rev bras hematol hemoter. 2017;39(1):66–69
w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Case
report
Plasma
cell
leukemia
with
t(11;14)(q13;q32)
simulating
lymphoplasmacytic
lymphoma
–
a
diagnostic
challenge
solved
by
flow
cytometry
Aleyde
Diniz
Loureiro
a,
Matheus
Vescovi
Gonc¸alves
a,
Maura
Rosário
Valério
Ikoma
b,
Maria
Regina
Regis
Silva
a,
Gisele
Wally
Braga
Colleoni
a,
Maria
de
Lourdes
Chauffaille
a,
Mihoko
Yamamoto
a,∗aUniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
bFundac¸ãoAmaralCarvalho,Jau,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received6September2016 Accepted10October2016 Availableonline22December2016
Introduction
Plasmacellleukemia(PCL)isarareandaggressive manifes-tationofmalignantplasmacellproliferationandcorresponds to2–4%ofmultiplemyeloma(MM)cases.1,2TheWorldHealth Organization(WHO)definesPCLbythepresenceofhighlevels (atleast2×109/L)ofclonalplasmacellsintheperipheralblood (PB)oratleast20%oftheleukocytedifferentialcount.1 Pri-maryPCL(pPCL)correspondsto60%ofthecasesandpresents as leukemia at diagnosis, usually with tissue infiltration, organomegalyandlymphadenopathyandalowerfrequency ofbonelesions(15–40%cases)thanmultiplemyeloma.2 Sec-ondaryPCListheterminalphaseofMMandcorrespondsto theremaining40%ofPCLcases;itusuallyhasapoorresponse tostandard MMtreatment.2,3 The diagnosis ofplasmacell neoplasmsiseasilysuggestedbythecharacteristicplasmacell
∗ Correspondingauthorat:DisciplinadeHematologiaeHemoterapia,EscolaPaulistadeMedicina(EPM),UniversidadeFederaldeSão
Paulo(UNIFESP),RuaDr.DiogodeFaria,824,3◦Andar,04037-003SãoPaulo,SP,Brazil.
E-mailaddress:[email protected](M.Yamamoto).
morphology,bothinMMandinPCL.Thegreatcontributionof immunophenotypingbyflowcytometry(FC)insuchdisorders depends on differentiatingnormal from neoplastic plasma cells.4,5However,inrarecasesofMMwithatypical morphol-ogythedifferentialdiagnosiswithotherlymphoproliferative disordersmaybeachallenge.Here,wepresentacaseofpPCL inwhichthediagnosisoflymphoplasmacyticlymphoma(LPL) wasinitiallysuggestedbymorphologyofperipheralblood(PB) andbonemarrow(BM)cells(aspirateandbiopsy)withthefinal diagnosisofpPCLbeingestablishedbyFC.
Case
report
A 77-year-old female patient consulted in the Rheuma-tology Service of the Hospital São Paulo for osteoporosis and was referred to the Hematology Clinic to investigate
http://dx.doi.org/10.1016/j.bjhh.2016.10.001
rev bras hematol hemoter. 2017;39(1):66–69
67
Figure1–Neoplasticcellmorphologyinperipheralblood(A)andbonemarrowaspiratefilms(B)showingsmall-to medium-sizedlymphoplasmacyticlymphocytes(MayGrunwaldGiemsastain,1000×).Bonemarrowbiopsy(C)replacedby
medium-sizedlymphocytes(C1;Hematoxylinandeosin stain,400×)andimmunohistochemistryexpressionofKi67of tumorcells(C2;immunoperoxidase,400×).
