r e v b r a s r e u m a t o l . 2017;57(5):483–486
w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Case
report
Whipple’s
disease
manifested
as
difficult-to-diagnose
polyarthralgia:
a
case
report
and
literature
review
Doenc¸a
de
Whipple
manifestada
como
poliartralgia
de
difícil
diagnóstico:
relato
de
caso
e
revisão
da
literatura
Guilherme
Almeida
Rosa
da
Silva
∗,
José
Soares
Pires
Neto
UniversidadeFederaldoEstadodoRiodeJaneiro(UNIRIO),RiodeJaneiro,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30January2014 Accepted7December2014 Availableonline20July2015
Introduction
Whipple’sdiseaseisararesystemicdisease,describedin1907 byGeorgeWhippleatJohnsHopkinsHospital.1Yearslater,in
1961,wasshowntobecausedbythebacteriumTropheryma whipplei.2Thisisamandatoryintracellularorganism,which
inhabitsmainlythegastrointestinaltractand,duetothelack ofdataprovingitsbenefittothehost,canbeconsidered a parasite.3
InfectionbyTropherymawhippleimaybeasymptomaticor presentwithseveralclinicalmanifestationssuchasfever, pol-yarthralgia,diarrhea,weightloss,fatigue,lymphadenopathy, pulmonary, heart, and skin involvement, and neurolog-ical disorders, such as oculomasticatory myorhythmia, oculo-facio-skeletalmyorhythmia,dementiaandintracranial hypertension.4 Itisarare disease andthe clinicalfeatures
are extensive and varied,with absolutely variable order of appearanceofsymptoms,determininganextremelydifficult
∗ Correspondingauthor.
E-mail:[email protected](G.A.Silva).
diagnosis.Without properantibiotictreatment, the disease invariably culminates in dissemination and is potentially fatal.5
Whipple’sdiseasehasanincidencethatismuchlowerthan 1:1,000,000people,withandoccurrenceof12newcasesper yearworldwidebeingestimated.Ithasacorrelationwith cel-lularimmunitydeficienciesandHLADRB1*13,DQB1*06and HLAB27.6,7 Itaffectsmainlymiddle-agedmen,aroundfifty
years,witharatioof6:1comparedtowomen.8Complaints
ofmigratorypolyarthralgiausuallyprecedediarrheainmany years.9
Thisarticleaimstoreportacasemarkedbypolyarthralgia thathaddifficultetiologicaldefinitionanddelayeddiagnosis, the conclusionofwhichwasWhipple’s disease andreview therelatedliterature.Thepatientwhosecasewasreportedin thisstudyagreedwiththepublicationandtheResearchEthics CommitteeofHospitalGaffréeandGuinleapprovedthestudy undernumber631,797.
http://dx.doi.org/10.1016/j.rbre.2015.05.003
484
rev bras reumatol.2017;57(5):483–486Case
report
Male, brown, 45-year-old patient, who has been married for 26 years, Brazilian from the city of Simonésia, in the stateofMinasGerais,businessman,evangelicalChristian.He presentedin2006with severe episodicright hip arthralgia thatremittedwithanalgesics.In2007hepresentedadditive, episodicandsometimesmigratoryarthralgiathataffectedthe rightkneejoint,rightsacroiliacjoint,rightelbowarthritisand, somemonthslater,rightanklearthritis.Duringthisperiod, the patientwas seenbyseveral physicians,who could not establish adiagnosis and prescribed painkillers,parenteral andoralanti-inflammatorydrugs.
He started tohave nocturnal flares of generalized non-specific pain, with dysesthesia, requiring several visits to emergency rooms with use ofweak opioids between 2008 and2009.Duringthisperiod,theclinicalfeaturesofadditive, migratory,episodicpolyarthralgiaevolvedtogeneralized pol-yarthritis,alsoaffectingthesternoclavicularjoint.Thepatient mainpaincomplaints referredtohip and sacroiliac joints. He has taken analgesics, nonsteroidal anti-inflammatory drugs, oral corticosteroids and weak opioids with partial response.
Therheumatologistassistantchosetostarttherapywith abiologicalagentinfliximab.Aftertheseconddose,he pre-sentedafeverandmaculopapularrashinthedorsalregion and upperlimbs. Duetodissatisfaction withthe resultsof treatment,in2010hesoughtphysiciansofotherspecialties andalternativetherapiesforpainreliefwithoutsuccess.
