w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Evaluating
the
relation
of
premenstrual
syndrome
and
primary
dysmenorrhea
in
women
diagnosed
with
fibromyalgia
Rabia
Terzi
a,
Hasan
Terzi
b,∗,
Ahmet
Kale
baDepartmentofPhysicalMedicineandRehabilitation,KocaeliDerinceTrainingandResearchHospital,Kocaeli,Turkey
bDepartmentofObstetricsandGynecology,KocaeliDerinceTrainingandResearchHospital,Kocaeli,Turkey
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received13October2014
Accepted24December2014
Availableonline16March2015
Keywords:
Fibromyalgia
Premenstrualsyndrome
Primarydysmenorrhea
Depression
a
b
s
t
r
a
c
t
Objective:Inthisstudy,weaimedtoinvestigatethepresenceofpremenstrualsyndrome
(PMS),primarydysmenorrhea(PD)anddepressionamongwomenwithfibromyalgia(FM)
andhealthyfemalesandtodeterminepossiblefactorsrelatedwithPMSandPDinFM.
Method:Thepresentstudywasconductedon98femalepatientsdiagnosedwithFMand
102ageandsex-matchedhealthycontrols.Allpatientswereevaluatedforpremenstrual
syndrome(PMS)andprimarydysmenorrhea(PD).Premenstrualsyndromewasassessed
amongthepatientsforthepresenceofoneormoreaffectiveorsomaticsymptomswithin
thefivedaysprecedingmenses.Thediagnosisofprimarydysmenorrheawasdefinedas
hav-ingabdominalpainorlowerbackpainlastingatleasttwodaysduringamenstrualperiod.
Dysmenorrheawasassessedviavisualanalogscale.Dysmenorrheawasratedvia
Multidi-mensionalScoringSystem.TheHamiltondepressionscalewasappliedtoallpatients.
Results:Primarydysmenorrheawasestablishedin41%ofFMpatientsand28%ofthecontrol
group.AstatisticallysignificantdifferencewasfoundinPDbetweenthetwogroups(p=0.03).
PMSwasestablishedin42%oftheFMpatientsand25%ofthecontrolgroup.Astatistically
significantdifferencewasfoundinPMSbetweenthetwogroups(p=0.03).
Conclusion:Thereisanincreasedfrequencyofpremenstrualsyndromeanddysmenorrhea
inFMpatients.Thepatientswithhighsymptomseverityscoresandhighdepressionscores
amongtheFMpatientsareatriskofPMSandPD.
©2015ElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](H.Terzi).
http://dx.doi.org/10.1016/j.rbre.2014.12.010
Avaliac¸ão
da
relac¸ão
entre
síndrome
pré-menstrual
e
dismenorreia
primária
em
mulheres
com
fibromialgia
Palavras-chave:
Fibromialgia
Síndromepré-menstrual
Dismenorreiaprimária
Depressão
r
e
s
u
m
o
Objetivo:Oobjetivodesteestudofoiinvestigarapresenc¸adesíndromepré-menstrual(SPM),
dismenorreiaprimária(DP)edepressãoemmulherescomfibromialgia(FM)emulheres
saudáveisedeterminarpossíveisfatoresrelacionadoscomaSPMeDPnaFM.
Método: Esteestudofoirealizadocom98pacientesdosexofemininocomdiagnósticode
FMe102controlessaudáveispareadosporidadeesexo.Todasaspacientesforamavaliadas
aprocuradesíndromepré-menstrual(SPM)edismenorreiaprimária(DP).Asíndrome
pré-menstrualfoideterminadapelapresenc¸adeumoumaissintomasafetivosousomáticosnos
cincodiasanterioresàmenstruac¸ão.Odiagnósticodedismenorreiaprimáriafoidefinido
comoapresenc¸adedorabdominaloulombarcomdurac¸ãomínimadedoisdiasdurante
operíodomenstrual.Adismenorreiafoiavaliadapelaescalavisualanalógica.A
dismenor-reiafoiclassificadapeloSistemadePontuac¸ãoMultidimensional.AEscaladeDepressãode
Hamiltonfoiaplicadaatodasaspacientes.
