www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Derivation
of
a
clinical
decision
rule
for
predictive
factors
for
the
development
of
pharyngocutaneous
fistula
postlaryngectomy
夽,夽夽
Suzana
Boltes
Cecatto
a,b,c,∗,
Matilde
Monteiro-Soares
d,
Teresa
Henriques
d,
Eurico
Monteiro
e,
Carla
Isabel
Ferreira
Pinto
Moura
faAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial(ABORL-CCF),SãoPaulo,SP,Brazil bAssociac¸ãoMédicaBrasileira(AMB),SãoPaulo,SP,Brazil
cOportoFacultyofMedicine,Oporto,Portugal
dCIDES/CINTESIS,HealthInformationandDecisionSciencesDepartment,OportoFacultyofMedicine,Oporto,Portugal eDepartmentofOtorhinolaryngology,PortugueseInstituteofOncologyofPorto,Oporto,Portugal
fDepartmentofOtorhinolaryngology,HospitalSãoJoão,PortoMedicalSchool,Oporto,Portugal
Received20March2014;accepted21September2014 Availableonline10June2015
KEYWORDS Postoperative complications; ENTsurgical procedures;
Laryngealneoplasms; Laryngectomy; Surgicalwound dehiscence;
Salivaryglandfistula
Abstract
Introduction:Pharyngocutaneousfistulaafterlarynxandhypopharynxcancersurgerycancause severaldamages.Thisstudy’saimwastoderiveaclinicaldecisionruletopredict pharyngocu-taneousfistuladevelopmentafterpharyngolaryngealcancersurgery.
Methods:Aretrospectivecohortstudywasconducted,includingallpatientsperformingtotal laryngectomy/pharyngolaryngectomy (n=171). Association between pertinent variables and pharyngocutaneousfistuladevelopmentwasassessedandapredictivemodelproposed. Results:American Society of Anesthesiologists scale, chemoradiotherapy, and tracheotomy beforesurgerywereassociatedwithfistulaintheunivariateanalysis.Inthemultivariate analy-sis,onlyAmericanSocietyofAnesthesiologistsmaintainedstatisticalsignificance.Usinglogistic regression,apredictivemodelincludingthefollowingwasderived:AmericanSocietyof Anes-thesiologists,alcohol,chemoradiotherapy,tracheotomy,hemoglobinandalbuminpre-surgery, localextension,N-classification,anddiabetesmellitus.Themodel’sscoreareaunderthecurve was0.76(95%CI0.64---0.87).Thehigh-riskgrouppresentedspecificityof93%,positivelikelihood
夽
Pleasecitethisarticleas:CecattoSB,Monteiro-SoaresM,HenriquesT,MonteiroE,MouraCIFP.Derivationofaclinicaldecisionrulefor predictivefactorsforthedevelopmentofpharyngocutaneousfistulapostlaryngectomy.BrazJOtorhinolaryngol.2015;81:394---401.
夽夽
Institution:WorkconductedatthePortugueseInstituteofOncology,cityofOporto(IPOPFG-EPE,Oporto),DepartmentofOtolaryngology, underthesphereoftheMaster’sDegreePrograminEvidenceandDecisionMakinginHealthcare---partofaMaster’sthesisdefendedbythe mainauthorinNovember2012atMedicineSchool,UniversityofOporto---Portugal.
∗
Correspondingauthor.
E-mail:[email protected](S.B.Cecatto).
http://dx.doi.org/10.1016/j.bjorl.2014.09.009
ratioof7.10,andpositivepredictivevalueof76%.Includingthemedium-low,medium-high,and high-riskgroups,asensitivityof92%,negativelikelihoodratioof0.25,andnegativepredictive valueof89%wereobserved.
Conclusion: Aclinicaldecisionrulewascreatedtoidentifypatientswithhighriskof pharyngo-cutaneousfistuladevelopment.Prognosticaccuracymeasuresweresubstantial.Nevertheless, itisessentialtoconductlargerprospectivestudiesforvalidationandrefinement.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE Complicac¸ões pós-operatórias; Procedimentos cirúrgicos otorrino-laringológicos; Neoplasiaslaríngeas; Laringectomia; Deiscênciadaferida operatória;
Fístuladasglândulas salivares
Derivac¸ãodeumaregradedecisãoclínicaparapredic¸ãodedesenvolvimentode
fístulafaringocutâneapóslaringectomia
Resumo
Introduc¸ão: Fístulafaringocutâneaapóscirurgiadecâncerdelaringeehipofaringecausa diver-sos danos. Nosso objetivo foi derivar uma regra de decisão clínica (RDC) para predizer o desenvolvimentodafístulafaringocutâneaapóscirurgia.
