RELATI ONS BETW EEN NURSI NG DATA COLLECTI ON, DI AGNOSES AND PRESCRI PTI ONS
FOR ADULT PATI ENTS AT AN I NTENSI VE CARE UNI T
1Em ilia Cam pos de Car v alho2 Fer nanda Tit ar eli Mer izio Mar t ins3 Mar ia Célia Bar cellos Dalr i4 Silvia Rit a Marin da Silva Canini4 Ana Mar ia Laus4 Mar ia Mar cia Bachion5 Lidia Apar ecida Rossi6
Carvalho EC, Mart ins FTM, Dalri MCB, Canini SRMS, Laus AM, Bachion MM, Rossi LA. Relat ions bet ween nursing dat a collect ion, diagnoses and prescript ions for adult pat ient s at an int ensive care unit . Rev Lat ino- am Enferm agem 2008 j ulho- agost o; 16( 4) : 700- 6.
This descr ipt iv e, r et r ospect iv e st udy aim ed t o analy ze t he r elat ion bet w een nur sing dat a collect ion, diagnoses an d pr escr ipt ion s f or 2 6 adu lt pat ien t s w h o w er e h ospit alized at t h e in t en se car e u n it of a lar ge t each in g h osp it al f or at least 2 4 h ou r s. Th r ou g h t h e an aly sis of m ed ical r ecor d s, 1 3 5 d iag n oses an d 4 2 1 n u r sin g pr escr ipt ions w er e est ablished, and 24 differ ent diagnosis cat egor ies and 20 differ ent it em s for pr escr ipt ions w er e ident ified. The m ost fr equent diagnosis r isk w as t hat for infect ion, pr esent in t he m edical r ecor ds of 22 ( 84.60% ) pat ient s, w it h 175 pr escr ipt ions ( 42% ) r elat ed t o t his diagnosis. The dat a t he nur ses collect ed w er e sufficient to establish the nursing diagnoses, and the m ajority of prescriptions (87.9% ) were related to the diagnoses.
DESCRI PTORS: nur sing pr ocess; nur sing diagnosis; int ensiv e car e unit
RELACI ONES ENTRE LA RECOLECCI ÓN DE DATOS, DI AGNÓSTI COS Y PRESCRI PCI ONES
DE ENFERMERÍ A A PACI ENTES ADULTOS EN UNA UNI DAD DE TERAPI A I NTENSI VA
La finalidad de est e est udio descr ipt iv o y r et r ospect iv o fue analizar la r elación ent r e la r ecolección de dat os, diagnóst icos y pr escr ipciones de enfer m er ía par a 2 6 pacient es adult os que est uv ier on hospit alizados en una unidad de t erapia int ensiva en un hospit al de enseñanza de gran port e, con perm anencia m ínim a de 24 horas. Median t e el an álisis de los ar ch iv os se est ablecier on 1 3 5 diagn óst icos y 4 2 1 pr escr ipcion es de en f er m er ía, sien do iden t if icados 2 4 cat egor ías de diagn óst ico y 2 0 dif er en t es ít em s de pr escr ipción . El diagn óst ico de riesgo para la infección fue el m ás frecuent e, que est uvo present e en el regist ro de 22 ( 84,60% ) pacient es. De las p r escr ip cion es, 1 7 5 ( 4 2 % ) se r ef ir ier on a est e d iag n óst ico. Se ob ser v a q u e los d at os r eg ist r ad os p or los enfer m er os en la r ecolección de dat os fuer on suficient es par a est ablecer los diagnóst icos de enfer m er ía y que la m ay or ía de las pr escr ipciones ( 87, 9% ) est uv ier on r elacionadas con los diagnóst icos.
DESCRI PTORES: pr ocesos de enfer m er ía; diagnóst ico de enfer m er ía; unidades de t er apia int ensiv a
RELAÇÕES ENTRE A COLETA DE DADOS, DI AGNÓSTI COS E PRESCRI ÇÕES DE
ENFERMAGEM A PACI ENTES ADULTOS DE UMA UNI DADE DE TERAPI A I NTENSI VA
Trabalho descrit ivo, ret rospect ivo, que t eve com o obj et ivo analisar a relação ent re a colet a de dados, diagnóst icos e prescrições de enferm agem est abelecidas por enferm eiros para 26 pacient es adult os que est iveram int ernados num a unidade de t erapia int ensiva de um hospit al de ensino de grande port e, com perm anência m ínim a de 24 h or as. Por m eio d a an álise d os p r on t u ár ios, f or am est ab elecid os 1 3 5 d iag n óst icos e 4 2 1 p r escr ições d e enfer m agem , sendo ident ificadas 24 difer ent es cat egor ias diagnóst icas e 20 difer ent es it ens par a pr escr ição. O diagnóst ico de risco para infecção foi o de m aior freqüência, present e no pront uário de 22 ( 84,60% ) pacient es. Das pr escr ições, 1 7 5 ( 4 2 % ) r elacionar am - se a esse diagnóst ico. Obser v a- se que os dados r egist r ados pelos enfer m eir os na colet a de dados for am suficient es par a o est abelecim ent o dos diagnóst icos de enfer m agem e a m aior ia das pr escr ições ( 87, 9% ) apr esent ou r elação com os diagnóst icos.
DESCRI TORES: pr ocessos de enfer m agem ; diagnóst ico de enfer m agem ; unidades de t er apia int ensiv a
1 Proj ect developed at t he Nursing Com m unicat ion Laborat ory, Universit y of Sao Paulo at Ribeirao Pret o College of Nursing, WHO Collaborat ing Cent re for
Nursing Research Developm ent , Brazil, and funded by CNPq; 2 RN, Full Professor, e- m ail: [email protected]; 3 RN, e- m ail: t it [email protected]; 4 RN, Facult y, e- m ail: m acdalr i@eer p. usp. br, canini@eer p. usp. br, analaus@eer p.usp.br. Univer sit y of Sao Paulo at Ribeirao Pr et o College of Nur sing, WHO Collaborat ing Cent er for Nur sing Resear ch Dev elopm ent , Brazil; 5 RN, Fu ll Pr ofessor, Sch ool of Nu r sin g, Goiás Federal Univ er sit y, Brazil, e- m ail: m [email protected]; 6 RN, Associat e Professor, Universit y of Sao Paulo at Ribeirao Pret o College of Nursing, WHO Collaborat ing Cent er for Nursing Research Developm ent , Brazil, e- m ail: [email protected].