Resultados: Adismenorreiaprimáriafoiencontradaem41%daspacientescomFMe28%
dogrupocontrole.Encontrou-sediferenc¸aestatisticamentesignificativanaDPentreosdois
grupos(p=0,03).ASPMfoidetectadaem42%daspacientescomFMe25%dogrupocontrole.
Houvediferenc¸aestatisticamentesignificativanaSPMentreosdoisgrupos(p=0,03).
Conclusão: Há um aumento nafrequência de síndrome pré-menstrual e dismenorreia
em pacientescomFM.Aquelascomescore degravidadedos sintomaselevadoe altas
pontuac¸õesdedepressãoentreaspacientescomFMestãoemriscodeSPMeDP.
©2015ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Fibromyalgia(FM) isamusculoskeletalcondition
character-ized by widespread pain, tender points, fatigue, and the
absenceofanotherdiseasetoexplainallthesesymptoms.1
Itisaconditionthataffectsapproximately5%oftheworld
populationandisparticularlyseeninwomen.2Inadditionto
widespreadpain;psychosomaticsymptoms,sleepdisorders,
cognitivedysfunctions,gynecologicalcomplaints,andsexual
dysfunctionsmaybeseeninfibromyalgia.3,4
Premenstrual syndrome (PMS) which repetitively occur
duringthelutealphaseofthemenstrualcycleischaracterized
bythepresenceofphysicalandaffective symptomswhich
interfereswithdailylifeofawoman.5 Althoughitsetiology
isunknown, genetic susceptibility, sensitivity to hormonal
changes and altered brain processes are considered to be
responsible.6,7Inaddition,gonadalhormonesarealsoknown
tobemodifycentralneurotransmitteractivitiessuchas
sero-toninandgammaaminobutyricacid(GABA);therefore,such
alterationsmaybeinvolvedintheunderlyingpathogenesisof
thedisease.8,9
Primarydysmenorrhea(PD)whichincreasedprostaglandin
levelsorprostaglandinsensitivitymayoccur,whichresultin
myometrialcontraction,ischemia,sensitivityinthepain
fib-rilsandpelvicpain,ultimately.10
PremenstrualsyndromeandPDarecommon
gynecologi-calconditionsinsexuallyactivewomen.Severalpsychological
factors and increasedcentralsensitization are accountable
forthe etiopathogenesis ofPMSand PD, asisthe casefor
fibromyalgia.11–16
Thereisalimitednumberofstudiesinvestigatinga
pos-siblerelationshipbetweenfibromyalgiaand PMSandPDin
theliterature.15,17Inthisstudy,weaimedtoinvestigatethe
presenceofPMS,PDanddepressionamongwomenwithFM
andhealthyfemalesandtodeterminepossiblefactorsrelated
withPMSandPDinFM.
Materials
and
methods
Thepresentstudywasconductedon98femalepatients
diag-nosedwithFMand102ageandsex-matchedhealthycontrols.
Thestudywasdesignedasaprospectivecase-controlstudy.
ThestudyprotocolwasapprovedbytheEthicsCommitteeof
theinstitution.Thestudyincludedfemalepatientsbetween
the ages of20 and 45 withregular menstrualperiods.The
womenwho werepregnantand menopausal,had aknown
psychiatricorgynecologicalconditionorprevioussurgery,and
thewomenwithadiseasepreventingcommunication
(men-talretardation),whowereusingoralcontraceptives,andwho
hadaseveresystemicdiseasewereexcludedfromthestudy.
Adetailedmedicalhistorywasobtainedandphysical
exam-inationswereperformedonallpatients.Demographicdata,
habits,medicationsused,gynecologicalhistory(ageof
menar-che, duration ofmenstrual cycle, duration and amount of
examinationsandinvestigationswereperformedduringthe
firstthreedaysofthemenstruation.
Diagnosisoffibromyalgia
ThediagnosisofFMwasbasedonthe2010AmericanCollege
ofRheumatology(ACR)FMdiagnosticcriteria(2010ACRFDC).
Thesymptomseverityscoresofthepatientswererecorded
basedon2010ACRcriteria.18Examinationoftenderspoints
(18intotal)wasperformedbypalpationinaccordancewith
the1990criteriaoftheACR.19Digitalpalpationwasperformed
withanapproximateforceof4kg.Thepainfulpointcountwas
recorded.ThepatientswhowerediagnosedwithFMatleast
sixmonthspriorwereincludedinthestudy.
