w w w . r b o . o r g . b r
Original
article
Functional
evaluation
of
arthroscopic
treatment
of
SLAP
lesions
through
the
O’Brien
portal
夽
Fabiano
Rebouc¸as,
Bruno
Cesar
Pereira,
Ricardo
Dantas
Rocha
∗,
Cantídio
Salvador
Filardi,
Miguel
Pereira
da
Costa,
Romulo
Brasil
Filho,
Antonio
Carlos
Tenor
Junior
HospitaldoServidorPúblicoEstadual,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received25August2013 Accepted29May2014 Availableonline12June2015
Keywords: Shoulderjoint
Shoulderdislocation/surgery Jointinstability
Arthroscopy
a
b
s
t
r
a
c
t
Objective:ToevaluatethefunctionalresultsfromarthroscopicrepairofSLAPlesionsthrough theportaldescribedbyO’Brien.
Methods:A retrospectiveevaluationwasconductedon19 shouldersin18 patientswho underwent arthroscopic repair of SLAP lesions through the O’Brien portal between November2007andJanuary2012.
Results:Nineteenshouldersin18patientswereevaluated:16malepatients(84.2%)andthree femalepatients(15.7%).Thepatients’agesrangedfrom27to40years(meanof34.3years). Therewere12patients(63.1%)withinjuriesontherightshoulder,six(31.5%)withinjuries ontheleftshoulderandone(5.2%)withbilateralinjury.Inrelationtodominance,13patients (68.4%)presentedtheinjuryonthedominantlimbandfive(26.3%)wereaffectedonthe non-dominantlimb.Weobservedthatninecases(47.3%)hadSLAPlesionsaloneand10cases (52.6%)wererelatedtoglenohumeralinstability.Therewasonecase(5.2%)ofrecurrenceof glenohumeraldislocation,butthispatientchosenottoundergoanewsurgicalintervention. AccordingtotheUCLAandASESscalestranslatedandadaptedtothePortugueselanguage, 96%oftheresultsweregoodorexcellent.
Conclusion:TheapproachfortreatingSLAPlesionsthroughtheportaldescribedbyO’Brien etal.iseasytoreproduce,withahighrateofgoodandexcellentresultsandalow compli-cationrate.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Avaliac¸ão
funcional
do
tratamento
artroscópico
da
lesão
SLAP
pelo
portal
O’Brien
Palavras-chave: Articulac¸ãodoombro
r
e
s
u
m
o
Objetivo:AvaliarosresultadosfuncionaisdoreparoartroscópicodalesãoSLAPpeloportal descritoporO’Brien.
夽
WorkdevelopedintheDepartmentofOrthopedicsandTraumatology,HospitaldoServidorPúblicoEstadual,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](R.D.Rocha). http://dx.doi.org/10.1016/j.rboe.2015.05.006
Luxac¸ãodoombro/cirurgia Instabilidadearticular Artroscopia
Métodos:Foifeitaavaliac¸ãoretrospectivade19ombrosde18pacientessubmetidosaoreparo artroscópicodalesãoSLAPpeloportaldeO’Brien,denovembrode2007ajaneirode2012. Resultados: Foram avaliados19 ombrosde 18 pacientes,16 (84,2%) dosexomasculino etrês(15,7%) dofeminino.A idadevarioude27 a40anos (médiade34,3).Noestudo, 12 (63,1%)pacientestiveram lesão noombrodireito,seis(31,5%) noombroesquerdoe houveum(5,2%)casodelesãobilateral.Emrelac¸ãoà dominância,13(68,4%)pacientes apresentaramalesãonomembrodominanteecinco(26,3%)tiveramomembronão domi-nanteacometido.Observamosquenove(47,3%)casostiveramlesãoSLAPisolada,10(52,6%) casosforamrelacionadosainstabilidadeglenoumeraleapenasum(5,2%)casoteverecidiva daluxac¸ãoglenoumeral.Essepacienteoptoupornãofazernovaintervenc¸ãocirúrgica.De acordocomasescalasULCAeASEStraduzidaeadaptadaparaalínguaportuguesa,obteve-se 96%deexcelentesebonsresultados.
