w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Review
article
Primary
myelofibrosis:
current
therapeutic
options
Paula
de
Melo
Campos
∗UniversidadeEstadualdeCampinas(Unicamp),Campinas,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received4April2016 Accepted5April2016 Availableonline27April2016
Keywords:
Myeloproliferativedisorders Primarymyelofibrosis Januskinase2
a
b
s
t
r
a
c
t
PrimarymyelofibrosisisaPhiladelphia-negativemyeloproliferativeneoplasmcharacterized byclonalmyeloidexpansion,followedbyprogressivefibrousconnectivetissuedepositionin thebonemarrow,resultinginbonemarrowfailure.Clonalevolutioncanalsooccur,withan increasedriskoftransformationtoacutemyeloidleukemia.Inaddition,disabling constitu-tionalsymptomssecondarytothehighcirculatinglevelsofproinflammatorycytokinesand hepatosplenomegalyfrequentlyimpairqualityoflife.Hereinthemaincurrenttreatment optionsforprimarymyelofibrosispatientsarediscussed,contemplatingdisease-modifying therapeuticsinadditiontopalliativemeasures,inanindividualizedpatient-basedapproach. ©2016Associac¸ ˜aoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Overview
Primarymyelofibrosis(PMF)isaPhiladelphia-negative myelo-proliferativeneoplasm(MPN)withapredominant prolifera-tionofmegakaryocytesandgranulocytesinthebonemarrow characterizedbyaninitialproliferativephase,followedbya reactive deposition of fibrous connective tissue inthe ter-minalphase.1Bonemarrowfailure,thromboembolicevents
and transformation to acute myeloid leukemia (AML) are the maincauses ofmorbi-mortality inPMF, but additional symptomssecondarytohepatosplenomegalyandabnormal blood counts frequently impair quality of life.1,2 The high
circulating levels of proinflammatory cytokines also result indisabling constitutional symptoms (fatigue,weight loss, nightsweats,fever,pruritus,arthralgias,myalgias).2Hence,
thedecisionregardingthebesttreatmentcombinationinPMF mustbeindividualized,takingthesymptoms,risksandlife expectationofeachpatientintoaccount.Despitetherecent
∗ Correspondenceat:HematologyandHemotherapyCenter,UniversidadeEstadualdeCampinas(Unicamp),RuaCarlosChagas,480,
13083-878Campinas,SP,Brazil.
E-mails:[email protected],[email protected]
advancesinthedevelopmentoftargetedtherapies,allogeneic hematopoieticstemcelltransplantation(allo-HSCT)remains the onlycurativeoptionavailableforPMF. Evidenceon the maintherapeuticoptions forPMFwillbediscussedin this article.
Molecular
characterization
Althoughno molecularlesioncan specificallyidentifyPMF, somerecurrentmutationsare foundand arehelpfulinthe diagnosis and theprognostic stratificationofPMFpatients.
JAK2 (Janus kinase 2),MPL (thrombopoietinreceptor)and CALR
(calreticulin) genes frequently harbor somatic mutations in PMF,whichinducetheconstitutiveactivationoftheJAK-STAT, PI3Kand ERKpathwaysinaligand-independentway, lead-ingtoincreasedmyeloidproliferation.Approximately50–60% ofPMFpatientsexhibittheJAK2V617Fmutation.3–5 A
gain-of-function mutationin MPL(MPLW515K/L), which encodes the
http://dx.doi.org/10.1016/j.bjhh.2016.04.003
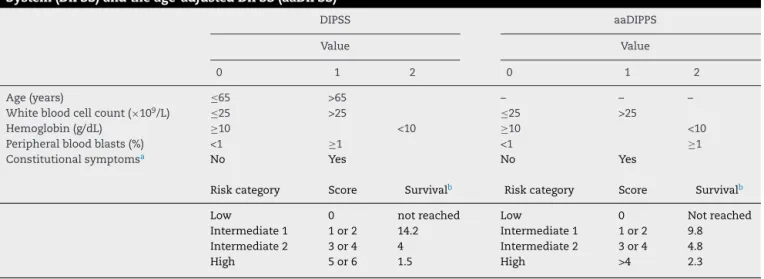
Table1–RiskstratificationofprimarymyelofibrosispatientsaccordingtotheDynamicInternationalPrognosticScoring System(DIPSS)andtheage-adjustedDIPSS(aaDIPSS)16
DIPSS aaDIPPS
Value Value
0 1 2 0 1 2
Age(years) ≤65 >65 – – –
Whitebloodcellcount(×109/L) ≤25 >25 ≤25 >25
Hemoglobin(g/dL) ≥10 <10 ≥10 <10
Peripheralbloodblasts(%) <1 ≥1 <1 ≥1
Constitutionalsymptomsa No Yes No Yes
Riskcategory Score Survivalb Riskcategory Score Survivalb
Low 0 notreached Low 0 Notreached
Intermediate1 1or2 14.2 Intermediate1 1or2 9.8 Intermediate2 3or4 4 Intermediate2 3or4 4.8
High 5or6 1.5 High >4 2.3
a 10%weightlossinsixmonths,nightsweats,unexplainedfeverhigherthan37.5◦C.
b Median,years.