Premenstrualsyndromeassessments
Premenstrualsyndromewasassessedbythepresenceofone
or more affective (e.g. social withdrawal, confusion,
anxi-ety, irritability, angry outbursts, or depression) or somatic
(e.g. swellingofextremities,headache,abdominalbloating,
orbreasttenderness)symptomswithinthefivedays
preced-ingmenses.Whetherthesymptomsrecurredbetweendays
4 and 13 of the cycle leading to impaired daily functions
wasalsoassessed.Thesymptomswereconfirmedbasedon
prospectivesymptomratingsintwocycles.Otherunderlying
pathologieswerealsoinvestigatedtoavoidmisdiagnosis.20,21
Diagnosisofprimarydysmenorrhea
Thepresenceofdysmenorrheawasexaminedinallpatients.
Thediagnosisofprimarydysmenorrheawasdefinedas
hav-ingabdominalpain orlower backpain lastingatleast two
days during a menstrual period. Patients with
dysmenor-rheaforsixmonthswereconsideredpositive.Dysmenorrhea
was assessedby Visual Analog Scale(VAS). Dysmenorrhea
wasratedthroughtheMultidimensionalScoringSystem.The
Multidimensional Scoring System,previously developed by
Anderschand Milsom,22 was usedto assess painintensity
amongpatients.Basedonthissystem,painlevelsaredefined
basedaccordingtothecriterialistedbelow:
1. Milddysmenorrhea:painful mensesthatdonotlimitor
hindernormaldailyactivities,andwhichresultinlittleor
nosystemicsymptomsand/oranalgesicneed.
2. Moderatedysmenorrhea:painfulmensesthatslightlylimit
orhindernormaldailyactivities,andwhichresultin
mod-eratesystemicsymptomsand/oranalgesicneed.
3. Severedysmenorrhea:painfulmensesthatseverelylimit
orhindernormaldailyactivities,resultinvisible
symp-toms(suchasfainting,vomiting,etc.),andrespondpoorly
toanalgesics.
Depression
TheHamiltondepressionscalewasappliedtoallpatients.The
Hamiltondepression ratingscale(HAMDS), whichwasfirst
developedbyHamilton,23isascalethatassessesthepatient’s
levelofdepression.Akdemiretal.24previouslyperformedthe
validityand reliabilitystudy forthe Turkishversion ofthe
HAMDS. TheHAMDSincludesatotalof17question items,
andthehighestscorethatcanbeobtainedis53.Inthisscale,
ascoreof7orlessisindicativeofthelackofanysignsrelating
todepression;ascorebetween8and16isindicativeofmildor
moderatedepression;andascoreof17oraboveisindicative
ofseveredepression.
Statisticalanalysis
Data were expressed in mean±standard deviation. The
parametric data ofthe patients were compared through a
t-test, while non-parametric data were compared through
Chi-square test. Ap valueof≤0.05 considered statistically
significant.
Results
The mean age of the patients included in the study was
35.9±5.2 years compared to 36.01±4.8 years in the
con-trol group. Nostatisticallysignificant difference wasfound
between the groups in terms of age, BMI, habitual
activi-ties, educationalstatus,maritalstatus,occupationalstatus,
and physicalexercise(p>0.05)(Table1).Forty-ninepercent
oftheFMpatientsand 51%ofthecontrolgrouphada
his-toryofsmoking.Noparticipantsusedalcoholineithergroup.
ThedurationofFMwas12±3.2months.ThemeanHAMDS
scorewas16.1±7.12inFMpatients,comparedto8.2±3.9in
thecontrolgroup,indicatingastatisticallysignificant
differ-ence (p<0.05).Thetenderpointcountwas13.15±2.2inthe
patientswithFM,comparedto3.57±1.6inthecontrolgroup.
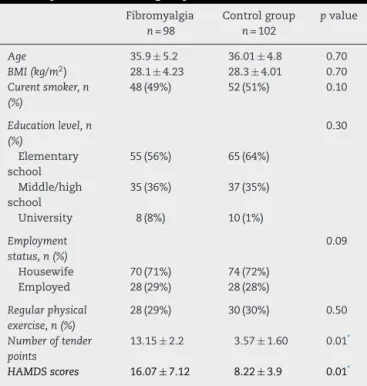
Table1–Demographicdataandnumberoftenderpoints anddepressioninbothgroups.