Conclusão:AabordagemdalesãoSLAPpeloportaldescritoporO’Brienetal.édefácil repro-dutibilidade,comaltoíndicedeexcelentesebonsresultadosebaixoíndicedecomplicac¸ões. ©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Withtheadventofarthroscopyoftheshoulder,itisnow possi-bletodiagnosetypesoflabrallesionthatwasnotdiagnosedby meansofradiographicmethods.Onetypeoflesioninvolving theupperareaoftheglenoidlabrum,whichbegins posteri-orlyandextendsanteriorlytotheglenoidcavity,isnamedthe SLAPlesion(superiorlabrumanteriorandposterior).Thisarea oftheglenoidlabrumisfunctionallyimportantfortheupper stabilityoftheshoulderandalsoservesasan“anchor”forthe insertionofthelongheadofthetendonofthebicepsbrachii muscle.1,2
SLAPlesionswerefirstdescribedbyAndrewsetal.3in1985 andweresubsequentlyclassifiedintofoursubtypesbySnyder etal.1in1990.In1995,Maffetetal.4addedtypeVtothe clas-sificationofSnyderetal.1Thiscompriseslesionsoftheupper glenoidlabrumthatextends totheanteroinferiorregion.In 1998,Morganet al.5 subdividedtypeII into threesubtypes accordingtothelocation ofthelesionintheupperglenoid labrum:anterior,posteriororcombined.
TheexactetiologyofSLAPlesionsremainsamatterof con-troversy.However,twopossiblecauseshavebeendescribedin theliterature:compressionforcesappliedtotheglenohumeral jointconsequenttoafallwiththeshoulderinapositionof abductionandflexion;ortensionforcesappliedtothearm, causedbyatractionmechanismappliedtotheupperlimbasa resultofathrowingmovement,whichisparticularlyobserved amongbaseballplayers.6–8
Theobjectiveofthepresentstudywastoevaluatethe func-tionalresultsfromarthroscopicrepairofSLAPlesionsthrough theportaldescribedbyO’Brien.9,10
Materials
and
methods
A retrospective evaluation was performed on 19 shoul-ders of 18 patients who underwent arthroscopic repair of SLAP lesions through the O’Brien portal between Novem-ber2007andJanuary2012.Theinclusioncriterionwasthat
the patients undergoing arthroscopic surgical treatmentof SLAP lesions had not responded clinically to conservative treatment.Patientswithhistoriesofprevioussurgeryor extra-articulardiseases intheshoulderthat wastobeevaluated wereexcluded.
SLAP lesionswere diagnosedwhentherewas apositive O’Brientestinassociationwithmagneticresonanceimaging ofthekneesuggestiveofalesionintheupperglenoidlabrum andarthroscopicobservationofthelesion.
The following were recorded: the time that elapsed betweenthestartofsymptomsofthelesionandthesurgical treatment;andthepatient’sage,sex,occupationandreturn tosport(activitylevel).Postoperativefunctionwasassessed using theUCLAand ASESscalesinthe versionstranslated andadaptedtothePortugueselanguage.2,11–13Datawere gath-ered by means of physicalexamination (O’Brien, Jobe and Patte tests)and aquestionnairethat wasappliedtoall the patients.
Thesurgicalprocedureswereperformedbythesame sur-gicalteam,withthepatientundergeneralanesthesia,without blockage ofthe brachialplexus. Thepatient wasplacedin the“deckchair”position.Aposteriorportalwasusedto intro-duce the arthroscopic opticaldevice, and this was located 2cm distallyand 2cmmedially tothe posterolateral angle oftheacromion.Thejointwasinvestigatedusingthe refer-encepointofthetendonofthelongheadofthebicepsbrachii muscleanditsupperlabralorigin.Followingthis,the ante-rior,inferiorandposteriorlabra,jointsurfaces,glenohumeral ligaments,rotatorcuff,capsuleandjointrecesseswere eval-uated.
Thefollowingintraoperativediagnostic criteriaforSLAP lesions were then used:a positivedrive-throughtest (easy passageofthearthroscopicopticaldevicethroughthe gleno-humeral space); positive peel-back test (glenoid labrum openinggreaterthan1cmduringabductionandexternal rota-tionoftheshoulder);anddirectviewingofthedegenerated andfibrillatedlabraltissuewithsignsofavulsion14(Fig.1).
UL
S
GC
Fig.1–IdentificationofSLAPlesion(arrow).UL,upper labrum;S,SLAPlesion;GC,glenoidcavity.