thrombopoietinreceptorand isakeyfactorforgrowthand survivalofmegakaryocytes,hasbeen reportedinup to5% ofPMFcases.6,7MPLmutationsmayoccurconcurrentlywith
theJAK2V617Fmutation.8Approximately60–80%ofJAK2and
MPLwildtypepatientsharborCALRmutations.9,10Additional
mutationsinepigeneticregulators,suchasTET2,11ASXL1,12
DNMT3A,13 IDH1/2,14 havebeen described inMPN patients
atvariable frequenciesandtheirprognosticvaluehasbeen objectofstudies.15
Risk
stratification
Adequate riskstratificationinPMFisessential toestablish themostsuitabletreatmentforaparticularpatient,taking therisk-benefitofeachapproachintoaccount.Inthissense, theDynamicInternationalPrognosticScoringSystem(DIPSS) for PMFis widely used in the clinical practice. DIPSS is a dynamicprognosticmodelthatconsidersmodificationsinthe riskprofileafterdiagnosisandcanpredictprognosisat differ-entstagesofthedisease(Table1).16Theage-adjustedDIPSSis
avariationspecificallydevelopedforyoungerpatients(age<65 years),comprisingthegroupthatismostcommonlysuitable forintensivetherapiessuchasallo-HSCT(Table1).16
Treatment
options
Hydroxyurea
Hydroxyurea (HU) is a non-alkylating antineoplastic agent used for cytoreduction in myeloproliferative neoplasms. AlthoughtherearefewwelldesignedstudiesevaluatingHU benefitsinmyelofibrosispatients,hydroxyureaisfrequently usedtoattenuatehyperproliferativemanifestationsrelatedto PMF.17 Inagroupof40PMFpatients, Martinez-Trilloset al.
showedsignificantresponserates,withreductionsin consti-tutionalsymptoms(55%),symptomaticsplenomegaly(45%), thrombocytosis (40%) and leukocytosis (28%); accentuation
of anemia was the mostcommon adverse event, and was observed inalmost halfof the patients.17 When HU
resis-tance/refractorinessisdocumentedinthePMFproliferative phase,switchingfromHUtoamoleculartargetedtherapy(i.e., JAK1/2inhibitor)shouldpromptlybeconsidered.18The
crite-riafor resistanceandrefractoriness toHU inPMFpatients havepreviouslybeendefinedbytheEuropeanLeukemiaNet consensus.18
Supporttherapy
Anemia
Anemia is a frequent manifestation of PMF19 that might
be caused by different interacting factors, such as bone marrowinsufficiency(fibrosis),hypersplenism,bleeding,iron deficiency, vitaminB12or folatedeficiency, orautoimmune hemolysis.20,21Moreover,specificPMFtreatmentwith
cytore-ductivedrugs(HU)17 andJAK1/2inhibitors22canleadto,or
increase, anemia in these patients. Besides correcting the potentially reversiblecauses ofanemia, some other thera-peutic possibilitiesmight beconsidered when anemia isa disablingsymptom.Someofthemarediscussedbelow.
a.Androgens
Androgenshavebeen usedtotreatanemia inPMFwith variableresponserates;mostofthestudiesdescribedresults observedinsmallcohorts.Danazol,asemisynthetic attenu-atedandrogenthathasfewersideeffects,resultsinananemia responserateof30–57%dependingontheadoptedresponse criteria.21,23,24Inacohortof50patientswithPMF,Cervantes
etal.21describeda30%responserate[definedbytransfusion
cessation intransfusion-dependent patientsor anincrease in hemoglobin(Hb)>2g/dL inpatients without transfusion requirements],withamedianduration ofanemiaresponse of14months.Androgensshouldnotbeusedinpatientswith prostaticsymptoms,prostatecancerormoderatetoadvanced hepaticdisease.
b.Erythropoiesis-stimulatingagents
causes,theexperienceinPMFisrelativelysmallandbasedon studieswithlimitedsamplesizes.Reportedoverallresponse rates range from 23% to60%.25–28 Hb <10g/dL,transfusion
independence,25,27andEPOlevels<125U/L27arefactorsthat
mightconferabetterresponsetotreatment.However,these data needto be validated in larger cohorts using uniform responsecriteria.
c.Immunomodulatingdrugs
Thalidomidehasshowneffectivenessinawidespectrum ofneoplasmsduetoitsanti-angiogenicandimmunological effects. Previous reports using high doses of thalido-mide (100–400mg) in PMF have demonstrated encour-aging responses regarding the improvement of anemia (20%–60%),thrombocytopenia(38%–80%), andsplenomegaly (25%–41%).29–32However,thehighlevelofsideeffects
(somno-lence,fatigue,edema,constipation,neurologicalsymptoms, neutropenia) significantly reduced tolerability.29,30,32,33 The
useoflowdosesofthalidomide(50–100mg)associatedornot withprednisone (0.5mg/kg/day) can decrease toxicity with similarresponserates.34–36Lenalidomide,athalidomide
ana-log,hasbeendescribedasanadditionaltherapeuticoption, withresponseratesrangingfrom19–30%foranemia,0–50% for thrombocytopenia and 10–42% for splenomegaly,37–39
according to the scheduled dose and the response crite-riaadopted.Recently,Daveretal.40evaluatedthecombined
effect oflenalidomide plus the JAK1/2 inhibitor ruxolitinib in31patientswithPMF;however, thestudy hadtobe dis-continuedprematurely duetotheelevatednumber ofdrop outs(23patients)duetodrugtoxicity.40Amongthepatients
whodidnotrequireearlydose interruption,responserates were high (73%), suggesting that additional studies using lower doses of lenalidomide and ruxolitinib might be of interest.40Moreover,aretrospectivestudybyJabbouretal.41
that evaluated three previous phase 2 clinical trials com-pared the efficacy of thalidomide and lenalidomide-based therapies, and observed overall response rates of16% and 34–38%, respectively, according to the International Work-ing Group (IWG) forMyelofibrosisTreatment and Research criteria.Inaddition,lenalidomideplusprednisoneimproved responsedurationwhencomparedtoboththalidomideand lenalidomidesingleagenttherapies,suggestingthat lenalido-mide plusprednisone might be a reasonableoption when decidingforimmunomodulatingdrugs.41Pomalidomideisa
potentsecond-generationimmunomodulatingdrugthathas a better toxicity and safety profile than thalidomide and lenalidomide,42 and has been tested in PMF in few
stud-ieswithvaryingresults.Anemiaresponseratesrangedfrom 10–37%,42–47butincreasedto53%inasinglereportthat
specif-icallyanalyzedthegroupofJAK2V617F-positivepatientswith
<10cm palpable splenomegaly and <5% circulating blasts, indicating that these factors might bepredictors of better response.44
d.Chronictransfusionandironchelation
Forthesymptomaticanemic patientsthatarerefractory tospecifictherapies,chronicredbloodcelltransfusionsmay improvesymptomsandqualityoflife.Forthetreatmentof secondary ironoverload intransfusion-dependent patients who have curative intentions (e.g. bone marrow trans-plantation) and/or higher life expectations, iron chelation shouldbeconsideredinordertopreventiron-inducedorgan
damage. Furthermore,ironchelation may promotean ery-throid response with increased Hb levels in some PMF patients,48albeitadditionalstudiesareneededtosupportthis
recommendation.