Método: Estudodecoorteretrospectivoincluindotodosospacientessubmetidosà laringec-tomia total e faringolaringectomia (n=171). Analisou-se a associac¸ão entre as variáveis pertinenteseodesenvolvimentodafístulaefoipropostoummodelopreditivo.
Resultados: Naanáliseunivariada,aASA,quimioradioterapia(QRT)etraqueostomiaantesda cirurgiaforamassociadasàfístula.Naanálisemultivariada,somenteaASAmanteve-se estatis-ticamentesignificante.Porregressãologística,derivamosummodelopreditivoincluindo:ASA, álcool,QRT,traqueostomia,hemoglobinaealbuminapré-operatórias,extensãolocal,N,DM. AcurvaROCdomodelofoi0,76(95%CI0,64---0,87).Ogrupodealtoriscoteveespecificidade 93%,Likelihoodpositivo7,10evalorpreditivopositivo76%.Incluindoosgruposdemédiobaixo, médioaltoealtorisco,temossensibilidadede92%,Likelihoodnegativo0,25evalorpreditivo positivo89%.
Conclusão:CriamosumaRDCparaidentificarospacientesdealtoriscoaodesenvolvimentoda fístulafaringocutânea.Asmedidasdeacuráciaprognósticaforamsubstanciais.Entretanto,é essencialconduzirestudosprospectivosmaioresparavalidac¸ão/refinamentodomodelo. ©2015Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Larynxandhypopharynxcancerrepresentsalmost45%ofall treateddiseasesinthistertiarycarehospital’sdepartment ofotolaryngology,specializedinoncology.
Prevalenceofpharyngocutaneousfistulaafterlarynxand pharyngolarynxcancersurgeryisreportedtobebetween9% and25%.1,2 Itsoccurrencevastlyincreasesthese patients’
lengthofstayandconsequentlythetreatmentcost.3
More-over, itsoccurrence can cause,amongother physical and psychological damages, the delay in onset of comple-mentary therapies (such as radiotherapy/chemotherapy), consequentlydelayingrecovery.
Untilnow,nostudyhasproposedaclinicaldecisionrule (CDR) for predicting pharyngocutaneousfistula after total laryngectomyandprimaryorrescuepharyngolaryngectomy, withorwithout neckdissection,andmajorpredictive fac-torswerescarcelyassessed.4Thus,thegoalwastoderive
sucha CDR ina sample of patientsfromthis hospital.Its creation is intended to encourage clinical behavior modi-ficationinordertoavoiddevelopmentofthiscomplication andthusfacilitatethereductionofunnecessarycostsaswell asimprovepatients’qualityoflife.
Methods
A retrospective cohort study was conducted (longitudinal historical cohort study), consecutively including all the patients performing total laryngectomy/pharyngolarynge-ctomy,duetocancerofthelarynxandhypopharynx,inthe OtolaryngologyDepartmentofthishospital,fromFebruary of2006toJuneof2011.Allpatientsdiagnosedwith laryn-gealandpharyngolaryngeal cancer wereevaluatedbythe team before final treatment. Only procedures consistent withtotallaryngectomywithorwithoutpartial pharyngec-tomy and primary closure of the pharyngeal defect were considered in this study. The operations were performed byfourdifferentsurgeons,twowithtenor moreyearsof experience,andtwowithless.
ThisstudyconductionwasapprovedbytheEthics Com-mitteeofthishospital.
Datacollection
Table1 AmericanSocietyofAnesthesiologistsrisk classi-ficationsystem.
ASAclass Classdefinition
I Normalhealthypatient
II Patientwithmildsystemicdisease III Patientwithsystemicdiseasethatisnot
incapacitating
IV Patientwithanincapacitatingsystemicdisease thatisaconstantthreattolife
V Amoribundpatientwhoisnotexpectedto survivefor24hourswithorwithoutoperation
Source:AmirQaseem,VincenzaSnow;NickFitterman;E.Rodney Hornbake;ValerieA.Lawrence;GeraldW.Smetana;KevinWeiss, DouglasK. Owens;ClinicalEfficacyAssessmentSubcommittee oftheAmericanCollegeofPhysicians;RiskAssessmentforand Strategies To Reduce Perioperative Pulmonary Complications forPatients Undergoing Noncardiothoracic.Surgery: A Guide-linefromtheAmericanCollegeofPhysicians.AnnalsofInternal Medicine.2006Apr;144(8):575---580.
January of 2012, using the institutional medical records. Follow-up was performed until the patients were dis-charged.