Posterior portal
Portal passing through
rotator cuff Anterior
portal Coracoid
process
Fig.2–Demarcationoftheboneanatomicalparameters andprobablelocationoftheanteriorportalandtheportal passingthroughtherotatorcuff.
ofneurovascularinjuries.Thiscannulawasplacedabovethe upperborderofthetendonofthesubscapularmuscle(anterior rotatorinterval).
ToconstructthearthroscopicportaldescribedbyO’Brien etal.9(portal2)(Fig.2)andplacethesecond8.5mmcannula,a
Fig.4–Openingupoftheupperglenoidrimusinga shavingblade.
Jelcono.14needlewasplacedinthesuperolateralregionofthe shoulder,throughtherotatorcuff,inthedirectionofthe pos-terosuperiorregionoftheglenoid(Fig.3).Thelocationofthe portalvariedaccordingtotheanatomyofthepatient’s shoul-derandthelocationoftheposteriorlabraldeinsertion,with theaimoffacilitatingaccesstotheposterosuperiorregionof glenoidandtotheglenoidlabrum.
After the portals had been constructed, the process of opening up the upper glenoid rim (and the anterior rim when necessary) was started, using a 4mm bone shaving blade (Fig. 4), in order to form a bloody bed that would favorhealingofthelabrum-capsulecomplexthatwouldbe reinserted.
Toreinserttheglenoidlabrum,twoabsorbablepolylactic acidanchorsofsize2.7mwereplacedusingnonabsorbable thread,startingfromtheanterosuperiorregion.Theanterior portal(portal1)wasusedasthemainoneandthe O’Brien portal (portal 2) was used as an auxiliary. To reinsert the labrum posteriorlytothe tendonofthe biceps,the O’Brien portal(portal2)wasusedasthemainoneandtheanterior portal(portal1)asanauxiliary.Topassthethreadsthrough theglenoidlabrum,curvedbird-beakinstrumentsalonewere used(Fig.5A–F).
Inthecasesinwhichthepatientpresentedanterior gleno-humeralinstabilitywithananteroinferiorlesionoftheglenoid
Fig.5–(A)ArthroscopicviewofthecannulaeattheanteriorportalsofO’Brien(arrows).(B)Anteriorlabrumreinsertedand anchorinsertedattheposteriorglenoidrim.(C)Passageofbirdbeakthroughtheposterosuperiorglenoidlabrum.
(D)Suturingoftheposteriorlabrum.(E)Stabilitytestontheupperglenoidlabrumusingprobe.(F)Negativepeel-backtest.
labrum(Bankartlesion),labralreinsertionwasalwaysstarted inananticlockwisedirection,fromtheanteroinferiorregion tothe posteriorregion,usinganothertwoanchors(totalof four).Afterlabralreinsertion,dermalsuturingoftheportals wasperformedandtheoperatedlimbwasthenimmobilized usingaVelpeausling.
Results
Nineteenshoulderswereevaluated,in18patients:16males (84.2%)andthreefemales(15.7%).Theminimum postopera-tive follow-up was seven months and the maximum was 56 months(mean of33.9). The patients’ ages rangedfrom 27to40years(meanof34.3).Therewere12patients(63.1%) withalesionintherightshoulder,sixcases(31.5%)intheleft shoulderandonecase(5.2%)ofbilaterallesions.Inrelation todominance,13patients(68.4%)presentedthelesioninthe dominantlimbandfive(26.3%)inthenon-dominantlimb.
Fromtheevaluationsonthese19shoulders,weobserved thatninecases(47.3%)hadSLAPlesionsalone,10cases(52.6%) were related to glenohumeralinstability and a single case (5.2%)presentedrecurrenceofglenohumeraldislocation.This patientdecidednottoundergo anewsurgicalintervention (Table1).
Inrelationtosportsactivity,ninepatientswerepracticing avarietyofsportsbeforetheinjury(volleyball,swimmingand
tennis)andninewerenot.Afterthesurgicaltreatment,eight oftheninepatientsreturnedtothesportsthattheyhadbeen doingbeforethetreatment.Onepatientdidnotreturntothe sportsactivitythathehadpracticed,buthedidnotcorrelate thiswiththesurgicalresult.
