r e v b r a s r e u m a t o l . 2017;57(5):475–478
w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Case
report
Devic’s
disease
in
an
adolescent
girl
with
juvenile
dermatomyositis
Neuromielite
óptica
em
uma
adolescente
com
dermatomiosite
juvenil
Melissa
Mariti
Fraga
a,
Enedina
Maria
Lobato
de
Oliveira
b,
Claudio
Arnaldo
Len
a,
Maria
Fernanda
Campos
b,
Maria
Teresa
Terreri
a,∗aUniversidadeFederaldeSãoPaulo,DepartamentodePediatria,UnidadedeReumatologiaPediátrica,SãoPaulo,SP,Brazil
bUniversidadeFederaldeSãoPaulo,DepartamentodeNeurologiaeNeurocirurgia,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received22April2014 Accepted1December2014 Availableonline9March2015
Introduction
Devic’sdisease,alsoknownasneuromyelitisoptica,is classi-fiedasanautoimmuneinflammatorydemyelinatingdisorder ofthe centralnervous system, distinct from multiple scle-rosis,that mainlyaffects theoptic nerve andspinal cord.1 Devic’sdiseasewasdemonstratedtobetheresultof antibod-iesagainstthewaterchannelaquaporin-4intheblood–brain barrier.2
Therehavebeen reportsofDevic’sdiseaseininfancy,3,4 but there are few reported associations of Devic’s dis-easewithotherdiseases.TheassociationofDevic’sdisease with dermatomyositis has not yet been described in the literature.
∗ Correspondingauthor.
E-mail:[email protected](M.T.Terreri).
Case
report
Afemale patientsought ourserviceat7years ofage, pre-sentingwithbipalpebraledemawithocularhyperemiaover theprevious4months.Shealsopresentededemaofthehands andfeet;paininthewrists,elbowsandknees;and muscu-larweakness.Shealsohad,onthatoccasion,anintermittent feverlasting15days.
The physical exam revealed heliotrope, Gottron’s sign, arthritisintheleftkneeandankle,andmuscularweakness intheupperandlowerlimbs(childhoodmyositisassessment scoreof14/52).5
Generalexamswereperformedwiththefollowingresults: hemoglobin of 10.4g/dl, 4400 leucocytes with a normal
http://dx.doi.org/10.1016/j.rbre.2014.12.004
2255-5021/©2015ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
476
rev bras reumatol.2017;57(5):475–478differential,erythrocytesedimentationrateof70mminthe firsthour,andanincreaseinmuscularenzymes (aspartate alaninetransferase712[normalvalue10upto35],creatine kinase187[normalvalue10upto155]andlactate dehydroge-nase1150[normalvalue240upto480]).
Assays for antinuclear antibodies, anti-DNA antibodies, anti-ENA(extractablenuclearantigens)antibodiesand anti-cardiolipin antibodies were negative, and the complement levelwasnormal.Amusclebiopsyshowedperifascicular atro-phytypicalofdermatomyositis.Thevideodeglutogramwas normal,andanailfoldcapillaroscopydemonstrateda sclero-dermapatternwithsignificantcapillarydeletionandectasia. Adiagnosisofjuveniledermatomyositiswasmade.6
Over two years, the patient received 11 pulse thera-pies of methylprednisolone, prednisone and methotrexate until clinical and laboratory control of the dermatomyosi-tis was achieved. The patient abandoned treatment for 4 years,thenshereturnedtothepediatricrheumatologyclinic four years ago, at age of 13, with no clinical (childhood myositis assessmentscore 41/52)5 nor laboratory evidence ofjuveniledermatomyositisactivityandnomedicationwas needed.
Two years ago,at age of15,the patient had numbness inthe left armwithout muscularweakness that lasted for 10daysandresolvedspontaneously.Aftertwomonths,the patientdevelopedparesthesiawithproximalanddistal mus-cularweaknessinallfourlimbs,anddifficultyinwalkingand carryingoutdailyactivities.Theneurologistorderedabrain computerizedtomographythatwasnormalandno medica-tionwasprescribed.Thepatientlostthefollowupagainand afterninemonthsoftheseinitialsymptoms,thepatienthad anepisodeofblurredvision anddistalweaknessinallfour limbs.
Theneurologicalexaminationrevealedhyperactivedeep tendonreflexesinrightupperlimbandlegs,without weak-ness,andaseverelossofvisionintherighteye(VA20/800) with fundus examination showingoptic disk atrophy. The expandeddisabilitystatusscale(EDSS)7 thatquantifies dis-ability in eight functional systems (pyramidal, cerebellar, brainstem,sensory,bowel andbladder,visual, cerebraland others)was4fromascaleof0to10.