I NTRODUCTI ON
N
ur sing pr act ice, suppor t ed by an int uit iv e b asis, h as b een st r u ct u r in g it self t h r ou g h scien t if icpr inciples, using m odels and t heor et ical appr oaches.
I t i s ch a r a ct e r i ze d b y sy st e m a t i ca l l y d e l i b e r a t e d
act iv it ies, logics and r at ionales, t hus suppor t ing t he
ev aluat ion of client s’ healt h condit ion.
Th e n u r s i n g p r o c e s s , a s a h e a l t h c a r e
m et h o d o l o g y, p r ov i d es t h e st r u ct u r e r eq u i r ed f o r
n u r s i n g c a r e . Th i s m e t h o d o l o g y c o m p r i s e s f i v e
i n t er r el a t ed co m p o n en t s: d a t a co l l ect i o n , n u r si n g
diagnosis, planning, im plem entation, and evaluation( 1- 2). Sev er al r ev iew st u d ies h av e look ed at t h e
effect s of t his m et hodology on clinical pract ice, m ainly
u s i n g t h e c l a s s i f i c a t i o n s f o r d i a g n o s e s( 3 ), int er v ent ion( 4 ), and r esult s( 5 ). Am ong ot her findings, t h ese st u dies h av e sh ow ed t h at dat a collect ion an d
r e a ch i n g a d i a g n o si s a r e f a ct o r s t h a t p o si t i v e l y
cont r ibut e t o nur sing docum ent at ion( 6).
The developm ent of each st age in t he nursing
p r ocess is d ir ect ly r elat ed w it h t h e n u r sin g t eam ’s
c o m p e t e n c e , s e r v i c e p h i l o s o p h y a n d r e s o u r c e s
available. St udies have shown t hat nurses’ cont inuing
educat ion on t his m et hodology significant ly im pr ov es
t he use of it s st ages. However, t he accuracy of nursing
d iag n oses d os n ot alw ay s m eet t h e q u alit y cr it er ia
for t he defining charact erist ics, and even less for t he
a s s o c i a t e d f a c t o r s . I t i s a l s o r e c o m m e n d e d t o
est ablish diagnoses, int ervent ions and result s t oget her
rat her t han separat ely( 6). The set of nursing diagnoses for one pat ient ( or a cer t ain client ele) ev idences t he
com plexit y of t he clinical condit ion and, consequent ly,
t he t ype of int ervent ions required t o solve t hose issues,
as w ell as t he r espect iv e gr oup of act iv it ies needed,
all of w hich ar e expr essed in nur sing pr escr ipt ions( 7). The num ber and t ype of nursing int ervent ions
t h e p a t i e n t r e ce i v e s h a s b e e n co n si d e r e d a ca r e
indicat or( 8- 10). Nev er t heless, t he effect t he diagnosis an d in t er v en t ion s h av e on p at ien t r esu lt s h as n ot
shown sat isfact ory evidence; on t he ot her hand, t here
has been an incr ease in t he quant it y and qualit y of
m edical r ecor ds( 11- 13).
I n addit ion , t h is for m of or gan izin g n u r sin g
w or k is con sider ed an im por t an t car e m an agem en t
t ool( 14) and allow s for providing pat ient s w it h t ailored qu alit y car e( 1 5 ). To r each all t h ese possibilit ies, t h e st ages of t his work inst rum ent should be appropriat ely
r eco r d ed .
I n t his sense, t he analysis of nursing not es in
m edical r ecor ds can cont r ibut e t o ident ify t he needs
a n d r e s u l t s o f p e r m a n e n t h e a l t h e d u c a t i o n
processes( 16- 17), help t o ident ify nursing’s part icipat ion in t he healt h result s pat ient s achieve( 6), as well as t o generat e dat a for sect or m anagers and t he inst it ut ion
adm in ist rat or.
A review of Brazilian nursing lit erat ure showed
t here are no st udies t hat look at t he effect s of m edical
r e c o r d q u a l i t y a n d t h e u s e o f d i a g n o s i s a n d
int er vent ion t axonom ies on pat ient r esult s. Sim ilar ly,
t h e r e a r e n o a n a l y se s o n t h e p e r t i n e n ce o f t h e
collect ed dat a for t he est ablished diagnoses, or about
t he correspondence of t hese dat a wit h t he associat ed
f a c t o r s o r d e f i n i n g c h a r a c t e r i s t i c s , a n d t h e
iden t if icat ion of t h ese elem en t s as det er m in an t s of
t h e pr escr ipt ion s.
These aspect s were obj ect s of int erest in t he
p r esen t st u d y. I n t h is sen se, t h e g en er al ob j ect iv e
w as t o analyze t he relat ions bet w een dat a collect ion,
est ablishing diagnoses and nur sing pr escr ipt ions for
adult s hospit alized in an int ensiv e car e unit .
Th e f o l l o w i n g s p e c i f i c o b j e c t i v e s w e r e
est ab lish ed :
- t o analyze nursing records focused on t he indent ified
diagn osis pr ofile;
- t o analyze t he relat ion bet ween nursing prescript ions
a n d t h e co n st r u ct i v e e l e m e n t s o f t h e i d e n t i f i e d
d iag n oses;
- t o analy ze t he m ost com m on nur sing diagnosis in
t er m s of it s sust ainabilit y in pat ient assessm ent dat a
an d p er t in en ce of t h e est ab lish ed p r escr ip t ion s f or
t hat pat ient .