Splenomegaly
The enlarged spleen is a major source of discomfort and impairedqualityoflifeinPMF.Constitutionalsymptoms,pain, earlysatietyduetogastriccompression,portalhypertension and cytopenias arefrequentfindings inPMFinthe fibrotic phase.49,50 InPMFpatientswithanunsatisfactoryresponse
topharmacologicaltreatment,splenectomyandsplenic radi-ationmaybetreatmentoptions,asdiscussedbelow.
a.Splenectomy
Despitetheimprovementinperioperativemortality follow-ing splenectomyobservedinthelastdecades duetobetter patient selection, vaccination, antimicrobials and surgical procedures,splenectomydoesnotseemtoalterpatient sur-vivalanddiseaseevolution.49However,itmightbe
exception-allyindicatedforthepalliativecontrolofpersistentanemia, thrombocytopenia,portalhypertensionandpain.49,51Ina
ret-rospectiveanalysisof223patientssubmittedtosplenectomy atthe Mayo Clinicduring a20-year period, durable remis-sions in constitutional symptoms, transfusion-dependent anemia, portal hypertension,and severe thrombocytopenia wereachievedin67%,23%,50%,and0%ofthepatients, respec-tively,withratesofnonfatalcomplicationsof30.5%,including 7.2%ofthrombosis,and 8.9%offatalcomplications.51
San-tosetal.52 described,inacohortof94splenectomizedPMF
patients, improvements of anemia and thrombocytopenia in47% and66% ofthecases,respectively. Thrombosiswas observedin16%ofthepatients,andpost-operativemortality was5%,withaloweroverallsurvivalforthepatientsthatwere submittedtosplenectomyduringdiseaseevolution.52Since
splenectomyisassociatedwithsubstantialrisks,the proce-dureshouldonlybeconsideredforselectedpatientsfollowing stringentcriteriaincludingabsenceofseverecomorbidities, adequatelifeexpectancy,significantsplenicsymptomsthat affectqualityoflife,andfailureofatleastonepharmacological therapyforsplenomegaly.49
b.Splenicirradiation
Splenic irradiation is a palliative modality of treatment consideredasanalternativetosplenectomyinPMFpatients that havesymptomaticsplenomegaly and areineligiblefor surgical procedures. However, although spleen size reduc-tion and symptomreliefare observedinahigh proportion of patients, response to treatment is usually brief and transient.50,53Theworseningofpre-treatmentcytopeniasand
the emergence of infectious complications are frequently found.53
Additionalpalliativemeasures
Myelofibrosisseverelycompromisesqualityoflifeasaresult ofmarkedsplenomegaly,profoundconstitutionalsymptoms and cachexia.54 In a group of458 patients, including PMF
and post-polycythemia vera (PV)/post-essential thrombocy-topenia (ET) myelofibrosis, Mesaet al. foundan incidence of84%forfatigue,47%forbonepain,50%forpruritus,56% fornightsweats and54% forsymptomaticsplenomegaly.54
managementandevaluationofnutritionalstatus,are manda-toryadjuvanttherapies.
Interferon
Interferon has been described as a therapeutic option in the treatment of PMF patients, though only a limited number of studies evaluating the effects of interferon in larger PMF cohorts are available. Previous studies indi-cated that recombinant interferon-␣ has the potential to
decreasetheproliferationofPMFneoplasticstemcellswith a significant reduction of marrow fibrosis, cellularity and megakaryocytedensity,55,56whichcanresultinimprovements
of splenomegaly and blood counts.56,57 Systemic toxicity
(cytopenias,asthenia,fatigue,myalgia)maylimitinterferon useinaproportionofpatients;however,mostcasescanbe manageablewithdosereductions.55,56Largerstudiesare
nec-essarytofullysupportinterferonuseinPMFpatientsandits effectsonoverallsurvival.