Fibromyalgia
n=98
Controlgroup
n=102
pvalue
Age 35.9±5.2 36.01±4.8 0.70
BMI(kg/m2) 28.1±4.23 28.3±4.01 0.70
Curentsmoker,n (%)
48(49%) 52(51%) 0.10
Educationlevel,n (%)
0.30
Elementary school
55(56%) 65(64%)
Middle/high school
35(36%) 37(35%)
University 8(8%) 10(1%)
Employment status,n(%)
0.09
Housewife 70(71%) 74(72%) Employed 28(29%) 28(28%)
Regularphysical exercise,n(%)
28(29%) 30(30%) 0.50
Numberoftender points
13.15±2.2 3.57±1.60 0.01*
HAMDSscores 16.07±7.12 8.22±3.9 0.01*
Table2–Thenumberofbothgroupsofdysmenorrhea, premenstrualsyndromeandgynecologicalhistory.
Fibromyalgia
n=98
Controlgroup
n=102
pvalue
Menstrualvolume, n(%)
0.30
Mild 40(40%) 44(43%) Moderate 36(37%) 40(40%) Severe 22(23%) 18(17%)
Durationof menstrualcycle (days)
29.01±1.23 28.76±1.45 0.50
Durationof menstruation (days)
5.47±1.42 5.28±1.72 0.08
Parity,n(%) 0.60
Nulliparous 12(12%) 12(12%) Multiparous 86(88%) 90(88%)
Methodofdelivery, n(%)
0.80
Normal delivery
66(67%) 64(63%)
Cesarean section
32(33%) 38(37%)
Ageofmenarche 12.47±1.38 12.36±1.22 0.40
Primary dysmenorrhea,n (%)
40(41%) 29(28%) 0.04*
Mild 18(45%) 15(52%)
Moderate 19(47%) 10(34%)
Severe 3(8%) 4(14%)
Dysmenorrhea VASscore
7.2±2.3 5.1±2.8 0.04*
Premenstrual syndrome,n(%)
42(42%) 25(25%) 0.03*
VAS,VisualAnalogScale. ∗ p<0.05.
Thedifferencewasstatisticallysignificant(p<0.05).However,
therewasnostatisticallysignificantdifferencebetweentwo
groupsintermsofmenstrualvolume,durationof
menstru-ation,deliverymethod,parity,andageofmenarche(p>0.05)
(Table2).
OfthepatientswithFM,41%werediagnosedwithPDwhich
wasratedasmildin18(45%)patients,moderatein19(47%)
patients,andsevereinthree(8%)patients.Amongthe
con-trols,PDwasestablishedin28%whichPDwasratedasmild
in15(52%)patients,moderateinten(34%)patients,andsevere
infour(14%)patientsinthecontrolgroup.Astatistically
sig-nificantdifferencewasfoundinPDbetweenthetwogroups
(p=0.03).ThedysmenorrheaVASvaluewas7.2±2.3intheFM
groupcomparedto5.1±2.8inthecontrolgroup,leadingtoa
significantdifference(p<0.05)(Table2).
AmongFMpatientsandhealthycontrols,PMSwas
estab-lishedin42%and25%,respectively.Astatisticallysignificant
differencewasfoundinPMSbetweenthetwogroups(p=0.03).
Thegroup withFMwas divided into two groups basedon
thepresenceofPDandPMS.Thesymptomseverityscoreof
theFMandPD(+)groupwas8.7±2.2comparedto4.5±1.8in
theFMandPS(−)group.Thetenderpointcountwas14.8±3.5
intheFMandPD(+)groupcomparedto11.8±2.4inthePD
(−) group.TheHamilton depression scorewas 19.0±4.5in
the FM and PD (+)group compared to14.0±3.5in the PD
(−)group.Astatisticallysignificantdifferencewasfoundin
symptom severityscore, tenderpointcount, and Hamilton
depressionscorebetweenthetwogroups,whereastherewas
no statistically significant difference in terms of age, BMI,
smoking,anddurationofFMdiagnosis(Table3).
ThesymptomseverityscoreoftheFMandPMS(+)group
was 9.9±5.2 comparedto 5.2±2.3in the FM and PMS (−)
groups.Thetenderpointcountwas13.6±3.6intheFMand
PMS(+)groupscomparedto12.7±4.3inthePMS(−)group.