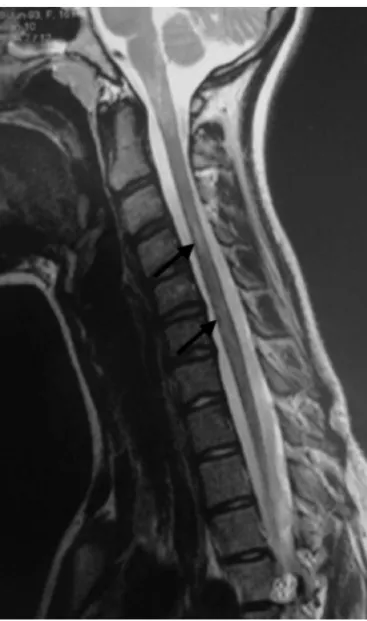
Laboratory tests including cerebrospinal fluid analysis showed noabnormalities.A neurologicalconsultation sug-gested central nervous system demyelination, and the neuraxismagneticresonanceimageshowedalongintraspinal lesionfromC3toT4(Figs.1and2).Aproposeddiagnosisof Devic’sdisease(neuromyelitisoptica)wasmade.Thepositive testforanti-aquaporin4antibodyconfirmedthe diagnosis. Thepatientwasstartedimmediatelyonpulsetherapywith methylprednisolonefollowedbyazathioprineplusprednisone asmaintenancetherapy.
Thepatientremainedstableforeightmonthswiththe ini-tialtherapeuticregimen.Ayear ago,thepatient presented a new outbreak of severe optic neuritis without muscu-larweakness butwithimpairedurinarysphincterfunction. Cerebrospinal fluid analysisand brain magneticresonance imaging were repeated. She was treated with intravenous immunoglobulin. Pulse therapy with methylprednisolone and the use ofprednisone 0.1mg/kg/day and azathioprine 3mg/kg/dayweremaintainedforfouryearsuptonow.After
Fig.1–Sagittalmagneticresonanceimage.T2-weighted cervicalspinalcordshowingalonghyperintensespinal cordlesion(blackarrow)inanadolescentgirlwithjuvenile dermatomyositis.
immunoglobulintreatment,thepatient’surinaryandvisual symptomsimproved.
Thepatienthasbeen inremissionforjuvenile dermato-myositisactivityforthelastfouryearsbutstillwithactivity oftheneuromyelitisoptica.
Discussion
Recurrent neuromyelitis optica is typically characterized by visual and spinal cord relapses. Clinical and labora-toryneuroimaging dataand theimmunopathology suggest that neuromyelitis optica differs from multiple sclerosis and presents a poorer prognosis, making early diagnosis of paramount importance for the initiation of aggressive immunosuppressivetherapy.8
rev bras reumatol.2017;57(5):475–478
477
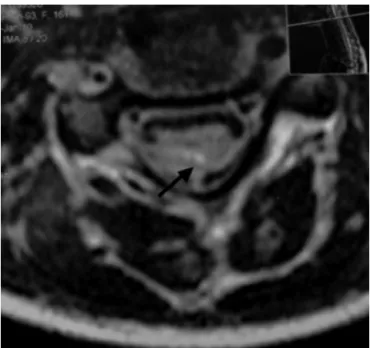
Fig.2–Axialmagneticresonanceimageofthecervical spine(C3)showingalonghyperintensespinalcordlesion (blackarrow)inanadolescentgirlwithjuvenile
dermatomyositis.
and at least 2 of the 3 following criteria: lesions in the spinalcord spanningat leastthree segments on magnetic resonanceimages,brainmagneticresonanceimages incom-patiblewithmultiplesclerosis andapositiveneuromyelitis opticaIgGtest(serummarker:auto-antibodydirectedagainst aquaporin-4).9
Anti-aquaporin4isanautoantibody(IgG)targetedagainst thewaterchannelsoftheblood–brainbarrier,andthe SNC lesion distribution corresponds to the areas where there is a high concentration of such channels. Therefore, anti-aquaporin-4maybeconsideredabiomarkerforneuromyelitis optica,althoughtheextentofthecorrelationbetweenthetiter oftheantibodyandtherelapseseverityisnotclear.9
Luccinetti et al. demonstrated the deposition of com-plement and perivascular IgM and the presence of an intenseinflammatoryinfiltratecomposedpredominantlyof macrophages,granulocytesandeosinophilsindemyelinating lesionsinneuromyelitisopticaautopsycases,confirmingthe importanceofhumoralimmunityinthepathophysiologyof neuromyelitisoptica.10
In a retrospective study covering a 15-year period, Jef-feryetal.evaluatedninechildrenwithneuromyelitisoptica. Allchildrenhadhadaviralinfectionpriortoneuromyelitis opticasymptoms.Bilateralopticneuritiswasacommon find-ing,observedin89%ofchildren,andallchildrenexhibiteda monophasiccourse.3However,antibody-positiveDevic’s dis-easeisnottypicallyassociatedwithamonophasicillnessbut doesdisplayaveryrapidprogressivecourse.
Ourpatientpresentedtheclinicalcharacteristicsdescribed above, magneticresonance imagingabnormalities and the presenceofantibodyanti-aquaporin-4.Shehastherecurrent formofthediseaseandalreadyhasirreversiblevisual impair-ment.