Asystematicreviewwasconductedinordertoidentifyall thepredictiveriskfactorsforthepharyngocutaneousfistula developmentdescribed inthe available literature(results notreportedinthisarticle).4
Allthevariables consideredaspertinentin thisreview werecollected,namely:
(a) Factors related to the patient: American Society of Anesthesiologists(ASA) classification(Table1),alcohol consumption(consideredheavyifthepatientregularly drank over 1L of alcoholic beverage per day, consid-ered ex-consumers or light consumers if they drank fromzerotofourcups/day),pre-operativehemoglobin level(<12.4g/dLor≥12.4g/dL),pre-operativealbumin
value(<37g/Lor ≥37g/L), andpresenceof major
co-morbidities(diabetesmellitus(DM),chronicobstructive pulmonarydiseases(COPD),heartdisease,orliver dis-ease).
(b) Factors related to illness: N-classification (based on theAJCC CancerStagingManual, 2010--- 7thedition), surgicalinterventionperformed(totallaryngectomyor pharyngolaryngectomy).
(c) Factors related to treatment: radiotherapy only (Rt) or chemoradiotherapy (CRT) prior to surgery and tra-cheotomypriortooperation.
Nutritionaldeficiencyandlossofweightwerepreviously excludedfromtheanalysisbecauseinsufficientdatawere availableinthemedicalrecordsassessed(120missing).
Regardingoutcome,pharyngocutaneousfistula develop-mentwasconfirmedclinically inpostoperativedaily visits bymorethanoneobserver(surgeonandresident)withthe utterancecontentofsalivaandthepaththefistulouswound analysis.
Statisticalanalysis
All variables were categorical andtheir presence in each group (with or without outcome development) was com-pared using the chi-squared or Fisher’s exact test, when applicable.Significancewasconsideredasap-value<0.05. The inclusion of ten to fifteen subjects per assessed predictivevariableisrecommended.5Asthepresent study
analyzedtheassociationbetween13variablesandan out-come,atleast130subjectswererequired.
It is common to observe that, when conducting mul-tivariate analysis, thereis a change in several predictive variables’ significance level. Thus, in several studies,5---7
variables have been included in the multivariate analysis whenap-value<0.2isobservedintheunivariateanalysis. In thismanner, it is assured thatall pertinentand poten-tiallypredictive variables arestudied.The same criterion wasusedfordetecting whichvariablesshouldbeincluded inthisstudy’sderivedmodel.
Multivariateanalysis,usinglogisticregression,was con-ductedforthepredictivemodel’sderivation.
Afterthepredictivemodelwascreated,theareaunder thereceiveroperatingcharacteristiccurve(AUC)was cal-culated and,throughthe ‘‘bestfit’’ ofthecoordinates of thecurve,fourriskcategorieswerecreated:highrisk(4), medium-high risk (3), medium-low risk (2), and low risk (1).Thesensitivity,specificity,predictivevalues,and like-lihood ratios with 95% confidence intervals (95% CI) were calculated.AllstatisticalanalysiswasperformedusingSPSS version18.0.
Results
Thisstudyincluded171subjects,characterizedinTable2. AlltheparticipantswereM0andpharyngealclosurewas performedwithtwolayers(musclesandmucosa)of contin-uoussutureorstapler(usedwheneverpossible).
Duringameanfollow-upof30days,48subjects(28.1%) developedpharyngocutaneousfistulapostoperatively.They wereallclassifiedasASA2or3;79.2%ashighalcohol con-sumers, almost 48.9% had preoperative hemoglobin level below 12.5g/dL, 16.7% were diabetic patients, 6.2% had somedegreeofCOPD,22.9%showedimpairedliverfunction orsomedegree ofheartdisease,8.3%hadreceived radio-therapy previouslytotheoperation,18.8%hadundergone chemotherapy/radiotherapy priortothe operation,andin 58.3% an emergencytracheotomy beforeelective surgery wasrequired.Infact,45%wereperformedemergentlyand 13.3%wereelectivetracheotomies.
Itwasobservedthatpatients withadvancedstage(IVa and IVb) hadthe largest absolute number of pharyngocu-taneousfistula(n=40)observedinthesample,althoughit wasnotstatisticallysignificant(p=0.25).However,the87 remainingpatientsinthesestages(representingalmost50% ofthesample)didnotdevelopafistula.Univariateand mul-tivariateanalysiswasperformed withtheinclusionof the relevantfactorsobtainedbyaprevioussystematicreview,4
which had potential for inclusion in the predictive model beingdeveloped,asalreadyexplained(Table3).