TheHamiltondepressionscorewas19.0±7.4intheFMand
PMS(+)groupscomparedto12.9±4.3inthePMS(−)group.A
statisticallysignificantdifferencewasfoundforthesymptom
severityscoreandHamiltondepressionscorebetweenthetwo
groups,whereastherewasnostatisticallysignificant
differ-enceintenderpointcount,age,BMI,smoking,andduration
ofFMdiagnosis(Table4).
Discussion
Inthepresentstudy,PMSandPDwerestatisticallyhigherin
theFMpatientscomparedtothecontrolgroup.HAMDSscores
werealsostatisticallysignificantlyhigherintheFMpatients
comparedtothecontrolgroup.InFMpatients,HAMDSscores
and symptomseverityscoreswere statisticallysignificantly
higherinthosediagnosedwithPDandPMScomparedtothose
withoutthesediagnoses.Inthepresentstudy,PMSwas
estab-lishedin42%oftheFMpatients.Intheliterature,15–20%ofthe
menstruatingwomenwerereportedtohavePMS.25In
addi-tion,PMSisaconditionassessedwithinthescopeofcentral
sensitivitysyndromes.26Chaeetal.27foundareductioninthe
pressurepainthresholdatacupuncturepointsinthewomen
withhighsymptomseverityscoresinpremenstrualsyndrome
comparedtothosewithlowscores.Amitaletal.15investigated
thesimilaritiesbetweenpremenstrualdysphoricdisorderand
FMsyndrome,andfoundhigherlevelsoftenderpointsand
higherratesofpsychiatriccomorbiditiesinthepatientswith
PMS.Fiveof30patientswithpremenstrualdysphoricdisorder
were diagnosedwith FM.In thepresent study,the
depres-sionscoresweresignificantlyhigherintheFMpatientswith
PMScomparedtothosewithoutPMS.Furthermore,thetender
pointcountwasobservedathigherratesinthegroupwithFM
andPMScomparedtothosewithoutPMS;however,no
statis-ticallysignificantdifferencewasfound.Yunusanalyzedtwo
studiesandindicatedaprimarydysmenorrheaprevalenceof
48%inatotalof103patientswithFMSfromallstudies.12,28
In the present study, premenstrualprimary dysmenorrhea
wasestablishedin41% oftheFMpatients.Thereiscentral
hypersensitivitytonoxiousandnon-noxiousstimuliinFM.18
In primary dysmenorrhea, hyperalgesia – especially in the
deep tissues–duringthe menstrualcycle hasbeen shown
asevidenceforthepresenceofcentralsensitization.13,29
Sev-eralquantitativesensorytestswereperformedtoassessthe
presenceofthecentralsensitizationinwomenwithprimary
dysmenorrhea.Inthesestudies,the painsensitivityto
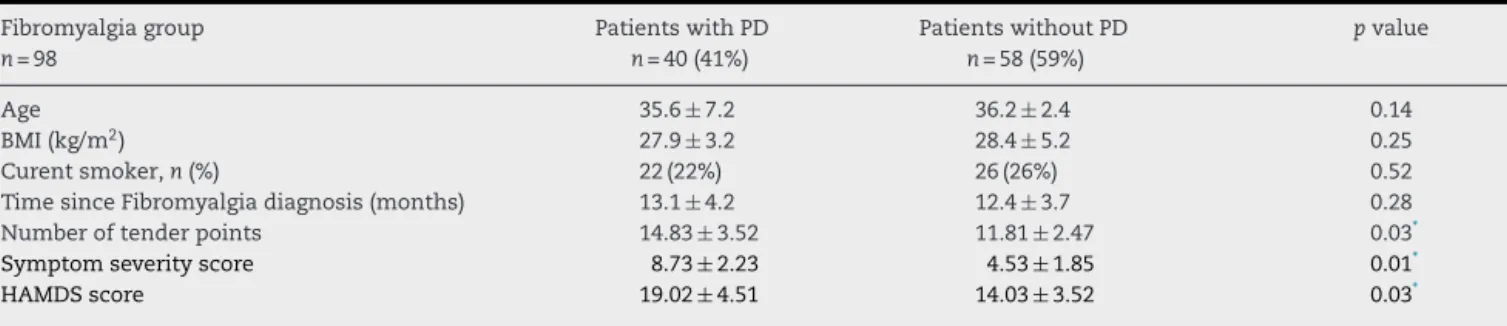
Table3–Comparisonofwithorwithoutadiagnosisofprimarydysmenorrheainpatientsdiagnosedwithfibromyalgia.