MATERI AL AND METHODS
Th i s d e scr i p t i v e , r e t r o sp e ct i v e st u d y w a s
based on in for m at ion abou t n u r sin g dat a collect ion ,
diagnoses and pr escr ipt ions r ecor ded in t he m edical
r ecor ds of an I n t en siv e Car e Un it ( I CU) at a lar
ge-scale t eaching hospit al locat ed in t he int er ior of São
Paulo St at e. This st udy was approved by t he Research
Et hics Com m it t ee of t he st udy inst it ut ion.
The m edical records of pat ient s aged 18 year
or older w er e analy zed, m en and w om en, w ho w er e
hospit alized for at least 24 hours at t he I CU bet ween
August and Novem ber 2004. This set t ing was select ed
w h er e t h e n u r sin g pr ocess w as im plem en t ed at t h e
place of st udy. I n t he st udy per iod, 65 pat ient s m et
t h e in clu sion cr it er ia. Th e sam p le con sist ed of 2 6
( 4 0 % ) m ed ical r ecor d s t h at w er e av ailab le at t h e
Medical and St at ist ical File Ser vice of t he inst it ut ion.
The m edical r ecor d cont ained a st andar dized
inst rum ent , specifically designed for use by t he nursing
t eam . Th e in st r u m en t con sist ed of f ou r par t s: dat a
collect ion cat egorized by basic hum an necessit ies, list
of nursing diagnoses, nursing prescript ion, and nursing
evolut ion sheet ( which corresponds t o t he evaluat ion) .
D a t a r eg a r d i n g a d m i ssi o n , a s w el l a s t h e
r ecor ds cont aining t he diagnoses for each client and
t he proposed prescript ions w ere t ranscribed from t he
sheet used at t he inst it ut ion t o a form sim ilar t o t hat
used by t he nursing t eam . One inst rum ent w as used
t o r eco r d t h e d at a co l l ect i o n an d an o t h er f o r t h e
d i a g n o s e s a n d n u r s i n g p r e s c r i p t i o n . A n u r s e
ex per ien ced in n u r sin g pr ocess pr act ice an d t h eor y
p e r f o r m e d d a t a c o l l e c t i o n . Th e p a t i e n t s a n d
professionals involved in t he st udy were assured t hat
t heir ident it y w ould be pr eser v ed.
The dat a collect ed fr om t he m edical r ecor ds
w e r e a n a l y z e d b y f i v e r e s e a r c h e r s , w h o w e r e
specialist s in t h e t h em e. I n each case, t h e r ecor ds
were exam ined wit h a view t o ident ifying t he accuracy
o f t h e g i v e n n u r si n g d i a g n o se s, a s p r o p o se d i n
lit erat ure( 18). As t o t he r ecor ds r egar ding t he nur sing diagnoses, it was observed t hat t heir com ponent s were
p r e s e n t ( t i t l e / d i a g n o s i s c h a r a c t e r i s t i c , d e f i n i n g
char act er ist ics, and r elat ed fact or s/ r isk fact or s) and
p e r t i n e n t f o r t h e c o l l e c t e d d a t a . Th e n u r s i n g
p r escr ip t ion s w er e an aly zed w it h a f ocu s on t h eir
relat ion wit h t he com ponent s described in each of t he
est ablished nur sing diagnoses. The aut hor s analy zed
each prescript ion and ident ified if it result ed from t he
d iag n osis cat eg or y, t h e r elat ed f act or s or d ef in in g
charact erist ics for t he real diagnoses or t he diagnosis
cat egor y or r isk fact or s for t he r isk diagnoses.
Aft er assessing each pat ient record, a deeper
analysis was carried out ; for exam ple, of t he diagnosis
r isk for infect ion, since it occur r ed m or e oft en.
RESULTS AND DI SCUSSI ONS
St udies t hat look ed at m edical r ecor ds show
t h a t n u r s i n g d i a g n o s e s a n d i n t e r v e n t i o n s v a r y
depending on t he purpose of t he healt h care delivered
t o t h e p a t i en t a d m i t t ed t o t h e h ea l t h ser v i ce( 1 9 ). Sim ilar ly, t he num ber of diagnoses is also associat ed
w it h t he specific char act er ist ics of pat ient s fr om t he
different sect ors( 6). The int ensive care unit set t ing and t he pur pose of t his healt h car e ser v ice cont r ibut e t o
t h e p r of i l e of t h e d i ag n oses an d p r escr i p t i on s, as
described below. I t is observed t hat t he diagnosis t it les
a r e p r e s e n t e d a c c o r d i n g t o t h e i n s t r u c t i o n s b y
Car penit o, a r efer ence adopt ed by t he nur ses in t he
st udied sect or( 2).
Fo r t h e 2 6 s a m p l e p a t i e n t s , t h e n u r s e s
at t ribut ed 24 different diagnosis cat egories ( diagnosis
t it les) , 15 of which are real diagnoses ( 62.5% ) and 9
ar e r isk diagnoses ( 37.5% ) ( Table 1) .
Th e s e d i a g n o s e s b e l o n g t o t h e d o m a i n s
n u t r it ion ( 2 ) , elim in at ion ( 2 ) , act iv it y / r est ( 6 ) , an d
s a f e t y / p r o t e c t i o n ( 1 0 ) p r o p o s e d b y t h e N o r t h
Am er ican Nur sing Diagnosis Associat ion( 3). Ther e ar e f ou r ot h er dom ain s specif ic t o cr it ical pat ien t s an d,
t hough not included in t his t axonom y, t hey are relat ed
w it h t he dom ains safet y / pr ot ect ion ( 1 ) , act iv it y / r est
( 2) and com fort ( 1) . The ot her nine dom ains and t heir
r espect iv e classes( 3) ar e not look ed at in t he nur ses’ clinical j udgm ent , but include feasible diagnoses for
t h e su b j ect s o b ser v ed . I n t h e st u d y l o cat i o n , t h e
p r of ession als m ain ly f ocu s on t h e m ost im m ed iat e
aspect s of healt h car e.