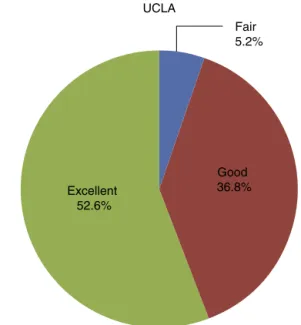
AccordingtotheUCLAscale,asadaptedtothePortuguese language,10patients(52.6%)obtainedresultsthatwere con-sideredtobeexcellent,seven(36.8%)presentedgoodresults, asinglepatient(5.2%)obtainedafairresultandthesewereno poorresults2,13(Fig.6).
Table1–SampleofpatientswithSLAPlesionswho
underwentsurgicaltreatment.
No.ofshoulders 19
No.ofpatients 18
Meanage(years) 34.3
Sex
Male 16(84.2%) Female 3(15.7%)
Limbaffected
Right 12(63.1%)
Left 6(31.5%)
Fair 5.2%
Good 36.8% Excellent
52.6%
UCLA
Fig.6–Resultfrompostoperativeevaluationaccordingto UCLAscale,asadaptedtothePortugueselanguage.
InrelationtotheASESscale,asadaptedtothePortuguese language,58%ofthe patientsobtainedscoresof100%,17% obtained95%,21%obtained90%and4%obtained70%(Fig.7). Allthe18patients,whoallcompletedthestudyfollow-up, presentednegativeJobeandPattetestsinthephysical exami-nationconductedatthetimeofthefunctionalevaluation.The meantimetakenforreleasefromtheoutpatientfollow-upwas sixmonths.
Discussion
In our sample, we found epidemiological agreement with theliteratureconsulted,withpredominanceofSLAPlesions inmales (84.2%)and higher frequencyof lesions affecting thedominantlimb(68.4%).1,6,8,10,11Themeanageamongour patientswas34.3years,whichwassimilartotheagefound
1 (4%)
5 (21%)
4 (17%)
14 (58%) ASES
100%
95%
90%
70%
Fig.7–Resultfrompostoperativeevaluationaccordingto ASESscale,asadaptedtothePortugueselanguage.
inthestudybyMiyazakietal.,6butgreaterthanthatofother studies.7,11
ThetreatmentforSLAPlesionsvariesfromconservativeto arthroscopicsurgery.Inarthroscopicprocedures,an anterosu-periorand/oranteroinferiorportalisusedinmostcases,with aroutethroughtherotatorintervaltoreachthelabrallesions oftheupperandlowerglenoid.Theseportalslimitaccessto theposteriorandsuperiorregionoftheglenoidforplacement ofananchorandreinsertionoftheposteriorlabrum.
Accessoryportalsforattemptingtofacilitate posterosupe-rioraccesshavebeendescribed,suchastheNeviaserportal andtransacromialportals.However,thereisariskofinjuryto thesuprascapularnerveandfracturesoftheacromion.14–16
More recently, Warner et al.17 described the use of an anterolateralportalforaccessingtheposterosuperiorregion oftheglenoidlabrum.However,this portalwouldrequirea wideincisioninthetendonoftherotatorcuff.
O’Brienetal.9developedaportalforaccessingupperlabral lesionsthatwouldenableaccesstotheanteriorand postero-superiorregionsoftheglenoidlabrum.Thiswasdescribedasa reliabletechniquethatwaseasilyreproducible,usinganeedle tolocatethemostappropriateregionforaccessingthe poste-riorlabrallesions.Thepotentialriskofinjurytotherotator cuffwasminimizedbyusingcannulaeofsmallerdiameters, whichonlygaverisetodivulsionofthefibersatthe muscle-tendonjunctionofthesupraspinatusmuscle.
InthestudybyO’Brienetal.,9arthroscopicrepairofSLAP lesionswasperformedin31patientsusingaportalpassing throughtherotatorcuff.Noinjuriestotherotatorcuff con-firmed by magneticresonance imagingwere observed. Oh etal.18obtainedexcellentpostoperativeresultsfrom arthro-scopicrepairstoSLAPlesionsusingaportalpassingthrough therotatorcuffin58shoulders,thusconfirmingthesafetyand efficiencyofthisportal.Inoursample,noevidenceof weak-nessoftherotatorcuff,asassessedthroughtheJobeandPatte tests,wasobserved.Norwasthereanydiminutionoftherange ofmotionoftheoperatedshoulder.