1000
1000 900
900 800
800 700
700 600
600 500
500 400
400 300
300 200
200 100
100 0
FSC–height CD45 PerCP
CD38 APC
CD20 APC
Normal B cells
Normal B cells
0
SSC–height
1000
900
800
700
600
500
400
300
200
100
0
1 1E1 1E2 1E3 1E4
1E1 1E2 1E3 1E4 1
1 1
3 1E1 1E1
1E2 1E2
1E3 1E3
1E4 1E4
SSC–height
CD19 PE
CD138 FITC
1 1
1E1 1E1
1E2 1E2
1E3 1E3
1E4 1E4
CD38 APC
CD38:FITC–A CD117:APC–A
0 0
50
1E2 1E3
1E3 1E3
1E2
1E2 1E2
1E1
–1E2
1E5 1E4
1E4 1E4
1E3 1E5
1E5
1E4 0 1E2
–1E2 1E3 1E4 1E5
CD81:APC–H7–A
CD28:PE–A
CD56 PE
cLambda FITC
1E1 1E2 1E3 1E4 1
1 1E3
1E2
1E1 1E4
cKappa PE
Figure2–Flowcytometrydotplotsofthecirculatingplasmacells(inblackdots)showingsmall-tolarge-sizedclonal plasmacellsexpressing(forward/sidescatteroflight)CD45−,CD19/CD20−,CD38++/CD138+heterogeneousand
68
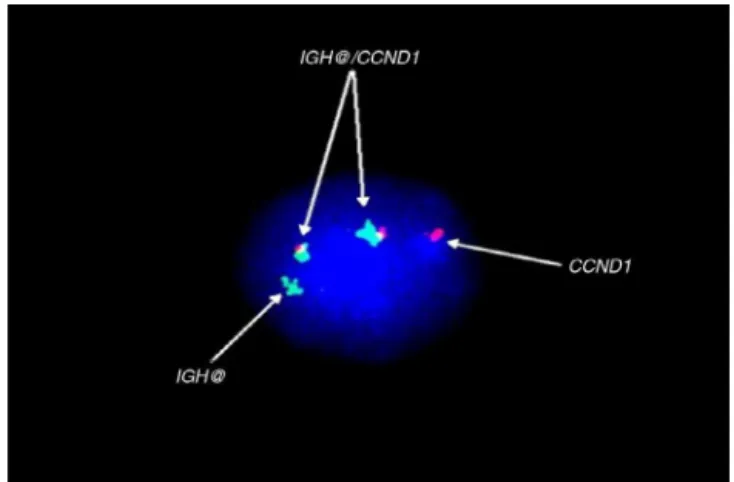
rev bras hematol hemoter. 2017;39(1):66–69Figure3–FISHusingprobesfortheCCND1 gene(red)and IGH gene(green),andredandgreenfusion,corresponding
toIGH-CCND1 rearrangement.
anemia. At physical examination, she was in good gen-eral condition without palpable lymph nodes, or liver or spleen enlargement. The complete blood count showed: Hemoglobin=10.1g/dL; Hematocrit=32.4%;white blood cell count8.6×109/L (neutrophils: 37%; lymphocytes: 58%) and platelet count140×109/L.Morphological analysisofthePB smearshowedsmall-tomoderate-sizedlymphoplasmacytoid lymphocytes(75%ofthelymphocytes)withbasophilic cyto-plasmand 1to 2nucleoli(Figure1A). BMaspirateshowed 90%oflymphocyteswiththesamecharacteristicsand5.6% oftypicalplasmacells(Figure1B).BMbiopsyshowed hyper-cellularmarrowwith80%ofyoung,small-tomedium-sized lymphoid cells (Figure1C). BMimmunohistochemistrywas inconclusive: tumor cells were negative for all of the fol-lowingantigens:CD45, CD3,CD5,CD10,CD20, CD23,CD30, CD79a,CD138,PAX5,CD1A,CD56,TdT,kappa,lambdaand cyclin D1, but the Ki67 was positivein about 40% ofcells. Theother laboratorialtestsshowedtotalserumproteinsof 10.2g/dL,albuminof3.83g/dL and monoclonalpeakinthe gamma globulinregion(4.4g/dL) thatwas identifiedasIgG byimmunofixation;normaltotalserumCa(10.8mg/dL)with ionic Ca 1.45mM/L (normal 1.15–1.32mM/L) and increased beta-2 microglobulin(4.7mg/L).Lytic lesions were seen on skullX-ray.Immunophenotyping byFCofBMcellsshowed thepresenceofclonalplasmacells (40%)expressing CD38, CD138dim, cykappa, smkappa, -2microglobulin and CD81, and were negative forCD45, CD56, CD19, cylambda, CD28 andCD117,suggestingaplasmacellmalignancydespitethe morphologicfeaturesofLPL(Figure2).SmallBlymphocytes (1.17%)expressedthenormalBcellphenotype(CD45++,CD 19+,CD20++,CD79b+,CD24+,FMC-7+,smKappa+/smLambda+ ratio of2:1, and negativeforthe CD5, CD10, CD11c, CD23, CD200,CD38,CD43antigens).Thefinal diagnosis wasPCL, IgG kappa. A fluorescent in situ hybridization (FISH) study waspositiveforcyclinD1(PRAD1,CCND1)/IGHrearrangement, showingthepresenceoft(11;14)(q13;q32)(Figure3). Consid-eringthe age ofthe patient(>70 years old)and transplant ineligibility,thetreatmentoptionwasmelphalan,thalidomide anddexamethasone.However,thepatientevolvedwith wors-eningofperformancestatusandgastricdiscomfortandshe