Each pat ient received four t o nine diagnoses,
which corresponded t o an average of five real or risk
diagnoses per pat ient , t ot aling 135 diagnoses for t his
client ele; 57 ( 42% ) real and 78 ( 58% ) risk diagnoses.
The m ost com m on diagnoses w er e: r isk for
infect ion ( 84.6% ) ; im paired physical m obilit y ( 69.2% ) ;
r i sk f o r a sp i r a t i o n ( 6 5 . 3 % ) ; a n d r i sk f o r i n j u r y
( 6 1 . 5 % ) . Th e f ollow in g eig h t d iag n oses r an g ed in
fr equency bet w een 38.4% and 15.3% . The ot her 14
cat egor ies occur r ed in 7.6% or less of cases.
A st udy per for m ed w it h pat ient s in int ensive
car e unit s( 20) show ed t he follow ing nur sing diagnoses as t h e m ost fr equ en t : pain , r isk for in j u r y, an x iet y,
d e cr e a se d ca r d i a c o u t p u t , r i sk f o r i n f e ct i o n a n d
k n ow ledge deficit .
I n t h e pr esen t st u dy, som e diagn oses w er e
o b se r v e d i n m o st m e d i ca l r e co r d s, su g g e st i n g a
ch ar act er ist ic p r of ile f or t h e I CU p op u lat ion , w h ile
ot h er s ar e sp ecif ic f or each in d iv id u al. Th is asp ect
suggest s t hat , ev en in a cont ex t of w or k ing w it hin a
s p e c i a l t y, t h e n u r s e s d o n o t l o s e t r a c k o f t h e
Tab le 1 – Dist r ib u t ion of t h e Diag n osis Cat eg or ies
a c c o r d i n g t o n u r s i n g n o t e s i n m e d i c a l r e c o r d s
exam ined at a t eaching hospit al in t he int erior of São
Paulo St at e, 2004
While exam ining t he elem ent s const it ut ing t he
diagnoses, it is observed t hat t he 135 diagnoses ( real
and of r isk ) pr esent ed a diagnosis cat egor y ( 100% )
founded on t he t ax onom y adopt ed by t he ser v ice( 2); h ow ev er, t h ey w er e in com p let ely f or m u lat ed , sin ce
t he relat ed or risk fact ors were present in 133 ( 98.5% )
and 39 ( 28. 8% ) st at ed t heir defining char act er ist ics
i n co m p l et el y ; f o r a b o u t 1 4 % o f t h e su b j ect s, n o
d ef in in g ch ar act er ist ic w as con sid er ed ; it is w or t h
r em em b er in g t h at 4 2 % of t h e ob ser v ed d iag n oses
w er e r eal , i . e., t h ey sh o u l d al so p r esen t d ef i n i n g
ch ar act er ist ics. Th ese dat a su ggest t h at n u r ses ar e
n o t v a l u i n g , i n t h e i r n o t e s c o n c e r n i n g n u r s i n g
d i a g n o s e s , t h e c l i n i c a l e v i d e n c e s ( d e f i n i n g
charact erist ics) t hat pat ient s show. I n t his sense, it is
unknown if professionals do or do not include cert ain
ev idences in t heir clinical j udgm ent pr ocess, t hough
t h e d a t a w a s a v a i l a b l e i n t h e p a t i e n t s ’ h e a l t h
assessm en t r ecor d .
The accuracy in reaching a diagnosis has been
r epor t ed as a r elev ant difficult y( 6, 18); and has v ar ied con sid er ab ly( 2 1 ). A st u d y r ep or t ed t h at 3 0 % of t h e analy zed nur sing diagnoses pr esent ed poor accuracy,
accor ding t o t he specialist s’ ev aluat ion( 22).
I n t h e pr esen t st u dy, r isk f or in f ect ion w as
ch o sen f o r t h e a n a l y si s b eca u se i t w a s t h e m o st
fr equent diagnosis in t his st udy. The dat a, collect ed
an d r ecor ded by t h e n u r ses, sh ow ed t h at 1 0 0 % of
p at ien t s p r esen t ed r elev an t , sp ecif ic, an d coh er en t
clu es r egar din g t h e diagn osis. How ev er, t h e n u r ses
w er e u n able t o r each a diagn osis f or f ou r pat ien t s.
Hence, it is underst ood t hat accuracy was not reached
f or 1 5 . 3 % of su bj ect s. Th is r at e is low er t h an t h at
observed in lit erat ure, t hough it was considered for a
sin g le d iag n osis. On t h e ot h er h an d , it sh ou ld b e
highlight ed t hat , in bot h sit uat ions, t he nurses st at ed
t h e r eal d i ag n osi s cat eg or y as al t er ed p r o t ect i o n,
inst ead of r isk for infect ion.
Nu r ses’ j u dgm en t an d decision - m ak in g in a
c e r t a i n s i t u a t i o n c a n r e f l e c t , b e s i d e s s p e c i f i c
knowledge in t heir work field, knowledge of t he choices
and lim it at ions inherent t o t he diagnosis classificat ions.
Th e p r o f e s s i o n a l ’ s t e c h n i c a l a n d i n t e r p e r s o n a l
r elat ionship skills w hen r eaching a diagnosis, besides
t heir cr it ical t hink ing and k now ledge, as w ell as t he
cont ext of t he sit uat ion affect t he nurse’s int erpret at ion
of t h e dat a, w h ich , in t u r n , af f ect s t h e accu r acy of
t heir diagnoses( 22- 23).
Fur t her st udies should look at t he r at ionale
o f t h e p r o f e s s i o n a l ’ s d i a g n o s i s , w h i c h s h o w s a
t endency t o select m or e specific r at her t han br oader
d iag n oses.