JAK1/2inhibitors
Theactivation ofthe JAK-STATpathway inducedby muta-tions in JAK2, CALR and MPL genes has a central role in inducing cell proliferation in PMF,15 making this
path-way a potential target for directed therapies. Ruxolitinib, the first US Food and DrugAdministration (FDA)-approved oralJAK1/2inhibitorisgenerally well-tolerated,and signif-icantly reduces splenomegaly and ameliorates debilitating myelofibrosis-related symptoms.22,58 An evaluation of the
nutritionalstatusinintermediate-2orhighriskPMFpatients showed that ruxolitinib significantly increased weight and albuminlevels.59Themostcommonsideeffectsarea
dose-dependentanemia and thrombocytopenia,that are usually manageablewithdosereductions.22,58Athree-yearfollowup
analysisofthecontrolledmyelofibrosisstudywithoralJAK inhibitor (COMFORT-I) – a double-blind, placebo-controlled trialthatpreviouslysuggestedasurvivalbenefitforthe ruxoli-tinibgroup58–reportedthatruxolitinibsignificantlyimproved
qualityoflife,reducedspleenvolumeandimprovedsurvival ofpatientswithintermediate-2orhighriskPMFwhen com-paredtoplacebo.60However,arecentCochranemeta-analysis
suggestedthatthereisinsufficientdatafordefinitive conclu-sionsregardingthebenefitsofruxolitinibonthesurvivalof PMFpatients.61Future updatesinruxolitinibstudies
show-inglongerfollow-uptimeswillbeofvaluetoallowdefinitive conclusionsregardingsurvivalbenefits.In ordertoidentify genesthatmaypredictresponsetoruxolitinibinmyelofibrosis patients,Pateletal.62screenedmutationsin28genes
recur-rentlymutatedinhematologicmalignancies,andfoundthat patientswith≥3mutationshadpoorerresponsesto
ruxoli-tinibandshorteroverallsurvival.62DespiteotherselectiveJAK
inhibitorshavingbeensubmittedtoclinicaltrialswith promis-ingresults63,64nonehavebeenapprovedforclinicaluseuntil
thepresent.
Bonemarrowtransplantation
Allo-HSCT is currently the only curative treatment option formyelofibrosis patients. Allo-HSCTshould beconsidered
in intermediate-2/high risk patients, and in patients with refractorydisease,adversecytogeneticsor>2%blastsinthe peripheralblood.65–68Althoughage>45yearsisdescribedas
anadverseprognosticfactorfortransplantationinPMF,66
allo-HSCTcanbeconsideredforindividualsyoungerthan70years old who have good performancestatus and no significant comorbidities.65 Previous studies have demonstrated that
unrelateddonor, post-transplanttransfusion dependence,66
and JAK2V617F levels>1%onemonthaftertransplantation67
are prognostic factors that adversely affect overall survival.
Special
situations
Post-polycythemiaveraandpost-essential thrombocythemiamyelofibrosis
PV andETare MPNwhich canevolvetomyelofibrosisasa disease-relatedcomplication,69withanincidenceofevolution
tofibrosisover15yearsof5–14%69,70and9.3%,69,71,72
respec-tively. Post-PV and post-ET myelofibrosis are molecularly distinct but phenotypicallysimilar to PMF,with equivalent clinical courses; for this reason, most clinical trials group patientsofthesethreediseasecategories intheircohorts.2
Currently,therearenospecifictherapeuticsforpost-PVand post-ETmyelofibrosis,andthesepatientsshouldbetreated similarlytoPMFpatients.2,73
Autoimmunemyelofibrosis
Autoimmunemyelofibrosis(AMF)isabenigncauseofbone marrowfibrosisassociatedwithautoimmunedisorders,such assystemiclupuserythematosus,scleroderma,Sjogren’s syn-drome, Hashimoto thyroiditis, autoimmune hepatitis, and Evans syndrome.74 AMF can also be found in patients
withno well-establisheddiagnosisofautoimmune disease, usuallyassociatedwithelevatedtitersofantinuclear antibod-ies,rheumatoid factor,and/orapositivedirectantiglobulin test.74,75 It is characterizedby reticulin marrow fibrosis in
theabsenceofclusteredoratypicalmegakaryocytesorother clinicopathologicalfeaturesofhematologicalmalignancies.76
AMFusuallyrespondstocorticosteroidtherapywitha gen-erally good prognosis.74,76 A course of prednisone starting
at 1mg/kg/day and tapered over 1–3 months can resultin completenormalizationofperipheralbloodcounts.76,77Cases
with partial response to corticosteroids appear to benefit from theaddition ofanother immunosuppressiveagent.In general, results ofsteroid therapy have been less impres-siveinAMFassociatedwithsystemiclupuserythematosus. Althoughreductionofbonemarrowfibrosisafter immunosup-pressivetreatmentmaybeobserved,thecompleteresolution ofbonemarrowfibrosisisnotnecessaryfortherecoveryof peripheralbloodcytopenias.76Consideringthedifferencesin
PMF DIPSS risk group
Low intermediate-1
Intermediate-2 high
Asymptomatic Symptomatic
Watch and wait + +
Symptom-directed treatment
JAK inhibitors Allo-SCT
Treatment failure Allo-SCT eligible Disease progression
Age Comorbidities Performance status Patients’ preferences
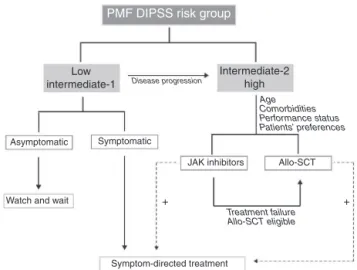
Figure1–Proposedtreatmentalgorithmforprimary
myelofibrosispatientsaccordingtoDIPSSriskgroups. Therapeuticdecisionstaketheriskgroupandpatients’ particularitiesintoaccount.Thepalliationofsymptoms
needstobecontinuouslypursued,independentlyofthe
therapeuticchoice,andareadditivetodisease-modifying treatment,asindicatedbythedottedlines.PMF:primary myelofibrosis;DIPSS:DynamicInternationalPrognostic ScoringSystem;Allo-HSCT:allogeneicstemcell transplantation.