Fibromyalgiagroup
n=98
PatientswithPD
n=40(41%)
PatientswithoutPD
n=58(59%)
pvalue
Age 35.6±7.2 36.2±2.4 0.14
BMI(kg/m2) 27.9±3.2 28.4±5.2 0.25
Curentsmoker,n(%) 22(22%) 26(26%) 0.52
TimesinceFibromyalgiadiagnosis(months) 13.1±4.2 12.4±3.7 0.28 Numberoftenderpoints 14.83±3.52 11.81±2.47 0.03*
Symptomseverityscore 8.73±2.23 4.53±1.85 0.01*
HAMDSscore 19.02±4.51 14.03±3.52 0.03*
BMI,bodymassindex;HAMDS,Hamiltondepressionratingscale. ∗ p<0.05.
Table4–Comparisonofwithorwithoutadiagnosisofpremenstrualsyndromeinpatientsdiagnosedwithfibromyalgia.
Fibromyalgiagroup
n=98
PatientswithPMS
n=42(42%)
PatientswithoutPMS
n=46(58%)
pvalue
Age 35.8±5.1 36.2±3.1 0.10
BMI(kg/m2) 27.4±7.2 28.8±3.1 0.40
Curentsmoker,n(%) 22(22%) 26(27%) 0.10
Timesincefibromyalgiadiagnosis(months) 11.8±3.7 11.9±3.7 0.20
Numberoftenderpoints 13.6±3.6 12.9±4.3 0.10
Symptomseverityscore 9.97±5.2 5.27±2.3 0.01*
HAMDSscore 19.0±7.4 12.9±2.7 0.03*
BMI,bodymassindex;HAMDS,Hamiltondepressionratingscale. ∗ p<0.05.
evaluatedin womenwith and withoutdysmenorrhea. The
pain threshold against pressure,13 heat,14 and electricity15
were reduced in the abdomen, back, and extremities in
themenstrualphaseindysmenorrheicpatients, whereasit
increasedagainstcold.Inonestudy,increasedamplitudeby
CO2laserevokedcerebralpotentialinthesepatients.14Inthe
study bySoyupek et al.,17 the frequencyofFM inprimary
dysmenorrhea was 15.6%. They observed that the somatic
symptomsandsymptomseverityscoreswerehigherinthe
patients withprimary dysmenorrhea and FMcompared to
thePDpatientswithoutFM. Similarlyinthepresent study,
symptomseverityscoresanddepressionscoreswerehigher
inthePDpatientswithFMcomparedtothosewithoutPD.In
thepresentstudy,thefindingtowardthestatistically
signifi-cantlyhigherratesofPDPMSandhigherdepressionscores
inFMthan thecontrolgroupsupportsthe hypothesisthat
these conditions may have some common grounds in the
etiopathogenesis.Inthepresentstudy,thedepressionscore
wasstatisticallyhigherintheFMgroupcomparedtothe
con-trol group. Thecomorbidity ofFM was demonstrated with
manypsychiatricconditionssuchasdepression, panic
dis-order,anxiety, and posttraumaticstress disorder. Although
therelationbetweendepressionandFMhasnotbeenexactly
understood,itisbelievedthatchronicpainmaycause
depres-sion,andalsothechronicpainsyndromesmaybeavariant
ofdepression.30 Therelation betweenpain and depression
ishighlycomplexandisassociatedwithmanyfactors.The
mode of stimulus,sex, emotional status, and the
medica-tionsusedare involvedinthisinteraction.31 Inthepresent
study,depressionscoresandsymptomseverityscoreswere
higher inthegroup withpremenstrualsyndromeand
dys-menorrhea among the FM patients. As the coexistence of
otherpainfulconditionswithFMmayincreasethedepression
scores,theoccurrenceofothersymptomsmayalsobedueto
theincreasedcentralsensitizationinthepatientswithhigh
symptomseverity scores.Well-designedfurtherstudies are
requiredinthismatter.Thestudiesdemonstratedthat
sen-sorystimulicausingpainwerelowerinthedepressedpatients
comparedtothecontrolgroup.32Thehigherdepressionscores
andalsothehigherVASscores,especiallyinpatientswithFM,
suggestedthattheremightbeareductioninthepain
thresh-oldinthisgroupofpatients.