B y o b s e r v i n g a l l m e d i c a l r e c o r d s , 4 2 1
p r escr i p t i o n s co u l d b e i d en t i f i ed f o r t h e o b t a i n ed
n u r sin g diagn oses, r an gin g bet w een 1 1 an d 2 2 per
pat ient , wit h an average of 16 prescript ions per pat ient .
I t is w or t h highlight ing t hat t he pr escr ibed act iv it ies
ar e dir ect ed by t he r esult expect ed for t he pat ient .
K n o w l e d g e a b o u t n u r s i n g i n t e r v e n t i o n s
r egar din g a cer t ain pat ien t gr ou p can iden t if y bot h
k n ow led g e g ap s in t h e ob ser v ed p r act ice an d n ew
p r ob lem - solv in g ap p r oach es of a d iag n osis. I n t h is
sense, t he Nursing I nt ervent ion Classificat ion( 4) as well as t he t axonom y adopt ed in t he sect or( 2) have helped t o dissem inat e int ervent ions and act ivit ies/ act ions for
nur sing diagnoses and for t he nur ses’ decisions.
A pr ev iously m ent ioned st udy, w it h pat ient s
fr om an I CU, r epor t ed t hat t he m ost used act iv it ies/
act ions were direct ed t o int ervent ions t o m onit or vit al
par am et er s, pr ov ide em ot ional suppor t , t eaching and
coor dinat ion( 20).
Th e p r e s c r i p t i o n s ’ s p e c i f i c i t y, i . e . , h o w
appropriat e t hey are for t he com ponent s of a part icular
d iag n osis, w as also an aly zed ( ob j ect iv e 2 ) . Am on g
s e s o n g a i
D N %
n o it c e f n i r o f k s i
R 22 84.6
y t il i b o m l a c i s y h p d e r i a p m
I 18 69.2
n o it a r i p s a r o f k s i
R 17 65.3
y r u j n i r o f k s i
R 16 61.5
. y t i r g e t n i n i k s d e r i a p m i r o f k s i
R 10 38.4
n r e t t a p g n i h t a e r b e v it c e f f e n
I 09 34.6
y t i r g e t n i n i k s d e r i a p m
I 08 30.7
n o it a li t n e v s u o e n a t n o p s n i a t s u s o t y t il i b a n
I 05 19.2
y t i r g e t n i e u s s it d e r i a p m
I 04 15.3
n o i s u f r e p e u s s it l a r e h p i r e p d e r e tl
A 04 15.4
e c n a r a e l c y a w r i a e v it c e f f e n
I 03 11.5
n o i s s i m s n a r t n o it c e f n i r o f k s i
R 02 7.6
e g n a h c x e s a g d e r i a p m
I 02 7.6
n o it c e t o r p d e r e tl
A 02 7.6
s t n e m e r i u q e r y d o b n a h t s s e l , n o it i r t u n d e r e tl
A 02 7.6
e s n o p s e r g n i n a e w y r o t a li t n e v l a n o it c n u f s y
D 01 3.8
n o it a li t n e v s u o e n a t n o p s n i a t s u s o t y t il i b a n i r o f k s i
R 01 3.8
n o i s u f r e p e u s s it c a i d r a c d e r e tl
A 01 3.8
n o it c n u f s y d r a l u c s a v o r u e n l a r e h p i r e p r o f k s i
R 01 3.8
n o i s u f r e p e u s s it l a r b e r e c d e r e tl
A 01 3.8
s s e c x e e m u l o v d i u l
F 01 3.8
n o it a n i m il e y r a n i r u d e r e tl
A 01 3.8
t r o f m o c d e r e tl
A 01 3.8
e r u t a r e p m e t y d o b d e r e tl a r o f k s i
t h e 3 7 9 p r e scr i p t i o n s p e r t i n e n t t o t h e r e co r d e d
diagn oses, 3 2 . 4 % w er e r elat ed w it h t h e diagn ost ic
cat egor ies, 9 0 % t o t h e r elat ed or r isk f act or s, an d
1 9 . 5 % t o t h e d e f i n i n g c h a r a c t e r i s t i c s . Mo s t
p r escr ip t ion s ( 8 7 . 9 % ) h av e som e r elat ion w it h t h e
d iag n oses r each ed , b u t 5 2 ( 1 2 . 1 % ) d id n ot , w h ich
ev idences t he use of pr escr ipt ions r egar dless of t he
pat ient s’ r ecor ded condit ion.
This is perhaps due t o t he fact t hat , in order
t o pr escr ibe n u r sin g act ion s, t h e pr ofession al m igh t
hav e consider ed t he m edical diagnosis as t he focus;
in t h is sen se, t h e st u dy sh ow s t h at n u r ses iden t if y
m ore issues relat ed t o t he m edical t han t o t he nursing
diagnosis( 24). I t m ay also be relat ed wit h difficult ies t o ident ify, in t he adopt ed t axonom y, t he hum an response
t o t h e sit u at ion , despit e clar it y abou t w h at act iv it y
w ou ld b e n ecessar y. Th e lit er at u r e sh ow s t h at , in
ce r t a i n si t u a t i o n s, r e a ch i n g a n u r si n g d i a g n o si s
b e c o m e s u n f e a s i b l e o r t h a t p r o b l e m s g o b y
unident ified. I n t hese cases, per m anent educat ion of
t he nursing st aff can cont ribut e t o an appropriat e use
o f n u r s i n g d i a g n o s e s a n d c o r r e s p o n d i n g
int er v ent ions( 24).