Treatment
decision
–
when
and
whom?
AsymptomaticPMFpatients inthe lowand intermediate-1 riskgroupsaccordingtoDIPSShavealongexpectedsurvival anddonotusuallyrequirespecifictreatment.Ifsymptomatic, patientsintheseriskcategoriescanbetreatedaccordingto theprevailingsymptom,asdiscussedabove.Intermediate-2 andhigh-riskDIPSSpatientshaveashortenedsurvivaland shouldbeconsidered fordisease-modifyingtherapies, such asJAKinhibitorsandallo-HSCT,whentolerated;thedecision betweenthesetwo optionshas tobeindividualizedtaking intoaccountthepatient’sage,performancestatusand prefer-ences.Combinationtherapiesforthepalliationofsymptoms, regardlessoftheriskgroupandtheprognosis,arebeneficial andshouldbeimplementedtoimprove patients’qualityof life.AtreatmentalgorithmisproposedinFigure1.
Conclusions
and
perspectives
Expressive progression has recently been achieved in the knowledge of the pathophysiology of primary myelofibro-sis, which has allowed the development of targeted-drugs thatmay alterdisease progression.Many molecule-specific drugsareunderdevelopmentorbeingtested,butcouldnot bediscussedhereinduetospacelimitations.JAKinhibitors haveshownpromisingresults,thoughadditionalstudiesand follow-uptimewillbeofvaluetofurthersupportsurvival ben-efits.Currently,allo-HSCTremainstheonlycurativeoption. Inapatient-basedapproach,thepalliationofthesymptoms isfundamentalfromdiagnosisuntilend-stagedisease.
Conflicts
of
interest
Theauthordeclaresnoconflictsofinterest.
Acknowledgements
TheauthorwouldliketothankRaquelS.FoglioforEnglish review, and Dr. SaraT. Olalla Saad from the University of CampinasandDr.FabiolaTrainafromtheUniversityofSão Paulo at Ribeirão Preto Medical School for their valuable collaboration.
r
e
f
e
r
e
n
c
e
s
1.ThieleJ,KvasnickaHM,TefferiA,BarosiG,OraziA,Vardiman, etal.Myelofibrosis.In:SwerdlowSH,CampoE,HarrisNL, JaffeES,PileriSA,SteinH,etal.,editors.WHOclassificationof tumoursofhaematopoieticandlymphoidtissues.Lyon: WHO;2008.p.44–7.
2.SavonaMR.Arewealteringthenaturalhistoryofprimary myelofibrosis?LeukRes.2014;38(9):1004–12.
3.JonesAV,KreilS,ZoiK,WaghornK,CurtisC,ZhangL,etal. WidespreadoccurrenceoftheJAK2V617Fmutationinchronic myeloproliferativedisorders.Blood.2005;106(6):2162–8.
4.KralovicsR,PassamontiF,BuserAS,TeoSS,TiedtR,Passweg JR,etal.Again-of-functionmutationofJAK2in
myeloproliferativedisorders.NEnglJMed. 2005;352(17):1779–90.
5.BaxterEJ,ScottLM,CampbellPJ,EastC,FourouclasN, SwantonS,etal.Acquiredmutationofthetyrosinekinase JAK2inhumanmyeloproliferativedisorders.Lancet. 2005;365(9464):1054–61.
6.PikmanY,LeeBH,MercherT,McDowellE,EbertBL,GozoM, etal.MPLW515Lisanovelsomaticactivatingmutationin myelofibrosiswithmyeloidmetaplasia.PLoSMed. 2006;3(7):e270.
7.PardananiAD,LevineRL,LashoT,PikmanY,MesaRA, WadleighM,etal.MPL515mutationsinmyeloproliferative andothermyeloiddisorders:astudyof1182patients.Blood. 2006;108(10):3472–6.
8.BoydEM,BenchAJ,Goday-FernandezA,AnandS,VaghelaKJ, BeerP,etal.ClinicalutilityofroutineMPLexon10analysisin thediagnosisofessentialthrombocythaemiaandprimary myelofibrosis.BrJHaematol.2010;149(2):250–7.
9.NangaliaJ,MassieCE,BaxterEJ,NiceFL,GundemG,Wedge DC,etal.SomaticCALRmutationsinmyeloproliferative neoplasmswithnonmutatedJAK2.NEnglJMed. 2013;369(25):2391–405.
10.Machado-NetoJA,deMeloCamposP,deAlbuquerqueDM, CostaFF,Lorand-MetzeI,OlallaSaadST,etal.Somatic mutationsofcalreticulininaBraziliancohortofpatientswith myeloproliferativeneoplasms.RevBrasHematolHemoter. 2015;37(3):211–4.
11.TefferiA,PardananiA,LimKH,Abdel-WahabO,LashoTL, PatelJ,etal.TET2mutationsandtheirclinicalcorrelatesin polycythemiavera,essentialthrombocythemiaand myelofibrosis.Leukemia.2009;23(5):905–11.
12.FisherCL,LeeI,BloyerS,BozzaS,ChevalierJ,DahlA,etal. Additionalsexcombs-like1belongstotheenhancerof trithoraxandpolycombgroupandgeneticallyinteractswith Cbx2inmice.DevBiol.2010;337(1):9–15.