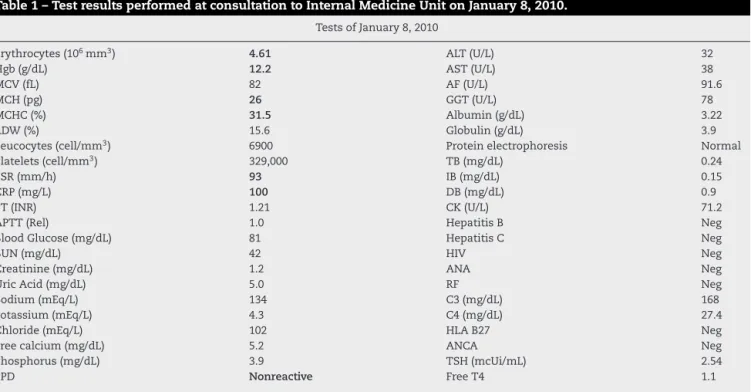
Giventheuncertaintyofthecase,helookedforthe Inter-nal Medicine Unit of the University Hospital Gaffrée and Guinle – UNIRIO. After history and physical examination, newcomplementarytestswererequested(Table1).Thefact that the patient had joint complaints, consulted multiple specialists,hadnegativecomplementarytestsforrheumatic diseases and presentedanon-reactive PPD,althoughliving in an endemic area of tuberculosis, was noted. This was interpretedasapossibledefectofcellimmunity.Withthis information,thediagnosishypothesiswasanarticular man-ifestationofasystemicdisease.SinceHLAB27wasnegative, the classic seronegative spondyloarthropathies(ankylosing spondylitis, inflammatory bowel disease, Reactive Arthri-tis, Psoriatic Arthritis) was less likely, but not impossible. Behc¸et’sdisease andWhipple’sdisease werecontemplated. Thepatientreceivedawrittensummaryoftheclinical fea-tures and an immediate request of upper gastrointestinal endoscopywithduodenalbiopsytospecificallyruleout Whip-ple’s disease. Despite this evaluation, the patient did not followtheindicationsandhedidnotreturn.
In 2011, together withthe articular features, he started a refractory very severe headache. Associated with the headache bursts, he developed a right hemiparesis and a leftfacialparalysisthatremittedspontaneously.Inaddition, hehadepisodesofdiarrheawithhematochezia,nauseaand vomiting,resultinginsignificantweightlossandmuscle atro-phy.
In2012,thediseaseprogressedandthepatientrequired hospitalization in the Intensive CareUnit (ICU) inthe city of Juiz de Fora, state ofMinas Gerais. He had intracranial
Table1–TestresultsperformedatconsultationtoInternalMedicineUnitonJanuary8,2010.
TestsofJanuary8,2010
Erythrocytes(106mm3) 4.61 ALT(U/L) 32
Hgb(g/dL) 12.2 AST(U/L) 38
MCV(fL) 82 AF(U/L) 91.6
MCH(pg) 26 GGT(U/L) 78
MCHC(%) 31.5 Albumin(g/dL) 3.22
RDW(%) 15.6 Globulin(g/dL) 3.9
Leucocytes(cell/mm3) 6900 Proteinelectrophoresis Normal
Platelets(cell/mm3) 329,000 TB(mg/dL) 0.24
ESR(mm/h) 93 IB(mg/dL) 0.15
CRP(mg/L) 100 DB(mg/dL) 0.9
PT(INR) 1.21 CK(U/L) 71.2
APTT(Rel) 1.0 HepatitisB Neg
BloodGlucose(mg/dL) 81 HepatitisC Neg
BUN(mg/dL) 42 HIV Neg
Creatinine(mg/dL) 1.2 ANA Neg
UricAcid(mg/dL) 5.0 RF Neg
Sodium(mEq/L) 134 C3(mg/dL) 168
Potassium(mEq/L) 4.3 C4(mg/dL) 27.4
Chloride(mEq/L) 102 HLAB27 Neg
Freecalcium(mg/dL) 5.2 ANCA Neg
Phosphorus(mg/dL) 3.9 TSH(mcUi/mL) 2.54
PPD Nonreactive FreeT4 1.1
rev bras reumatol.2017;57(5):483–486
485
Fig.1–Specimencollectedbyduodenalbiopsy.Periodic Acid–Schiff(PAS)staining.Markedaccumulationof
PAS-positivemacrophages(whitearrow)onsubmucosa
andpresenceoffibrosis(blackarrow)suggestingachronic process.
hypertension due to cerebral edema, confirmed by mag-neticresonance imaging(MRI) associatedwith dyspneaon minimalexertion, paroxysmal nocturnal dyspnea, prerenal failure, pleural effusion and generalized edemaconsistent withcongestiveheartfailure.Theechocardiographyshowed amitralvalvevegetationandinsufficiency.Themedicalteam who conductedthe case requested an upper gastrointesti-nalendoscopywithduodenal biopsy forWhipple’s disease investigation after reviewing information collected in the consultationattheInternalMedicineUnitin2011. Histopatho-logicalspecimenexaminationandpolymerasechainreaction (PCR)wereperformedatthePasteurInstituteinFrance(Fig.1), whichconfirmedTropherymawhipplei.Theprimer oligonu-cleotidesequenceusedwaspW3FE(5′-GGAATTCCAGAGATA
CCCGCCGCCCAA-3′)andpW2RB(5′-CGGGATCCCATTCGC
TCCACCTTGCGA-3′).10
In view of the diagnosis, therapy was initiated with trimethoprim-sulfamethoxazole, soon interrupted due to severe gastrointestinal intolerance. Therapy was replaced with doxycycline100mg orally 2 tablets bid and hydroxy-chloroquine600mgorally once a day. Thepatient showed dramaticclinicalimprovementandwasdischargedfor out-patientmonitoring.