Table2 CharacterizationofthesampleaccordingtoTNM stage(AJCCCancerStagingManual,2010---7thedition)and demographicfeatures.
Characteristic Frequency
(n=171) %
Demographicfeatures
Malegender 166 97.1
Age(>60years) 75 43.9
Smokinghabits(>20cigarettes/day) 142 83 Stage
I 1 0.6
II 5 2.9
III 38 22.2
IVa 120 70.2
IVb 7 4.1
T
Tis 1 0.6
T1 1 0.6
T2 5 2.9
T3 45 26.3
T4a 119 69.6
N
N0 83 48.5
N1 25 14.6
N2a 28 16.4
N2b 17 9.9
N2c 13 7.6
N3 5 2.9
associatedwithfistuladevelopmentintheunivariate anal-ysis.Inthemultivariateanalysis,onlytheASAclassification maintainedstatisticalsignificance(p<0.05).Albumin,prior CRT, and tracheotomy performed before surgery showed predictivepotential(p<0.2)forinclusioninthemodel.
Althoughalbumindidnotachievestatisticalsignificance in the univariate analysis and there were many missing
1.0
0.8
0.6
0.4
0.2
0.0
0.0 0.2 0.4 0.6 0.8 1.0 1-specificity
Sensitivity
Model1 Modelcat2 Reference line Source of the curve ROC curve
Diagonal segments are produced by ties
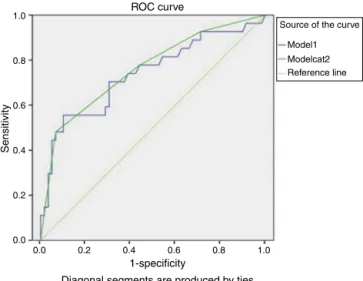
Figure1 Model’sareaunderthereceiveroperating charac-teristiccurve.Ivoryline,lineofreferenceofAUC0.5;blueline, scoreofthemodel;greenline,fourcategoriesofthemodel.
albuminvaluesinthissample(85missing),itwasobserved thatitsexclusionfromthemodelsubstantiallyreducedthe validity(particularlyregardingsensitivity).
Alcohol consumption, preoperative hemoglobin <12.5g/dL, DM presence, N-classification, primary tumor locationand extension, and no prior Rt were not associ-ated with fistula development, but increased the CDR’s prognosticaccuracy (regarding the balance of sensitivity-specificity)andthuswerealsoincluded.
Themodelthereforeincludedallpre-operativevariables analyzedthatpresentedap-value<0.2andallthose consid-eredimportantbyasystematicreviewpreviouslyconducted by this team.4 The best results were obtained using the
followingmodel:
Riskscore=(4.98×ASAclassification)
+(1.97×alcoholconsumption)
+(5.10×chemoradiotherapy)
+(2.40×tracheotomy)
+(0.75×hemoglobinpre-surgery)
+(0.69×localextension)
+(1.01×N-classification)
+(0.75×presenceofDM)
+(3.03×albuminpre-surgery).
ThismodelpresentedanAUCof0.74(95%CI0.61---0.86), asshowninFig.1.
The model’sscorestratification intofour differentrisk categoriesisproposed:lowrisk(forascore≤9.88),
medium-low(9.881---12.25),medium-high(12.26---17.1),andhighrisk (score>17.1).Thisstratification resultedintheprognostic accuracyvaluesinTable4.Thevaluesforthecut-offswere selectedbyanassessmentofAUCcoordinates,usingthose thatprovidedbestfit.
Approximately half of the participants (48%) who developed a pharyngocutaneous fistula were classified as high risk. By associating the three highest risk groups (high+medium-high+medium-low),92%offistula develop-ment was predicted. It was also observed that with an increasein the riskdegree, more subjectsdevelop fistula (p<0.001forchi-squaredinanassociationandtrend analy-sis).
Ahighspecificityforthehigh-riskgroup(93%)wasnoted, withmoderatelyhighpositivelikelihoodratio(LR+)of(7.10) andpositive(PPV)andnegativepredictivevalues(NPV)with highresults(76%and79%respectively)(Table5).Withthe threegroupsofmedium-low/medium-high/highrisk,a sen-sitivityof92%, negativelikelihoodratio(LR-)of0.25,and NPVof89%wereobtained.
ThemeasuresofprognosticvalidityforASAclassification werealsocalculated,inordertocomparewiththeresultsof Farwelletal.8;thesevaluesareshowninTable6.Thus,this
Table3 Univariateandmultivariateanalysisoftherelationshipbetweenthevariablesincludedintheclinicaldecisionrule andthefrequencyofpharyngocutaneousfistula.