decidedtostopthethalidomide.Duetotheworseningofher clinicalcondition,itwasdecidedtouseonlydexamethasone (40mg/week)andclosemonitoringofherclinicalcondition. Afterthreemonths,thepatientsufferedapathologicalfemur fractureandeventuallydiedofpulmonarysepsis.
Discussion
pPCLisararediseasethataffectsyoungerindividuals;ithas asubacuteonsetandpatientshaveapoorerperformance sta-tus(ISS3inabout60%ofcases)atdiagnosisthanthosewith MM.1,2,6 Thereisahigh incidenceofanemiaand thrombo-cytopenia duetothe suppressionofnormalhematopoiesis intheBMwhichisusuallygreatlyinfiltrated.2,4,6Moreover, pPCLhasahigherincidenceofextramedullaryinvolvement that appears to be a result of a lower expression of cell adhesion molecules, such as CD56, facilitating the release ofleukemicplasmacellsfromtheBMmicroenvironment.4,5 Our patient had no evidence of extramedullary disease at diagnosis, but she presented mild anemia and was under treatment for osteoporosis. Her BM biopsy showed exten-siveinvolvementbylymphoplasmacytoidcellsthathadthe same characteristics asinthe PB,which sometimesmakes the differential diagnosis between LPL and PCLdifficultby morphological analysis alone. Immunohistochemistry was inconclusiveas,unexpectedly,theexpressionofCD138was negativeinneoplasticcells.Thereasonsforthismaybedue todown-regulationoftheantigenorthesamplepreparation process.Inthis particularcase,FChadakey rolein estab-lishing the correctdiagnosis.4,5,7,8 Normal plasma cells are CD19+/CD45+/CD38bright/CD56−whileneoplasticplasmacells are usuallyCD19−/CD45−/CD38+/CD56+.5,8 However,asseen inthepresentcase,PCLcells showalowexpressionofthe cell adhesionmoleculeCD56suggestingaworseprognosis; thiswasassociatedwiththepresenceofneoplasticcellsin thePB.4,9LPLismorphologicallycharacterizedbythepresence ofsmallplasmacytoidlymphocytesandsomeplasmacellsin whichtheimmunophenotypeusuallyresemblesthenormal lymphocytes and plasma cells exceptfor clonalrestriction andCD25+/− andCD138+/−expression.Thisdiffersfromthe immunophenotypeprofileofneoplasticplasmacellsfoundin thiscase.1,7,8,10
Furthermore, FC can also give additional information relatedtotheprognosisinplasmacellneoplasms.The expres-sions of B2 microglobulin and CD81, both positive in the currentcase,andtheabsenceofCD45arerelatedtoanadverse prognosis.5,11 Expression of CD28represents an aggressive phenotype associated with tumor expansion and shorter disease free survival.5 In our patient, the malignant cells expressedanunfavorableimmunophenotypicprofileexcept fortheabsenceofCD28.Plasmacells,eithernormalor malig-nant,usuallyexpressCD138,butmalignantplasmacellsmay have dim expressionofthis marker, which maybe dueto down-regulationofthisantigen.Importantly,thecytogenetic alterationdetectedinthiscaseisdescribedinapproximately 20%ofallplasmacellneoplasms.2,3Thepresenceoft(11;14) (q13;q32) reflects the juxtaposition of the proto-oncogene