Risk f or I n f ect ion : r elat ion w it h pat ien t assessm en t
dat a and per t inence for t he pr escr ipt ions
An al y zi n g t h e m ost f r eq u en t d i ag n osi s, i n
t er m s of it s sust ainabilit y in pat ient assessm ent dat a
and per t inence for t he pr escr ipt ions ( obj ect iv e 3) , it
w a s co n si d e r e d i m p o r t a n t t o cl a r i f y t h a t r i sk f o r
in f ect ion is con sid er ed( 2 ) “a con d it ion in w h ich t h e individual is at risk of being invaded by an opport unist
or pat hogenic agent ( virus, fungus, bact eria, prot ozoa,
or any ot her parasit e) from endogenous or exogenous
sou r ces”. Th is d iag n osis is g r ou p ed in t h e NANDA
Taxonom y I I in Dom ain 11( 3), which addresses Safet y / Pr ot ect ion , w h ich m ean s “ b ein g f r ee f r om d an g er,
physical inj uries, or harm s t o t he im m unologic syst em ;
pr escr ipt ion against losses; and pr ot ect ion of safet y
and securit y” and in Class 1 infect ion “ w hich are t he
host ’s r esponses aft er t he pat hogenic inv asion”.
Th e con cept of a diagn osis, it s dom ain an d
cl ass ar e t h e m ai n el em en t t o ef f ect i v el y st at e a
p r ob lem id en t if ied b y t h e n u r se. I n t h is case, t h e
d i ag n o si s w as co n st r u ct ed b ased o n t h e p at i en t ’s
v u ln er abilit y t o ex posu r e.
Th e pr esen ce of t h is diagn osis in 8 4 . 6 % of
t h e m ed i cal r eco r d s sh o w s t h at t h e p r o f essi o n al s
c o n s i d e r t h e r i s k f a c t o r s p r e s e n t i n t h e I CU
hospit alizat ion cont ex t , in w hich pat ient s ar e usually
subm it t ed t o at least one inv asiv e pr ocedur e. Since
nur ses, aft er r eaching a diagnosis and it s elem ent s,
obt ain t he m eans t o select t he int ervent ions t hey will
prescribe, it is expect ed t hat , based on t hat diagnosis,
t he necessary prot ect ion m easures are prescribed and
im p lem en t ed .
When exam ining t he elem ent s const it ut ing t he
diagnosis r isk for infect ion, it w as obser v ed t hat , in
t he 22 m edical r ecor ds, at least one r isk fact or w as
ident ified ( Table 2) .
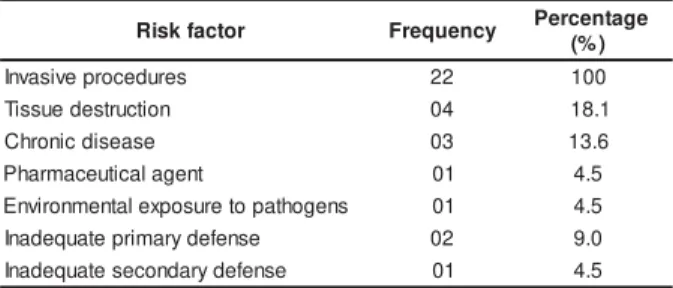
Table 2 – Dist ribut ion of risk fact ors for t he diagnosis
r isk for infect ion at t r ibut ed in t he obser v ed m edical
r ecor ds ( n= 22) at a t eaching hospit al in t he int er ior
of São Paulo St at e, 2004
r o t c a f k s i
R Frequency Percentage
) % (
s e r u d e c o r p e v i s a v n
I 22 100
n o it c u r t s e d e u s s i
T 04 18.1
e s a e s i d c i n o r h
C 03 13.6
t n e g a l a c it u e c a m r a h
P 01 4.5
s n e g o h t a p o t e r u s o p x e l a t n e m n o r i v n
E 01 4.5
e s n e f e d y r a m i r p e t a u q e d a n
I 02 9.0
e s n e f e d y r a d n o c e s e t a u q e d a n
I 01 4.5
The difficult y t o st op basing nursing diagnosis
on et iologic fact ors has been report ed in lit erat ure( 25).
I n t he pr esent st udy, t her e w er e r ecor ds r efer r ing t o
seven different risk fact ors. All records report t he risk
f a ct o r i n v a si v e p r o ced u r es. I n so m e r eco r d s, t h e
m e a n s o f i n v a si o n a r e n o t sp e ci f i e d w h e r e a s, i n
ot h er s, t h ey w er e st at ed as, f or in st an ce, v en ou s
punct ur es, cat het er s, v ent ilat ion sy st em and ot her s.
Th e s e d a t a r e i n f o r c e t h e e x i s t e n c e o f a
b eh av ior p at t er n am on g n u r ses r eg ar d in g t h e w ay
t hey reach t his diagnosis for t he st udied client ele, and
in t erm s of t he risk fact ors and t erm s adopt ed, which
allows for t he charact erizat ion of one of t he pat ient s’
m ar k in g f eat u r es.
Re g a r d i n g t h e p r e s c r i p t i o n s , s o m e w e r e
dir ect ed t o t h e diagn osis t it le ( diagn osis cat egor y ) ,
w hile ot hers t o t he risk fact ors.
For t h at d iag n osis, 1 7 5 p r escr ip t ion s w er e
est ablished, r anging fr om six t o 11, w it h an aver age
e i g h t p r e scr i p t i o n s p e r p a t i e n t . Tw e n t y d i f f e r e n t
pr escr ipt ion it em s w er e obser v ed, m ain ly r egar din g
b o d y h y g i e n e , o r a l h y g i e n e , p e r s o n a l h y g i e n e ,
d r e ssi n g s, cl e a n i n g t h e u r i n e b a g , a n d ch a n g i n g
I t is not iced t hat appr ox im at ely 42% of t he
pr escr ipt ions ar e associat ed t o t he diagnosis r isk for
infect ion. The charact erist ics of t he observed unit and
t he st r ong inst it ut ion policy r egar ding t he cont r ol of
indicators in this sector, such as infection rates and other
institutional guidelines, m ay be related to these results.
I t cannot be affir m ed t hat t he pr escr ipt ions
relat ed t o t he diagnosis risk for infect ion are exclusive
t o t h is d iag n osis, sin ce som e in t er v en t ion s can b e
r e c o m m e n d e d f o r d i f f e r e n t h u m a n r e s p o n s e s .
