritis.ArchPhysMedRehabil.2004;85:1224–30. 17.HedegrenE,KnustonLM,Hanglund-ÂkerlindY,HagelbergS.
Lowerextremityisometricjointtorqueinchildrenwith juvenilechronicarthritis.ScandJRheumatol.2001;30:69–76. 18.CamelsPM,NellenM,VanderBorneI,JoudinP,MinaireP.
Concentricandeccentricisokineticassessmentof
flexor–extensortorqueratiosatthehip,knee,andankleina samplepopulationofhealthysubjects.ArchPhysMed Rehabil.1997;78:1224–30.
19.HombäckAM,PorterMM,DownhamD,LexellJ.Reliabilityof isokineticankledorsiflexionstrengthmeasurementsin healthyyoungmenandwomen.ScandJRehabilMed. 1999;31:229–39.
20.SuzukiT,BeanJF,FieldingRA.Musclepoweroftheankle flexorspredictsfunctionalperformancein
community-dwellingolderwomen.JAmGeriatrSoc. 2001;49:1161–7.
21.YaggieJA,McGregorSJ.Effectsofisokineticanklefatiguein themaintenanceofbalanceandposturallimits.ArchPhys MedRehabil.2002;83:224–8.
22.WoodsonC,BandyWD,CurisD,BaldwinD.Relationshipof isokineticpeaktorquewithworkandpowerforankleplantar flexionanddorsiflexion.JOrthopSportsPhysTher.
1995;22:113–5.
23.HorstmannT,MaschmannJ,MayerHC,HeitkampM,Handel H.Theinfluenceofageonisokinetictorqueoftheupperand lowerlegmusculatureinsedentarymen.IntJSportsMed. 1999;20:362–7.
24.WennerbergD.Reliabilityofanisokineticdorsiflexionand plantarflexionapparatus.AmJSportsMed.1991;19:519–22. 25.DamholtV,LermansenNB.Asymmetryofplantarflexion
strengthinthefoot.ActaOrthopScand.1978;49:215–9. 26.GrossMT,BrugnolottiJC.Relationshipbetweenmultiple
27.LeslieM,ZachazewskiJ,BrowneP.Reliabilityofisokinetic torquevaluesforankleinvertorsandevertors.JOrthop SportsPhysTher.1990;12:612–6.
28.GoslinMT,CharterisJ.Isokineticdynamometer:normative dataforclinicaluseinlowerextremity(knee)cases.ScandJ RehabilMed.1979;11:105–9.
29.LyngbergKK,RamsingBU,NawrockiA,HarrebyM, Danneskiold-SamsoeB.Safeandeffectiveisokineticknee extensiontraininginrheumatoidarthritis.ArthritisRheum. 1994;37:623–8.
30.BrookeMH,KaplanH.Musclepathologyinrheumatoid arthritis,polymyalgiarheumatica,andpolymyositis.Acta Path.1972;94:101–18.
31.EdströmL,NordemanR.DifferentialchangesintypeIand typeIImusclefibersinrheumatoidarthritis.ScandJ Rheumatol.1994;3:155–60.
32.MiróO,PedrolE,CasademontJ,Garcia-CarrascoM,Sanmarti R,CebriánM,etal.Muscleinvolvementinrheumatoid arthritis:clinicopathologicalstudyof21symptomaticcases. SeminArthritisRheum.1996;25:421–8.
33.StokesM,YoungA.Thecontributionofreflexinhibitionto arthrogenousmuscleweakness.ClinRehabil.1984;67: 7–14.