Variables All
n(%)
Withfistula n(%)
Withoutfistula n(%)
Univariateanalysis p-Value
Multivariateanalysis p-Value
ASA
2 107(63) 25(51.1) 82(68) 0.05a 0.005
3 62(36.2) 23(48.9) 39(32)
Alcohol
Heavy 126(73.7) 38(79.2) 88(71.5) 0.34a 0.361
Hemoglobinpre
<12.4g/dL 65(39.6) 22(48.9) 43(36.1) 0.15a 0.665
Albuminpre
<37.0g/L 30(34.1) 7(25) 23(38.3) 0.24a 0.07
Comorbidities
DM 25(14.6) 8(16.7) 17(13.8) 0.63a 0.72
COPD 18(10.5) 3(6.2) 15(12.2) 0.4a
Liverdisease 39(22.8) 11(22.9) 28(22.8) 1a Cardiopathy 42(24.6) 11(22.9) 31(25.2) 0.85a N
N0 83(48.6) 21(43.8) 62(50.4) 0.25b 0.933
N1 25(14.6) 8(16.7) 17(13.8)
N2a+N2b+N2c 58(33.9) 17(9.94) 41(23.96)
N3 5(2.9) 2(1.16) 3(1.74)
Location
Larynx 67(39.2) 18(10.5) 49(28.6) 0.86a 0.539
Pharyngolaryngeal 104(60.8) 30(62.5) 74(60.2) Rtpre
Yes 12(7.0) 4(8.3) 8(6.5) 0.74a
CRTpre
Yes 15(8.8) 9(18.8) 6(4.9) 0.01a 0.120
Tracheotomypre
Yes 77(45) 28(58.3) 49(39.8) 0.04a 0.144
Rt,radiotherapy;CRT,chemoradiotherapy;pre,preoperative;DM,diabetesmellitus;COPD,chronicobstructivepulmonarydiseases. aFisher’sexacttest.
b Chi-squaredtest.
Table4 Riskstratificationofdevelopingfistulapharyngocutaneousforthemodel.
Pharyngocutaneousfistula Riskgroups Total
Lowrisk Medium-lowrisk Medium-highrisk Highrisk
No 17(89%) 16(80%) 22(73%) 4(24%) 59
Yes 2(11%) 4(20%) 8(27%) 13(76%) 27
Total 19 20 30 17 86
Discussion
Clinical decision rules (CDR) are instruments used to increase health professionals’ accuracy in diagnostic and prognosticassessmentbysummarizingtheprobabilityofa particularoutcome.
Pharyngocutaneousfistularepresentsamajor postopera-tivecomplication of laryngectomizedpatients. Until now, noCDR has been derived for determining the risk of fis-tuladevelopment;consequently,thisstudywasconducted. As13variableswereincluded, theinclusionof130to195 participantswasrequired.The presentstudy included171
patients, which should be an adequate number.5 It was
decidedto use fourcategories in ordertomaintain equi-librium between the best fit of the model and clinical application; i.e., on one hand, with a higher number of categories, theclassificationcan beadjusted more effec-tivelytotheoriginalscore’sAUC;ontheotherhand,clinical applicabilityimproveswithalowernumberofcategories.
Inthisanalysis,theincidenceofthepharyngocutaneous fistulawas28.1%,whichisbetweenthevaluesobtainedby otherauthors.9---14
T able 5 Risk stratification of modelCat2 and validity measures for the different cut-offs. Cut-off
Fistulas n(%)
Se % (95% CI) Spec % (95% CI) LR+ (95% CI) LR − (95% CI) PPV % (95% CI) PNV % (95% CI) High risk (4) 13 (48) 48 (29---67) 93 (86---99) 7.10 (2.5---19.7) 0.55 (0.38---0.80) 76 (56---96) 79 (70---89) Medium-high (3) + high risk (4) 21 (77) 77 (62---93) 55 (43---68) 1.76 (1.2---2.5) 0.39 (0.18---0.83) 44 (30---58) 84 (73---95) Medium-low (2) + medium-high (3) + high risk (4) 25 (92) 92 (82---102) 28 (17---40) 1.30 (1.0---1.5) 0.25 (0.06---1.03) 37 (25---48) 89 (75---103) Se, sensibility; Spec, specificity; LR+, positive likelihood; LR − , negative likelihood; PPV , positive predictive value; PNV , negative predictive value; 95% CI, 95% confidence interval.
the10thtothe15thpostoperativeday,asdemonstratedin 38%ofthepresentcases.1,15---23
This analysis has shown, in agreement with other studies,17,24,25thatfortheadvancedstage(IVaandIVb)there
seemstobeahigherfistulaincidence.Thisrelationshipwas notstatisticallysignificantbothinthepresentaswellasin otherstudies.1,10---13,15,16,18---23,26---29
TheunivariateanalysisconfirmedthatCRTandprior tra-cheotomyarefactorsassociatedwithformationof pharyn-gocutaneous fistula, as did other authors.9,12,13,24,26,30,31
Tracheotomy previous to the operation was not con-sidered a risk factor for the fistulization by several authors15,18,20---22,25---28,31 contrary to the present findings.