Neuromyelitisopticafindingsmayappearinpatientswith other autoimmune, inflammatory and infectious diseases with some reports in adults and children.11 Although the authorsdonotsuggestapossibleexplanationforthese associ-ations,infectiousagentscantriggertheautoimmuneprocess. There is no consensus on the treatment of recurrent neuromyelitisoptica.Severalalternativeshavebeenreported. Relapses are treated with oral prednisone, methylpred-nisolone,intravenousimmunoglobulinandplasmapheresis.12 Maintenance therapy involves monthly intravenous immunoglobulin13 and rituximab.14 Recently, two stud-iesshowedthattreatmentwithazathioprineplusprednisone ormofetilmycophenolatehaltsdiseaseprogression.12,15
Afterthefirstoutbreak,thispatientreceivedpulsetherapy withmethylprednisoloneandmaintenancewithprednisone and azathioprine. After the second outbreak, the use of methylprednisolonepulsetherapywithmonthlyintravenous immunoglobulin,inadditiontomaintainingprednisoneand azathioprine,waspreferred.
Conclusion
The onset of atypical neurological symptoms during the courseofarheumaticdiseaseshouldcallattentiontothe pos-sibilityofanassociationwiththisautoimmunedisease.Inthe casepresentedherein,theappearanceofunusualvisualand motorsymptomsinapatientwithjuveniledermatomyositis readilyledtoclinicalsuspicion,andlaboratorytestsconfirmed theassociatedneurologicaldisease.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.JacobA,MatielloM,WingerchukDM,LucchinettiCF,Pittock
SJ,WeinshenkerBG.Neuromyelitisoptica:changingconcepts.
JNeuroimmunol.2007;187:126–38.
2.Hino-FukuyoN,TakahashiT,HaginoyaK,UematsuM,
TsuchiyaS.ClinicalfeaturesofJapanesepediatricpatients
withanti-aquaporin4antibody.NoToHattatsu.
2011;43:359–65.
3.JefferyAR,BuncieJR.PediatricDevic’sneuromyelitisoptica.J
PediatrOphthalmolStrabismus.1996;33:223–9.
4.GokceG,CeylanOM,MutluFM,AltinsoyHI,KoyluT.
RelapsingDevic’sdiseaseinachild.JPediatrNeurosci.2013;8:
146–9.
5.LovellDJ,LindsleyCB,RennebohmRM,BallingerSH,Bowyer
SL,GianniniEH,etal.Developmentofvalidateddisease
activityanddamageindicesforthejuvenileidiopathic
inflammatorymyopathies.II.TheChildhoodMyositis
AssessmentScale(CMAS):aquantitativetoolforthe
evaluationofmusclefunction.TheJuvenileDermatomyositis
DiseaseActivityCollaborativeStudyGroup.ArthritisRheum.
1999;42:2213–9.
6.BohanA,PeterJB.Polymyositisanddematomyositis(two
478
rev bras reumatol.2017;57(5):475–4787. KurtzkeJF.Ratingneurologicimpairmentinmultiple
sclerosis:anexpandeddisabilitystatusscale(EDSS).
Neurology.1983;33:1444–52.
8. O’RiordanJI,GallagherHL,ThompsonAJ,HowardRS,
KingsleyDP,ThompsonEJ,etal.ClinicalandMRIfindingsin
Devic’sneuromyelitisoptica.JNeurolNeurosurgPsychiatry.
1996;60:382–7.
9. WingerchukDM,LennonVA,PittockSJ,LucchinettiCF,
WeinshenkerBG.Reviseddiagnosticcriteriaforneuromyelitis
optica.Neurology.2006;66:1485–9.
10.LuccinettiCF,MandlerRN,McGavernD.Aroleforhumoral
mechanismsinthepathogenesisofDevic’sneuromyelitis
optica.Brain.2002;125:1450–61.
11.BichuettiDB,OliveiraEML,SouzaNA,RiveroRL,GabbaiAA.
NeuromyelitisopticainBrazil:astudyonclinicaland
prognosticfactors.MultScler.2009;15:613–9.
12.BichuettiDB,OliveiraEML,OliveiraDM,AmorindeSouzaN,
GabbaiAA.Neuromyelitisopticatreatment.Analysisof36
patients.ArchNeurol.2010;67:1131–6.
13.BakkerJ,MetzL.Devic’sneuromyelitisopticatreatedwith
intravenousgammaglobulin(IVIG).CanJNeurolSci.
2004;31:265–7.
14.BeresSJ,GravesJ,WaubantE.Rituximabuseinpediatric
centraldemyelinatingdisease.PediatrNeurol.2014;51:
114–8.
15.FalciniF,TrepaniS,RicciL,SimonniniG,DeMartinoM.
SustainedimprovementofagirlaffectedwithDevic’sdisease
over2yearsofmycophenolatemofetiltreatment.