14.PardananiA,LashoTL,FinkeCM,MaiM,McClureRF,TefferiA. IDH1andIDH2mutationanalysisinchronic-andblast-phase myeloproliferativeneoplasms.Leukemia.2010;24(6):1146–51.
15.LangabeerSE,AndrikovicsH,AspJ,BellosilloB,CarilloS, HaslamK,etal.Moleculardiagnosticsofmyeloproliferative neoplasms.EurJHaematol.2015;95(4):270–9.
16.PassamontiF,CervantesF,VannucchiAM,MorraE,RumiE, PereiraA,etal.Adynamicprognosticmodeltopredict survivalinprimarymyelofibrosis:astudybytheIWG-MRT (InternationalWorkingGroupforMyeloproliferative NeoplasmsResearchandTreatment).Blood. 2010;115(9):1703–8.
17.Martinez-TrillosA,GayaA,MaffioliM,Arellano-RodrigoE, CalvoX,Diaz-BeyaM,etal.Efficacyandtolerabilityof hydroxyureainthetreatmentofthehyperproliferative manifestationsofmyelofibrosis:resultsin40patients.Ann Hematol.2010;89(12):1233–7.
18.BarosiG,BirgegardG,FinazziG,GriesshammerM,HarrisonC, HasselbalchH,etal.Aunifieddefinitionofclinicalresistance andintolerancetohydroxycarbamideinpolycythaemiavera andprimarymyelofibrosis:resultsofaEuropean
LeukemiaNet(ELN)consensusprocess.BrJHaematol. 2010;148(6):961–3.
19.CervantesF,DupriezB,PereiraA,PassamontiF,ReillyJT, MorraE,etal.Newprognosticscoringsystemforprimary myelofibrosisbasedonastudyoftheInternationalWorking GroupforMyelofibrosisResearchandTreatment.Blood. 2009;113(13):2895–901.
20.ReillyJT.Pathogenesisandmanagementofidiopathic myelofibrosis.BaillieresClinHaematol.1998;11(4):751–67.
21.CervantesF,IsolaIM,Alvarez-LarranA,Hernandez-BoludaJC, CorreaJG,PereiraA.Danazoltherapyfortheanemiaof myelofibrosis:assessmentofefficacywithcurrentcriteriaof responseandlong-termresults.AnnHematol.
2015;94(11):1791–6.
22.HarrisonC,KiladjianJJ,Al-AliHK,GisslingerH,WaltzmanR, StalbovskayaV,etal.JAKinhibitionwithruxolitinibversus bestavailabletherapyformyelofibrosis.NEnglJMed. 2012;366(9):787–98.
23.CervantesF,Alvarez-LarranA,DomingoA,Arellano-Rodrigo E,MontserratE.Efficacyandtolerabilityofdanazolasa treatmentfortheanaemiaofmyelofibrosiswithmyeloid metaplasia:long-termresultsin30patients.BrJHaematol. 2005;129(6):771–5.
24.CervantesF,Hernandez-BoludaJC,AlvarezA,NadalE, MontserratE.Danazoltreatmentofidiopathicmyelofibrosis withsevereanemia.Haematologica.2000;85(6):595–9.
25.HuangJ,TefferiA.Erythropoiesisstimulatingagentshave limitedtherapeuticactivityintransfusion-dependent patientswithprimarymyelofibrosisregardlessofserum erythropoietinlevel.EurJHaematol.2009;83(2):154–5.
26.CervantesF,Alvarez-LarranA,Hernandez-BoludaJC,Sureda A,GranellM,VallansotR,etal.Darbepoetin-alphaforthe anaemiaofmyelofibrosiswithmyeloidmetaplasia.BrJ Haematol.2006;134(2):184–6.
27.CervantesF,Alvarez-LarranA,Hernandez-BoludaJC,Sureda A,TorrebadellM,MontserratE.Erythropoietintreatmentof theanaemiaofmyelofibrosiswithmyeloidmetaplasia: resultsin20patientsandreviewoftheliterature.BrJ Haematol.2004;127(4):399–403.
28.TsiaraSN,ChaidosA,BourantasLK,KapsaliHD,Bourantas KL.Recombinanthumanerythropoietinforthetreatmentof anaemiainpatientswithchronicidiopathicmyelofibrosis. ActaHaematol.2007;117(3):156–61.
29.BarosiG,GrossiA,ComottiB,MustoP,GambaG,MarchettiM. Safetyandefficacyofthalidomideinpatientswith
myelofibrosiswithmyeloidmetaplasia.BrJHaematol. 2001;114(1):78–83.
30.BarosiG,ElliottM,CanepaL,BalleriniF,PiccalugaPP,VisaniG, etal.Thalidomideinmyelofibrosiswithmyeloidmetaplasia: apooled-analysisofindividualpatientdatafromfivestudies. LeukLymphoma.2002;43(12):2301–7.
31.ElliottMA,MesaRA,LiCY,HookCC,AnsellSM,LevittRM, etal.Thalidomidetreatmentinmyelofibrosiswithmyeloid metaplasia.BrJHaematol.2002;117(2):288–96.
32.StruppC,GermingU,SchererA,KundgenA,ModderU, GattermannN,etal.Thalidomideforthetreatmentof idiopathicmyelofibrosis.EurJHaematol.2004;72(1):52–7.