In performing the multivariate analysis, these variables remained as potential predictive factors for the fistula development,asotherauthorshaveconcluded.24,30
Intheunivariateanalysis,radiotherapypriortosurgery wasnot significantfor pharyngocutaneous fistula develop-ment,asotherauthorsconcluded.2,11,14,18,20,21,25---29,32,33Their
inclusioninthefinalmodeldidnotaddsignificantchanges inaccuracy,thustheywereexcluded.
ASAclassification,unlikeotherstudies,8,21,34was
signifi-cantasariskfactorforfistuladevelopmentintheunivariate andmultivariateanalysis,whichdemonstratesthatthe pres-enceofpre-operativeco-morbiditiesandfunctionalstatus ofthepatienthaveamajorimportanceinthedevelopment ofintra-andpost-surgicalcomplications.
Few authorshave assessedtheASA classification’s pre-dictive value8 for this outcome, although its relevance
has been demonstrated in the present sample, reflecting the key role of the pre-operative control of comorbidi-ties.Paradoxically,evaluatingeachcomorbidityseparately (DM,COPD,liverdisease,andheartdisease),theydidnot demonstrate significant association with fistula develop-ment (both in the univariate and multivariate analysis). Inthis aspect, the available evidence is contradictory, as some authors reported the same results11,13 while others
found a significant relationship between fistula andthese comorbidities.1,12,15,16,20,21,34
After the multivariate analysis, pre-operative hypoal-bumin (<3.7g/L) was an independent factor for the development of the pharyngocutaneous fistula, as other authorsconcluded.12,15,20,34
Intheavailableliterature,itwasnotpossibletofinda CDRdeveloped specificallyfor stratifyingpatientsbytheir riskofpharyngocutaneousfistulaformationafter pharyngo-laryngectomyandtotallaryngectomy.
Forthehigh-riskgroup,ahighspecificitywasobserved, andtherefore the ability todetermine amongpatients at highestriskthosewhowillnotdeveloppharyngocutaneous fistula.However,themodelidentifiedwithhighsensitivity thegroupsofmedium-low+medium-high+highrisksubjects whowilldevelopafistula.Inahospitalsetting,thisallows thedistribution of economic andpersonnel resources pri-marilytopatientswithhigherprobabilityfortheoccurrence of postoperative complications. It also allows healthcare professionalstoactmoreintensivelyandearlierinthe pre-operativeand post-operativeperiodin ordertoassistthe identifiedtheriskgroup.
Table6 RiskstratificationoftheAmericanSocietyofAnesthesiologistsclassificationandprecisionmeasurements.
ASA Fistula n(%)
Se% (95%CI)
Spec% (95%CI)
LR+ (95%CI)
LR− (95%CI)
PPV% (95%CI)
NPV% (95%CI)
ASA3 23(48.9) 47(33---62) 67(59---76) 1.48(1---2.2) 0.76(0.57---.03) 37(25---49) 76(68---84)
Se,sensitivity;Spec,specificity;LR+,positivelikelihood;LR−,negativelikelihood;PPV,positivepredictivevalue;NPV,negative
predic-tivevalue;95%CI,95%confidenceinterval.
targetedtothehealingthiscomplicationareatremendous financialburdenonanyhealthcaresystem.
It should be emphasized that the derived model has somelimitations. Thecollectionof thevariableswas per-formedretrospectivelyandthereforewasnotascomplete andaccurateasitwouldhavebeenwithaprospectivebasis. Examplesincludetheabsenceofalbumininthe preopera-tiverecordsof85patientsandthelackofobservedrecords tocharacterize the nutritionalstatus of the patientprior to surgery. Regardless of the limiting factors, a CDR has beendevelopedforeasyapplicationwithrobustvaluesfor prognosticaccuracy,namelytheAUCvalueof0.76(95%CI 0.64---0.87).