How ever, it was obser ved t hat , in t he pr esent st udy,
t hese it em s were associat ed wit h t he elem ent s of t hat
diagnosis: 42% w er e per t inent t o t he diagnosis t it le
( n= 73) , im ply ing infect ion cont r ol act ions; and 58%
of t he prescript ions ( n= 102) were direct ly relat ed wit h
r isk fact or s, denot ing infect ion pr ev ent ion act ions.
CONCLUSI ONS
Us i n g m e d i c a l r e c o r d s f o r r e t r o s p e c t i v e
s t u d i e s o f t h e n u r s i n g p r o c e s s c a n h a v e s o m e
lim it at ions in t erm s of t he cont ent of t he inform at ion
i n cl u d ed i n t h e r ecor d s. Th i s h as b een p r ev i ou sl y
report ed in lit erat ure, which can be relat ed t o t he lack
of i n f or m at i on , t h e q u al i t y of t h e r ecor d s, h av i n g
div er gen ces, t h e cov er age or r epr esen t at iv en ess of
t h e p a t i e n t s’ r e a l co n d i t i o n , a s w e l l a s p o ssi b l e
infor m at ion duplicit y or discont inuit y.
However, despit e t he bias, t he analysis of t his
i n f o r m at i o n r em ai n s p o si t i v e. Th ese asp ect s w er e
consider ed w hen pr oposing t he pr esent st udy.
According t o t he exam ined records regarding
t he ser v ice t o adult pat ient s hospit alized in I CU, t he
n u r ses:
- est ablished 24 different t ypes of diagnosis cat egories
( d i a g n o si s t i t l e s) , 1 5 co n ce r n i n g r e a l d i a g n o se s
( 62.5% ) and 9 risk diagnoses ( 37.5% ) , m ainly in t he
dom ains act ivit y/ r est ( 6) , and safet y/ pr ot ect ion ( 10) ;
- ident ified, m ost fr equent ly, t he diagnoses: r isk for
infect ion ( 84.6% ) ; im paired physical m obilit y ( 69.2% ) ;
r i s k f o r a s p i r a t i o n ( 6 5 . 3 % ) , a n d r i s k f o r i n j u r y
( 6 1 . 5 % ) ;
- m ade incom plet e r ecor ds of t he diagnoses, i. e., of
t h e 1 3 5 d i a g n o se s ( r e a l a n d r i sk ) , 1 3 3 ( 9 8 . 5 % )
present ed relat ed or risk fact ors, and only 39 ( 28.8% )
pr esen t ed t h e def in in g ch ar act er ist ics. I t sh ou ld be
st at ed t hat 42% w er e r eal, i.e., t hey should pr esent
t he defining char act er ist ics;
- est ablished m ost prescript ions ( 87.9% ) pert inent t o
t h e i d e n t i f i e d n u r si n g d i a g n o se s, l e a v i n g 1 2 . 1 %
w it hout any r elat ion;
- e s t a b l i s h e d p r e s c r i p t i o n s f o c u s e d o n n u r s i n g
d i a g n o si s m o st l y ( 9 0 % ) b a sed o n r el a t ed o r r i sk
f act or s, w h ile on ly 1 9 . 5 % w er e b ased on d ef in in g
ch ar act er ist ics;
- det erm ined t he diagnosis risk for infect ion based on
t h e i n f o r m a t i o n o b t a i n e d a t t h e m o m e n t o f d a t a
collect ion , ev iden cin g an accu r acy lev el su per ior t o
lit er at ur e r epor t s for diagnoses in gener al;
- est ablished nur sing pr escr ipt ions for t his diagnoses
consist ent ly wit h t he t it le ( 42% ) or wit h t he risk fact ors
( 5 8 % ) .
The use of differ ent nur sing pr ocess phases
a n d t a x o n o m i e s t o n a m e t h e d i a g n o s e s a n d
i n t e r v e n t i o n s p o r t r a y t h e n u r s e s ’ s e a r c h f o r
f ou n dat ion s t o base t h eir h ealt h car e on . How ev er,
t his pr ocess is not alw ay s fr ee fr om difficult ies. One
of t hese difficult ies is r ecor ding t hese st ages, w hich
is an indispensible st ep for developing and cont rolling
t h e h ealt h car e pr ocess. Th is r ecor d also per m it s a
cont inuous follow - up t o im plem ent t his m et hodology
effect ively, which should be done at t he st udy locat ion,
accor ding t o t he obt ained dat a.
REFERENCES
1 . Gr i f f i t h - K e n n e y J, Ch r i st e n se n PJ. N u r si n g Pr o ce ss: Applicat ion of t heories, fram ew orks and m odels. 2nd, St Louis ( MI ) : Mosb y ; 1 9 8 6 .
2. Carpenit o- Moyet LJ. Diagnóst ico de enferm agem : aplicação à pr át ica clínica. 10ª ed. Por t o Alegr e ( RS) : Ar t m ed; 2005. 3 . Nor t h Am er ican Nur sing Diagnosis Associat ion - NANDA. D i a g n ó s t i c o s d e En f e r m a g e m d a N A N D A : d e f i n i ç õ e s e classificação, 2005- 2006. Por t o Alegr e ( RS) : Ar t m ed; 2006. 4 . M c Cl o s k e y JC, B u l e c h e k GM . Cl a s s i f i c a ç ã o d a s I nt er v enções de Enfer m agem ( NI C) . 3ª ed. São Paulo ( SP) : Ar t m ed ; 2 0 0 4 .
5 . Mo o r h ead S, Jo h n so n M, Maas ML. Nu r si n g o u t co m es classificat ion 3r d ed St Lou is ( MO) : Mosby ; 2 0 0 3 .
6. Müller- St aub M, Lav im MA, Needham I , vanAcht er ber g T. Nur sing diagnoses, int er v ent ions and out com es: applicat ion an d im p act on n u r sin g p r act ice: sy st em at ic r ev iew . J Ad v Nu r s 2 0 0 6 ; 5 6 ( 5 ) : 5 1 4 - 3 1 .