33.CanepaL,BalleriniF,VaraldoR,QuintinoS,ReniL,ClavioM, etal.Thalidomideinagnogenicandsecondarymyelofibrosis. BrJHaematol.2001;115(2):313–5.
34.MesaRA,SteensmaDP,PardananiA,LiCY,ElliottM, KaufmannSH,etal.Aphase2trialofcombinationlow-dose thalidomideandprednisoneforthetreatmentof
myelofibrosiswithmyeloidmetaplasia.Blood. 2003;101(7):2534–41.
35.MarchettiM,BarosiG,BalestriF,ViarengoG,GentiliS,Barulli S,etal.Low-dosethalidomideamelioratescytopeniasand splenomegalyinmyelofibrosiswithmyeloidmetaplasia:a phaseIItrial.JClinOncol.2004;22(3):424–31.
36.WeinkoveR,ReillyJT,McMullinMF,CurtinNJ,RadiaD, HarrisonCN.Low-dosethalidomideinmyelofibrosis. Haematologica.2008;93(7):1100–1.
37.TefferiA,CortesJ,VerstovsekS,MesaRA,ThomasD,Lasho TL,etal.Lenalidomidetherapyinmyelofibrosiswithmyeloid metaplasia.Blood.2006;108(4):1158–64.
38.Quintas-CardamaA,KantarjianHM,ManshouriT,ThomasD, CortesJ,RavandiF,etal.Lenalidomideplusprednisone resultsindurableclinical,histopathologic,andmolecular responsesinpatientswithmyelofibrosis.JClinOncol. 2009;27(28):4760–6.
39.MesaRA,YaoX,CripeLD,LiCY,LitzowM,PaiettaE,etal. Lenalidomideandprednisoneformyelofibrosis:Eastern CooperativeOncologyGroup(ECOG)phase2trialE4903. Blood.2010;116(22):4436–8.
40.DaverN,CortesJ,NewberryK,JabbourE,ZhouL,WangX, etal.Ruxolitinibincombinationwithlenalidomideas therapyforpatientswithmyelofibrosis.Haematologica. 2015;100(8):1058–63.
41.JabbourE,ThomasD,KantarjianH,ZhouL,PierceS,CortesJ, etal.Comparisonofthalidomideandlenalidomideas therapyformyelofibrosis.Blood.2011;118(4):899–902.
42.DaverN,ShastriA,KadiaT,NewberryK,PemmarajuN, JabbourE,etal.PhaseIIstudyofpomalidomidein
combinationwithprednisoneinpatientswithmyelofibrosis andsignificantanemia.LeukRes.2014;38(9):1126–9.
43.DaverN,ShastriA,KadiaT,Quintas-CardamaA,JabbourE, KonoplevaM,etal.Modestactivityofpomalidomidein patientswithmyelofibrosisandsignificantanemia.LeukRes. 2013;37(11):1440–4.
44.BegnaKH,PardananiA,MesaR,LitzowMR,HoganWJ, HansonCA,etal.Long-termoutcomeofpomalidomide therapyinmyelofibrosis.AmJHematol.2012;87(1):66–8.
45.BegnaKH,MesaRA,PardananiA,HoganWJ,LitzowMR, McClureRF,etal.Aphase-2trialoflow-dosepomalidomide inmyelofibrosis.Leukemia.2011;25(2):301–4.
46.MesaRA,PardananiAD,HusseinK,WuW,SchwagerS,Litzow MR,etal.Phase1/-2studyofPomalidomideinmyelofibrosis. AmJHematol.2010;85(2):129–30.
47.TefferiA,VerstovsekS,BarosiG,PassamontiF,RobozGJ, GisslingerH,etal.Pomalidomideisactiveinthetreatmentof anemiaassociatedwithmyelofibrosis.JClinOncol.
2009;27(27):4563–9.
myeloproliferativeneoplasmsinfibroticphase.EurJ Haematol.2015.
49.MesaRA.HowItreatsymptomaticsplenomegalyinpatients withmyelofibrosis.Blood.2009;113(22):5394–400.
50.ElliottMA,TefferiA.Splenicirradiationinmyelofibrosiswith myeloidmetaplasia:areview.BloodRev.1999;13(3):163–70.
51.TefferiA,MesaRA,NagorneyDM,SchroederG,Silverstein MN.Splenectomyinmyelofibrosiswithmyeloidmetaplasia:a single-institutionexperiencewith223patients.Blood. 2000;95(7):2226–33.
52.SantosFP,TamCS,KantarjianH,CortesJ,ThomasD,Pollock R,etal.Splenectomyinpatientswithmyeloproliferative neoplasms:efficacy,complicationsandimpactonsurvival andtransformation.LeukLymphoma.2014;55(1):121–7.
53.KitanakaA,TakenakaK,ShideK,MiyamotoT,KondoT, OzawaK,etal.Splenicirradiationprovidestransient palliationforsymptomaticsplenomegalyassociatedwith primarymyelofibrosis:areporton14patients.IntJHematol. 2016.
54.MesaRA,SchwagerS,RadiaD,ChevilleA,HusseinK,Niblack J,etal.TheMyelofibrosisSymptomAssessmentForm (MFSAF):anevidence-basedbriefinventorytomeasure qualityoflifeandsymptomaticresponsetotreatmentin myelofibrosis.LeukRes.2009;33(9):1199–203.
55.PizziM,SilverRT,BarelA,OraziA.Recombinant interferon-alphainmyelofibrosisreducesbonemarrow fibrosis,improvesitsmorphologyandisassociatedwith clinicalresponse.ModPathol.2015;28(10):1315–23.