Final
considerations
Wehavestatisticallycalculatedamathematicalmodelwith a good accuracy to detect the groups with medium/high riskof pharyngocutaneous fistuladevelopment. Ulteriorly, itwill allow abestdistribution of economic andpersonal resources targeting to patients withhigher probability of thiscomplicationoccurrence.Thesestudy’majorstrengths arethefactthatitrepresentsfirstadequateandspecifically CDRderivedforthepharyngocutaneousfistuladevelopment riskstratification thatadditionallypresentedrobustvalues ofprognosticvalidity.Themajorlimitationsofthestudyare itsretrospectiveandunicenterdesignandamodestsample size.Despite these limitations our CDR outperformed the ASA classification--- whichwas validatedfor this outcome prediction.
ThisCDRispresentedasaproposalforalaterprospective multicentervalidation,reliabilityassessmentand optimiza-tion. We also wish to assess their applicability practice amonghealthprofessionalsandthereforemakeaneconomic impactandease ofuseanalysisof implementationamong healthservicesinourcountry.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
Theauthorswouldliketothankallthestaffofthehospital thathelpedintheexecutionofthisstudy.Thisworkwasa partofaMaster’s ThesisinEvidence-basedMedicine from theUniversityofMedicineofPorto.
References
1.Galli J, De Corso E, Volante M, Almadori G, Paludetti G. Postlaryngectomy pharyngocutaneous fistula: incidence,
predisposingfactors,andtherapy.OtolaryngolHeadNeckSurg. 2005;133:689---94.
2.Makitie AA, Niemensivu R, Hero M, Keski-Santti H, Back L, KajantiM,etal.Pharyngocutaneousfistulafollowingtotal laryn-gectomy:a single institution’s 10-year experience.Eur Arch Otorhinolaryngol.2006;263:1127---30.
3.EstebanF,Delgado-RodriguezM,MochonA,SolanoJ,Soldado L, Solanellas J. Study of in-patient hospital stay follow-ing total laryngectomy: multivariable retrospective analysis of a 442 total laryngectomies. Acta Otorrinolaringol Esp. 2006;57:176---82.
4.Cecatto SB, Soares MM, Henriques T, Monteiro E, Moura CI. Predictivefactorsforthepostlaryngectomypharyngocutaneous fistuladevelopment:systematicreview.BrazJ Otorhinolaryn-gol.2014;80:167---77.
5.ConcatoJ,FeinsteinAR,HolfordTR.Theriskofdeterminingrisk withmultivariatemethods.AnnInternMed.1993;118:201---10.
6.HuY,XiongCL,ZhangZJ,BergquistR,WangZL,GaoJ,etal. Comparisonofdata-fittingmodelsfor schistosomiasis:acase studyinXingzi,China.GeospatHealth.2013;8:125---32.
7.Li Y, Yan J, Li M, Xiao Z, Zhu X, Pan J, et al. Addition ofSNAP to perinatalrisk factors improves theprediction of bronchopulmonarydysplasia ordeathincritically illpreterm infants.BMCPediatr.2013;13:138,http://dx.doi.org/10.1186/ 1471-2431-13-138.
8.FarwellDG, Reilly DF, WeymullerEA, Greenberg DL,Staiger TO, Futran NA. Predictors of perioperative complications in head and neck patients. Arch Otolaryngol Head Neck Surg. 2002;128:505---11.
9.Dirven R, Swinson BD, Gao K, Clark JR. The assessment of pharyngocutaneous fistula rate in patients treated primarily withdefinitiveradiotherapyfollowedbysalvagesurgeryofthe larynxandhypopharynx.Laryngoscope.2009;119:1691---5. 10.JeannonJP,OrabiA,ManganarisA,SimoR.Methicillinresistant
Staphylococcusaureusinfectionasacausativeagentoffistula formationfollowingtotallaryngectomy foradvancedhead& neckcancer.HeadNeckOncol.2010;2:14.
11.ParikhSR,IrishJC,CurranAJ,GullanePJ,BrownDH,Rotstein LE.Pharyngocutaneousfistulae inlaryngectomypatients:the TorontoHospitalexperience.JOtolaryngol.1998;27:136---40. 12.TsouYA,HuaCH,LinMH,TsengHC,TsaiMH,ShahaA.
Compar-isonof pharyngocutaneousfistula betweenpatientsfollowed byprimarylaryngopharyngectomyandsalvage laryngopharyn-gectomy for advanced hypopharyngeal cancer. Head Neck. 2010;32:1494---500.
13.WakisakaN,MuronoS,KondoS,FurukawaM,YoshizakiT. Post-operativepharyngocutaneousfistulaafterlaryngectomy.Auris NasusLarynx.2008;35:203---8.