Thepresentstudyislimitedtobeacross-sectionalstudy
withalimitednumberofpopulations.Whetherthe
patholo-giesexaminedinthestudywerepresentpriortothediagnosis
ofFMwasnotinvestigated.
In conclusion, there is an increased frequency of
pre-menstrualsyndromeanddysmenorrheainFMpatients.The
patientswithhighsymptomseverityscoresandhigh
depres-sionscoresamongtheFMpatientsareatriskofPMSandPD.It,
hence,suggeststhattheremaybecommonetiopathological
mechanismsamongthesemedicalconditions.However,
fur-therlargescalestudiesarerequiredtoconfirmthesefindings.
Conflicts
of
interest
r
e
f
e
r
e
n
c
e
s
1. ArnoldLM,ClauwDJ,WohlreichMM,WangF,AhlJ,GaynorPJ, etal.Efficacyofduloxetineinpatientswithfibromyalgia: pooledanalysisof4placebo-controlledclinicaltrials.Prim CareCompanionJClinPsychiatry.2009;11:237–44.
2. WhiteKP,HarthM.Classification,epidemiologyandnatural historyoffibromyalgia.CurrPainHeadacheRep.2001;5: 320–9.
3. BigattiSM,HernandezAM,CronanTA,RandKL.Sleep disturbancesinfibromyalgiasyndrome:relationshiptopain anddepression.ArthritisRheumArthritisCareRes. 2008;59:961–7.
4. BatmazI,SariyildizMA,DilekB,InanirA,DemircanZ, HatipogluN,etal.Sexualityofmenwithfibromyalgia:what arethefactorsthatcausesexualdysfunction?RheumatolInt. 2013;33:1265–70.
5. JohnsonSR.Premenstrualsyndrome,premenstrualdysphoric disorder,andbeyond:aclinicalprimerforpractitioners. ObstetGynecol.2004;104:845–59.
6. HalbreichU.Theetiology,biology,andevolvingpathologyof premenstrualsyndromes.Psychoneuroendocrinology. 2003;28:55–99.
7. KendlerKS,KarkowskiLM,CoreyLA,NealeMC.Longitudinal population-basedtwinstudyofretrospectivelyreported premenstrualsymptomsandlifetimemajordepression.AmJ Psychiatry.1998;155:1234–40.
8. ReameNE,MarshallJC,KelchRP,PulsatileLH.Secretionin womenwithpremenstrualsyndrome(PMS):evidencefor normalneuroregulationofthemenstrualcycle.
Psychoneuroendocrinology.1992;17:205–13.
9. BäckströmT,AnderssonA,AndreéL,BirznieceV,BixoM, BjörnI,etal.Pathogenesisinmenstrualcycle-linkedCNS disorders.AnnNYAcadSci.2003;1007:42–53.
10.TsengYF,ChenCH,YangYH.Roseteaforreliefofprimary dysmenorrheainadolescents:arandomizedcontrolledtrial inTaiwan.JMidwiferyWomensHealth.2005;50:e51.
11.HalbreichU,BorensteinJ,PearlsteinT,KahnLS.The
prevalence,impairment,impact,andburdenofpremenstrual dysphoricdisorder(PMS/PMDD).Psychoneuroendocrinology. 2003;28:1–23.
12.YunusMB,MasiAT,AldagJC.Acontrolledstudyofprimary fibromyalgiasyndrome:clinicalfeaturesandassociationwith otherfunctionalsyndromes.JRheumatolSuppl.
1989;19:62–71.
13.BajajP,MadsenH,Arendt-NielsenL.Acomparisonof modality-specificsomatosensorychangesduring menstruationindysmenorrheicandnondysmenorrheic women.ClinJPain.2002;18:180–90.
14.GranotM,YarnitskyD,Itskovitz-EldorJ,GranovskyY,PeerE, ZimmmerEZ.Painperceptioninwomenwithdysmenorrhea. ObstetGynecol.2001;98:407–11.