56.SilverRT,VandrisK,GoldmanJJ.Recombinant
interferon-alphamayretardprogressionofearlyprimary myelofibrosis:apreliminaryreport.Blood.
2011;117(24):6669–72.
57.SilverRT,KiladjianJJ,HasselbalchHC.Interferonandthe treatmentofpolycythemiavera,essentialthrombocythemia andmyelofibrosis.ExpertRevHematol.2013;6(1):49–58.
58.VerstovsekS,MesaRA,GotlibJ,LevyRS,GuptaV,DiPersioJF, etal.Adouble-blind,placebo-controlledtrialofruxolitinibfor myelofibrosis.NEnglJMed.2012;366(9):799–807.
59.MesaRA,VerstovsekS,GuptaV,MascarenhasJO,AtallahE, BurnT,etal.Effectsofruxolitinibtreatmentonmetabolicand nutritionalparametersinpatientswithmyelofibrosisfrom COMFORT-I.ClinLymphomaMyelomaLeuk.
2015;15(4):214–21.
60.VerstovsekS,MesaRA,GotlibJ,LevyRS,GuptaV,DiPersioJF, etal.Efficacy,safety,andsurvivalwithruxolitinibinpatients withmyelofibrosis:resultsofamedian3-yearfollow-upof COMFORT-I.Haematologica.2015;100(4):479–88.
61.Marti-CarvajalAJ,AnandV,SolaI.Januskinase-1andJanus kinase-2inhibitorsfortreatingmyelofibrosis.Cochrane DatabaseSystRev.2015;4:CD010298.
62.PatelKP,NewberryKJ,LuthraR,JabbourE,PierceS,CortesJ, etal.Correlationofmutationprofileandresponseinpatients withmyelofibrosistreatedwithruxolitinib.Blood.
2015;126(6):790–7.
63.BeauverdY,McLornanDP,HarrisonCN.Pacritinib:anew agentforthemanagementofmyelofibrosis?ExpertOpin Pharmacother.2015;16(15):2381–90.
64.JamiesonC,HasserjianR,GotlibJ,CortesJ,StoneR,TalpazM, etal.EffectoftreatmentwithaJAK2-selectiveinhibitor,
fedratinib,onbonemarrowfibrosisinpatientswith myelofibrosis.JTranslMed.2015;13:294.
65.KrogerNM,DeegJH,OlavarriaE,NiederwieserD,Bacigalupo A,BarbuiT,etal.Indicationandmanagementofallogeneic stemcelltransplantationinprimarymyelofibrosis:a consensusprocessbyanEBMT/ELNinternationalworking group.Leukemia.2015;29(11):2126–33.
66.MarkiewiczM,DzierzakMietlaM,WieczorkiewiczA,MiziaS, HelbigG,KoperaM,etal.Safetyandoutcomeofallogeneic stemcelltransplantationinmyelofibrosis.EurJHaematol. 2016;96(3):222–8.
67.LangeT,EdelmannA,SieboltsU,KrahlR,NehringC,JakelN, etal.JAK2p.V617Falleleburdeninmyeloproliferative neoplasmsonemonthafterallogeneicstemcell
transplantationsignificantlypredictsoutcomeandriskof relapse.Haematologica.2013;98(5):722–8.
68.RondelliD,BarosiG,BacigalupoA,PrchalJT,PopatU, AlessandrinoEP,etal.Allogeneichematopoieticstem-cell transplantationwithreduced-intensityconditioningin intermediate-orhigh-riskpatientswithmyelofibrosiswith myeloidmetaplasia.Blood.2005;105(10):4115–9.
69.CerquozziS,TefferiA.Blasttransformationandfibrotic progressioninpolycythemiaveraandessential
thrombocythemia:aliteraturereviewofincidenceandrisk factors.BloodCancerJ.2015;5:e366.
70.PassamontiF,RumiE,PungolinoE,MalabarbaL,BertazzoniP, ValentiniM,etal.Lifeexpectancyandprognosticfactorsfor survivalinpatientswithpolycythemiaveraandessential thrombocythemia.AmJMed.2004;117(10):
755–61.
71.WolanskyjAP,SchwagerSM,McClureRF,LarsonDR,TefferiA. Essentialthrombocythemiabeyondthefirstdecade:life expectancy,long-termcomplicationrates,andprognostic factors.MayoClinProc.2006;81(2):159–66.
72.BarbuiT,ThieleJ,PassamontiF,RumiE,BoveriE,RuggeriM, etal.Survivalanddiseaseprogressioninessential
thrombocythemiaaresignificantlyinfluencedbyaccurate morphologicdiagnosis:aninternationalstudy.JClinOncol. 2011;29(23):3179–84.
73.CervantesF.HowItreatmyelofibrosis.Blood. 2014;124(17):2635–42.
74.Vergara-LluriME,PiatekCI,PullarkatV,SiddiqiIN,O’Connell C,FeinsteinDI,etal.Autoimmunemyelofibrosis:anupdate onmorphologicfeaturesin29casesandreviewofthe literature.HumPathol.2014;45(11):2183–91.
75.BassRD,PullarkatV,FeinsteinDI,KaulA,WinbergCD,Brynes RK.Pathologyofautoimmunemyelofibrosis.Areportofthree casesandareviewoftheliterature.AmJClinPathol. 2001;116(2):211–6.
76.PullarkatV,BassRD,GongJZ,FeinsteinDI,BrynesRK.Primary autoimmunemyelofibrosis:definitionofadistinct
clinicopathologicsyndrome.AmJHematol.2003;72(1): 8–12.