In our series of 19 shoulders, in 18 patients who were treatedforSLAPlesionswithameanpostoperativefollow-up of33.9months,goodclinicalresultswerefoundthrough eval-uationsusingthe ASESand UCLAscales,astranslatedand adaptedtothePortugueselanguage.Itwasfoundthat96%of theresultswereexcellentorgood,similartothefindingsfrom otherstudies.6,8,18
Conclusion
ThepresentstudydemonstratedthataccessingSLAPlesions from portalspassingthrough therotator cuff,as described byO’Brienetal.,waseasilyreproducible,withahighrateof excellentandgoodresultsandalowcomplicationrate.
Conflicts
of
interest
r
e
f
e
r
e
n
c
e
s
1. SnyderSJ,KarzelRP,DelPizzoW,FerkelRD,FriedmanMJ.Slap lesionsoftheshoulder.Arthroscopy.1990;6(4):274–9.
2. KeenerJD,BrophyRH.Superiorlabraltearsoftheshoulder: pathogenesis,evaluation,andtreatment.JAmAcadOrthop Surg.2009;17(10):627–37.
3. AndrewsJR,CarsonWGJr,McLeodWD.Glenoidlabrumtears relatedtothelongheadofthebiceps.AmJSportsMed. 1985;13(5):337–41.
4. MaffetMW,GartsmanGM,MoseleyB.Superiorlabrum-biceps tendoncomplexlesionsoftheshoulder.AmJSportsMed. 1995;23(1):93–8.
5. MorganCD,BurkhartSS,PalmeriM,GillespieM.TypeIISlap lesions:threesubtypesandtheirrelationshipstosuperior instabilityandrotatorcufftears.Arthroscopy.
1998;14(6):553–65.
6. MiyazakiAN,FregonezeM,SantosPD,SilvaLA,SellaGV, SoaresAL,etal.Avaliac¸ãodosresultadosecomplicac¸õesda suturaastroscópicadalesãoSlap.RevBrasOrtop.
2011;46(1):51–6.
7. SelbyRM,AltchekDW,DiGiacomoG.TheDiGiacomo technique:simplifiedsuturepassinginSlaprepair. Arthroscopy.2007;23(4):439,e1–2.
8. KimSH,HaKI,KimSH,ChoiHJ.Resultsofarthroscopic treatmentofsuperiorlabrallesions.JBoneJointSurgAm. 2002;84(6):981–5.
9. O’BrienSJ,AllenAA,ColemanSH,DrakosMC.The
trans-rotatorcuffapproachtoSlaplesions:technicalaspects forrepairandaclinicalfollow-upof31patientsata minimumof2years.Arthroscopy.2002;18(4):372–7.
10.BrockmeierSF,VoosJE,WilliamsRJ3rd,AltchekDW,Cordasco FA,AllenAA.Outcomesafterarthroscopicrepairoftype-II SLAPlesions.JBoneJointSurgAm.2009;91(7):
1595–603.
11.GodinhoGG,FreitasJMA,LeiteLMB,PinaERM.LesõesSlapno ombro.RevBrasOrtop.1998;33(5):345–52.
12.ColemanSH,CohenDB,DrakosMC,AllenAA,WilliamsRJ, O’BrienSJ,etal.ArthroscopicrepairoftypeIIsuperiorlabral anteriorposteriorlesionswithandwithoutacromioplasty:a clinicalanalysisof50patients.AmJSportsMed.2007;35(5): 749–53.
13.KimTK,QuealeWS,CosgareaAJ,McFarlandEG.Clinical featuresofthedifferenttypesofSlaplesions:ananalysisof onehundredandthirty-ninecases.JBoneJointSurgAm. 2003;85(1):66–71.
14.McFarlandEG,NeiraCA,GutierrezMI,CosgareaAJ,MageeM. Clinicalsignificanceofthearthroscopicdrive-throughsignin shouldersurgery.Arthroscopy.2001;17(1):38–43.
15.KatzLM,HsuS,MillerSL,RichmondJC,KhetiaE,KohliN, etal.PooroutcomesafterSlaprepair:descriptiveanalysis andprognosis.Arthroscopy.2009;25(8):849–55.
16.CoenMJ,JobeCM,PakK.Acromialcompromisewithuseofa transacromialportal:abiomechanicalstudy.JShoulderElbow Surg.1995;4(4):249–53.
17.WarnerJJ,KannS,MarksP.Arthroscopicrepairofcombined Bankartandsuperiorlabraldetachmentanteriorand posteriorlesions:techniqueandpreliminaryresults. Arthroscopy.1994;10(4):383–91.