15.AmitalD,HerskovitzC,FostickL,SilbermanA,DoronY, ZoharJ,etal.Thepremenstrualsyndromeandfibromyalgia– similaritiesandcommonfeatures.ClinRevAllergyImmunol. 2010;38:107–15.
16.YunusMB.Fibromyalgiaandoverlappingdisorders:the unifyingconceptofcentralsensitivitysyndromes.Semin ArthritisRheum.2007;36:339–56.
17.SoyupekF,GuneyM,KaplanO,KumbulDogucD.Is
fibromyalgiasyndromecommoninthepatientswithprimary dysmenorrhea?JMuskuloskeletPain.2013;21:
156–60.
18.WolfeF,ClauwDJ,FitzcharlesMA,GoldenbergDL,KatzRS, MeaseP,etal.TheAmericanCollegeofRheumatology preliminarydiagnosticcriteriaforfibromyalgiaand measurementofsymptomsseverity.ArthritisCareRes. 2010;62:600–10.
19.WolfeF,SmytheHA,YunusMB,BennettRM,BombardierC, GoldenbergDL,etal.TheAmericanCollegeofRheumatology 1990criteriafortheclassificationoffibromyalgia:reportof themulticentercriteriacommittee.ArthritisRheum. 1990;33:160–72.
20.AmericanCollegeofObstetricsandGynecology.ACOG practicebulletin:premenstrualsyndrome.Washington: ACOG;April2000.p.15.
21.FreemanEW,SammelMD,LinH,RickelsK,SondheimerSJ. Clinicalsubtypesofpremenstrualsyndromeandresponses tosertralinetreatment.ObstetGynecol.2011;118:1293–300.
22.AnderschB,MilsomI.Anepidemiologicalstudyofyoung womenwithdysmenorrhea.AmJObstetGynecol. 1982;144:655–60.
23.HamiltonM.Theassessmentofanxietystatesbyrating.BrJ MedPsychol.1959;32:505.
24.AkdemirA,TurkcaparMH,OrselSD,DemirergiN,DagI, OzbayMH.ReliabilityandvalidityoftheTurkishversionof theHamiltonDepressionRatingScale.ComprPsychiatry. 2001;42:1615.
25.LeteI,DuenasJL,SerranoI,DovalJL,Martinez-salmeanJ,Coll C,etal.AttitudesofSpanishwomentowardpremenstrual symptoms,premenstrualsyndrome,andpremenstrula dysphoricdisorder:resultsofanationwidesurvey.EurJ ObstetGynecolReprodBiol.2011;159:115–8.
26.YunusMB.Centralsensitivitysyndromes:anewparadigm andgroupnosologyforfibromyalgiaandoverlapping conditions,andtherelatedissueofdiseaseversusillness. SeminArthritisRheum.2008;37:339–52.
27.ChaeY,KimH-Y,LeeH-JP,ParkH-J,HaemD-H,AnnK,etal. Thealterationofpainsensitivityatdisease-specific acupuncturepointsinpremenstrualsyndrome.JPhysiolSci. 2000;57:115–9.
28.ChoudhuryAK,YunusMB,HaqSA,AlamMN,SebrinaF,Aldag JC.ClinicalfeaturesoffibromyalgiainaBangladeshi
population.JMuskuloskeletPain.2001;9:25–33.
29.GiamberardinoMA,BerkleyKJ,IezziS,DeBigontinaP, VecchietL.Painthresholdvariationsinsomaticwalltissues asafunctionofmenstrualcycle,segmentalsiteandtissue depthinnon-dysmenorrheicwomen,dysmenorrheicwomen andmen.Pain.1997;71:187–97.
30.BuskilaD,CohenH.Comorbidityoffibromyalgiaand psychiatricdisorders.CurrPainHeadacheRep.2007;11:333–8.
31.GieseckeT,GracelyRH,GrantMAB,NachemsonA,PetzkeF, WilliamsDA,etal.Evidenceofaugmentedcentralpain processinginidiopathicchroniclowbackpainarthritis rheum.2004;50:613–23.
32.DickensC,McGowanL,DaleS.Impactofdepressionon experimentalpainperception:asystematicreviewofthe literaturewithmeta-analysis.PsychosomMed.