Discussion
Whipple’s disease has a variable presentation of pol-yarthralgia, including symmetric and asymmetric formsof intermittentnature,sometimesbeingmigratoryoradditive. Joint involvementispresent in over 90% ofcasesand can precedetheexuberantmanifestationofthediseaseinabout adecade.11
Thepatientpresentedthepolyarticulararthritisfeatures aboutfiveyearsbeforethesevereillness.During theinitial period, he had consultations with multiple internists and
rheumatologistswithoutaspecificdiagnosis,alsoundergoing immunosuppressivetherapies(infliximab)thatworsenedthe disease.Thesearchforpainreliefwasaddedtothefrustration ofnotreceivinganaccuratediagnosis,includingseeking alter-nativetherapies.Whenhewasseenatourclinic,somedetails calledourattention.Thefirstwasthefactthatexperts,even orderinganextensivelistoftests,couldnotprovideaclear diagnosticdefinition,whatreinforcedthehypothesisthatthis wasajointdiseaseprobablyrelatedtoararesystemicdisease, possiblyindirectlyrelatedtorheumatology.
Other relevant information was the absence of symp-tomssuchaschronicdiarrhea(inflammatoryboweldisease), lesionssuggestiveofpsoriasisoranyotherskininvolvement (psoriasis, SAPHO or Behcet’s disease), no history of sexu-allytransmitteddiseases(ReactiveArthritis),featuresthatare non-excludingwhenconsideringthatthearticular manifes-tationmayprecedeothersymptoms.ThenegativeHLAB27 wasvaluedbecauseofitsknowncorrelationwithseronegative spondyloarthropathies.12
Finally, wehighlight the fact ofPPD not being reactive, something possible, but unusual in a resident of a highly endemictuberculosisregion.Thenon-reactivePPDleadusto thinkofcellularimmunitychanges,notlinkedtoAIDS,given thatHIVtestwasnegative.ThehypothesisofWhipple’s dis-easewassuggested,13–15butthepatientdidnotreturntothe
outpatient’sclinicwiththeuppergastrointestinalendoscopy andduodenalbiopsythathadbeenrequested.Abandonment wasattributedtothepatient’s lackoftrustintheabilityof medicinetosolvetheproblemofchronicpain.Thecasehas evolvedinto atypicalformofacomplex clinicalsyndrome relatedtoWhipple’sdisease.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.WhippleGH.Ahithertoundescribeddiseasecharacterized anatomicallybydepositsoffatandfattyacidsinthe intestinalandmesentericlymphatictissues.BullJohns HopkinsHosp.1907;18:382–91.
2.ChearsWC,AshworthCT.Electronmicroscopicstudyofthe intestinalmucosainWhipple’sdisease:demonstrationof encapsulatedbacilliformbodiesinthelesion.
Gastroenterology.1961;41:129–38.
3.WilsonKH.Whipplediseaseresearchaccelerates.JInfectDis. 2011;204:4–5.
4.DobbinsWOIII.Whipple’sdisease.MayoClinProc. 1988;63:623–4.
5.GuthikondaB,RouahE,KrishnanB,PowellSZ,GoodmanJC, GopinathSP,etal.Whipplediseaseofthecentralnervous system:anunusualoccurrenceinassociationwithacquired immunedeficiencysyndrome.JNeurosurg.2010;112:983–9.
6.MartinettiM,BiagiF,BadulliC,FeurleGE,MullerC,MoosV, etal.TheHLAallelesDRB1*13andDQB1*06areassociatedto Whipple’sdisease.Gastroenterology.2009;136:2289–94.
7.FeurleGE.AssociationofWhipple’sdiseasewithHLA-B27. Lancet.1985;325:1336.
486
rev bras reumatol.2017;57(5):483–486assessmentoftreatmentin29patients.MayoClinProc. 1988;63:539–51.
9. TanTQ,VogelH,TharpBR,CarrolCL,KaplanSL.Presumed centralnervoussystemWhipple’sdiseaseinachild:case report.ClinInfectDis.1995;20:883–9.
10.FenollarF,FournierP,RaoultD.Quantitativedetectionof TropherymawhippleiDNAbyreal-timePCR.JClinMicrobiol. 2002;40:1119–20.
11.DurandD,LecomteC,CathedrasP,RoussetH,GodeauP. Whipple’sdisease.ClinicalReviewof52cases.TheSNFMI ResearchGrouponWhipple’sdisease.SocieteNationale FrancaisedeMedecineInterne.MedTropherymaWhipplei. 1997;76:170–84.
12.McHughNJ.Otherseronegativespondyloarthropathies. Medicine.2010;78:190–3.
13.DobbinsWOIII.IsthereanimmunedeficitinWhipple disease?DigDisSci.1981;26:247–52.
14.KentSP,KirkpatrickPM.Whippledisease.Immunologicaland histochemicalstudiesofeightcases.ArchPatholLabMed. 1980;104:544–7.
15.GrollA,ValbergLS,SimonJB,EidingerD,WilsonB,Forsdyke DR.ImmunologicaldefectinWhipple’sdisease.