14.WeingradDN,SpiroRH.Complicationsafterlaryngectomy.Am JSurg.1983;146:517---20.
15.Boscolo-RizzoP,DeCillisG,MarchioriC,CarpeneS,DaMosto MC.Multivariateanalysisofriskfactorsforpharyngocutaneous fistula after total laryngectomy. Eur Arch Otorhinolaryngol. 2008;265:929---36.
17.GrauC,JohansenLV,HansenHS,AndersenE,GodballeC, Ander-senLJ, et al. Salvage laryngectomy and pharyngocutaneous fistulaeafterprimaryradiotherapyforheadandneckcancer:a nationalsurveyfromDAHANCA.HeadNeck.2003;25:711---6. 18.MarkouKD,VlachtsisKC,NikolaouAC,PetridisDG,KouloulasAI,
DaniilidisIC.Incidenceandpredisposingfactorsof pharyngocu-taneousfistulaformationaftertotallaryngectomy. Istherea relationshipwithtumorrecurrence?EurArchOtorhinolaryngol. 2004;261:61---7.
19.Papazoglou G, Doundoulakis G, Terzakis G, Dokianakis G. Pharyngocutaneous fistula after total laryngectomy: inci-dence, cause, and treatment. Ann Otol Rhinol Laryngol. 1994;103:801---5.
20.Pinar E, Oncel S, Calli C, Guclu E, Tatar B. Pharyngocuta-neousfistulaaftertotallaryngectomy:emphasisonlymphnode metastasesasa newpredisposingfactor.JOtolaryngolHead NeckSurg.2008;37:312---8.
21.Redaelli de Zinis LO, Ferrari L, Tomenzoli D, Premoli G, ParrinelloG,NicolaiP.Postlaryngectomypharyngocutaneous fis-tula:incidence,predisposingfactors,andtherapy.HeadNeck. 1999;21:131---8.
22.SakiN,NikakhlaghS,KazemiM.Pharyngocutaneousfistulaafter laryngectomy:incidence,predisposingfactors,and outcome. ArchIranMed.2008;11:314---7.
23.VirtaniemiJA, Kumpulainen EJ, HirvikoskiPP, Johansson RT, Kosma VM. The incidence and etiology of postlaryngectomy pharyngocutaneousfistulae.HeadNeck.2001;23:29---33. 24.KlozarJ,CadaZ,KoslabovaE.Complicationsoftotal
laryngec-tomyintheeraofchemoradiation.EurArchOtorhinolaryngol. 2012;269:289---93.
25.SoyluL,KirogluM,AydoganB,CetikF,KirogluF,AkcaliC,etal. Pharyngocutaneousfistulafollowinglaryngectomy.HeadNeck. 1998;20:22---5.
26.DedivitisRA,RibeiroKC,CastroMA,NascimentoPC. Pharyngo-cutaneousfistulafollowingtotallaryngectomy.Acta Otorhino-laryngolItal.2007;27:2---5.
27.Ikiz AO, Uca M, Guneri EA,Erdag TK, Sutay S. Pharyngocu-taneousfistulaand totallaryngectomy:possiblepredisposing factors,withemphasisonpharyngealmyotomy.JLaryngolOtol. 2000;114:768---71.
28.Qureshi SS, Chaturvedi P, Pai PS, Chaukar DA, Deshpande MS, PathakKA, et al. A prospective study of pharyngocuta-neousfistulasfollowingtotallaryngectomy.JCancerResTher. 2005;1:51---6.
29.Saydam L, Kalcioglu T, Kizilay A. Early oral feeding fol-lowing total laryngectomy. Am J Otolaryngol. 2002;23: 277---81.
30.HorganEC,DedoHH.Preventionofmajorand minorfistulae afterlaryngectomy.Laryngoscope.1979;89:250---60.
31.Paydarfar JA, Birkmeyer NJ. Complications in head and neck surgery: a meta-analysis of postlaryngectomy pharyn-gocutaneous fistula. Arch Otolaryngol Head Neck Surg. 2006;132:67---72.
32.MortonRP,MehannaH,HallFT,McIvorNP.Predictionof pharyn-gocutaneousfistulasafterlaryngectomy.OtolaryngolHeadNeck Surg.2007;136:S46---9.
33.Palomar-Asenjo V, Sarroca Capell E, Tobias Gomez S, Perez HernandezI,Palomar-GarciaV.Pharyngocutaneousfistula fol-lowingtotallaryngectomy.Acase---controlstudyofriskfactors implicated in its onset. Acta Otorrinolaringol Esp. 2008;59: 480---4.