7. Helberg JL. Pat ient s’ st at us at hom e care discharge. I m age J Nu r s Sch 1 9 9 3 ; 2 5 ( 2 ) : 9 3 - 9 .
9 . Cu n h a SMB, Bar r os ALB. An álise d a im p lem en t ação d a Sist em at ização d a Assist ên cia d e En f er m ag em , seg u n d o o Modelo Conceit ual de Hor t a. Rev Br as Enfer m 2005; 58( 5) : 5 6 8 - 7 2 .
1 0 . Le e TT, Mi l l s ME. Th e r e l a t i o n s h i p a m o n g m e d i c a l diagn osis, n u r sin g diagn osis, an d n u r sin g in t er v en t ion an d t h e im p licat ion s f or h om e h ealt h car e. J Pr of Nu r s 2 0 0 0 ; 1 6 ( 2 ) : 8 4 - 9 1 .
11. Currel R, Urquhart C. Nursing record syst em s: effect s on n u r s i n g p r a c t i c e a n d h e a l t h c a r e o u t c o m e s . Co c h r a n e Dat abase of Sy st em at ic Rev iew 2 0 0 3 ( 3 ) .
1 2 . Nah m R, Post on I . Measu r em en t s of t h e ef f ect s of an int egrat ed, point - of care com put er syst em on qualit y of nursing docum ent at ion and pat ient sat isfact ion. Com put Nur s 2000; 1 8 ( 5 ) : 2 2 0 - 9 .
13. Daly JM, Buckw alt er K, Maas M. Writ t en and com put erized car e plans. J Ger ont ol Nur s 2 0 0 2 ; 2 8 ( 9 ) : 1 4 - 2 3 .
1 4 . Sán ch ez RR, Lan d er os MS, Con t r er as MFP, Sep ú lv ed a EC, M u ñ o z GP. Pr o c e s s o f n u r s i n g : a t t e n t i o n t o o l i n m anagem ent of t he car e. Enfer m er ía 2002; 37( 120) : 2- 5. 1 5 . M a r q u e s LV P; Ca r v a l h o D V. S i s t e m a t i z a ç ã o d a a s s i s t ê n c i a d e e n f e r m a g e m e m c e n t r o d e t r a t a m e n t o int ensivo: percepção das enferm eiras. Rev Min Enferm 2005; 9 ( 3 ) : 1 9 9 - 2 0 5 .
1 6 . Mü ller - St au b M, Need h am I , Od em b r eit M, Lav in MA, VanAcht erberg T. I m proved qualit y of nursing docum ent at ion: r esult s of a nur sing diagnoses, int er v ent ions and out com es i m p l e m e n t a t i o n st u d y. I n t N u r s Te r m i n o l Cl a ssi f 2 0 0 7 ; 1 8 ( 1 ) : 5 - 1 7 .
1 7 . Con sid in e J. Th e r ole of n u r ses in p r ev en t in g ad v er se
event s relat ed t o inspirat ory dysfunct ion: lit erat ure review . J Ad v Nu r s 2 0 0 5 ; 4 9 ( 6 ) : 6 2 4 - 3 3 .
1 8 . Lu n n e y M . Pe n s a m e n t o c r ít i c o e d i a g n ó s t i c o s d e enfer m agem . Est udos de caso e análises. Por t o Alegr e( RS) : Ar t m ed ; 2 0 0 4 .
1 9 . Og a s a w a r a C, H a s e g a w a T, Ku m e Y, Ta k a h a s h i I , Ka t a y a m a Y, Fu r u h a sh i Y e t a l . Nu r si n g d i a g n o se s a n d i n t er v en t i on s of j ap an ese p at i en t s w i t h en d - st ag e b r east ca n ce r a d m i t t e d f o r d i f f e r e n t ca r e p o u r p o se s. I n t Nu r s Ter m in ol Classif 2 0 0 5 ; 1 6 ( 3 - 4 ) : 5 4 - 6 4 .
20. Coenem A, Ryam P, Sut t on J, Devine E, Werley HH, Kelber S. Use of t he Nursing Minim um Dat a Set t o describe nursing int ervent ions for select nursing diagnoses and relat ed fact ors in an acut e car e set t ing. Nur s Diagn 1995; 6( 3) : 109- 14. 2 1 . Le v i n RF, Lu n n e y M, Kr a i n o v i ch - Mi l l e r B. I m p r o v i n g diagnost ic accur acy using an ev idence- based nur sing m odel. I n t Nu r s Ter m in ol Classif 2 0 0 4 ; 1 5 ( 4 ) : 1 1 4 - 2 2 .
22. Lunney M, Karlic B, Kiss M, Musphy P. Accuracy of nurse’s d i a g n o se s o f p sy ch o so ci a l r e sp o n se s. Nu r s D i a g n 1 9 9 7 ; 8 ( 4 ) : 1 5 7 - 6 6 .
2 3 . Jesu s CAC, Car v alh o EC. Br azilian Nu r ses Accu r acy in Nam i n g Di ag n o st i c St at em en t s. I n : Ran t z MJ, LeMo n e P. ( o r g a n i z a t o r s . ) . Cl a s s i f i c a t i o n o f N u r s i n g D i a g n o s e s -Pr oceed in g s of t h e Fou r t een t h Con f er en ce. Glen d ale ( CA) : Cin ah l I n for m at ion Sy st em s; 2 0 0 2 . p. 1 2 2 - 6 .
24. Lee TT. Nur sing diagnoses: fact or s affect ing t heir use in charting standardized care plans. J Clin Nurs 2005; 14: 640- 47. 25. Sm it h- Higuchi KA, Dulber g C, Duff V. Fact or s associat ed w it h nursing diagnosis ut ilizat ion in Canada. Nurs Diagn 1999; 1 0 ( 4 ) : 1 3 7 - 4 7 .