rev bras hematol hemoter. 2017;39(1):66–69
69
overallsurvival.2,12 However,theexpectedoverexpressionof cyclin D1 was not identified in the BM biopsy specimen, probablyduetoantigenretrieval problemsafterthe decal-cification ofthe sample. Additionally, the presence ofthis abnormalityinplasmacellneoplasmsisusuallyassociated withtheatypicalmorphologicappearanceofLPLreportedin 50%ofthecases.6Furthermore,lackofexpressionsofCD56 andCD117havebeenassociatedtoplasmacellmalignancies inpatientswitht(11;14), aspreviouslydescribed.9 Of inter-est,theMYD88L265Psomaticmutation,presentin>90%of patientswithLPL/Waldenström’smacroglobulinemiaandalso innon-IgMLPL,isusefultodifferentiatethesedisordersfrom MM,includingIgMsecretingmyeloma,andsomeotherB-cell malignancies.13Thisstudywasnotcarriedoutinthepresent casebecausethediagnosisofPCLwasquicklyconcludedby FC.Inconclusion,thepresentclinicalcaseillustratestherare presentationofPCLwithatypicalmorphologyandhighlights theimportance ofFCinthe differential diagnosis between PCLandLPL.Additionallyt(11;14)(q13;q32)byFISH,increased theinformationnotonlyaboutthediagnosis butaboutthe prognosis.
Conflict
of
interest
Theauthorsdeclarenoconflictofinterest.
r
e
f
e
r
e
n
c
e
s
1. MckennaRW,KyleRA,KuehlWM,GroganTM,HarrisNL, CouplandRW.Plasmacellneoplasms.In:SwerdlowSH, CampoE,HarrisNL,JaffeES,PileriSA,SteinH,etal.,editors. WHOclassificationoftumoursofhaematopoieticand lymphoidtissues.fourtheditionLion:IARC;2008.p.200–13.
2. FernándezdeLarreaC,KyleRA,DurieBG,LudwigH,Usmani S,VesoleDH,etal.Plasmacellleukemia:consensus statementondiagnosticrequirements,responsecriteriaand treatmentrecommendationsbytheInternationalMyeloma WorkingGroup.Leukemia.2013;27(4):780–91.
3.TiedemannRE,Gonzalez-PazN,KyleRA,Santana-DavilaR, Price-TroskaT,VanWierSA,etal.Geneticaberrationsand survivalinplasmacellleukemia.Leukemia.
2008;22(5):1044–52.
4.García-SanzR,OrfaoA,GonzálezM,TaberneroMD,BladéJ, MoroMJ,etal.Primaryplasmacellleukemia:clinical, immunophenotypic,DNAploidy,andcytogenetic characteristics.Blood.1999;93(3):1032–7.
5.RajaKR,KovarovaL,HajekR.Reviewofphenotypicmarkers usedinflowcytometricanalysisofMGUSandMM,and applicabilityofflowcytometryinotherplasmacelldisorders. BrJHaematol.2010;149(3):334–51.
6.FonsecaR,BloodEA,OkenMM,KyleRA,DewaldGW,Bailey RJ,etal.Myelomaandthet(11;14)(q13;q32);evidencefora biologicallydefineduniquesubsetofpatients.Blood. 2002;99(10):3735–41.
7.RawstronAC,OrfaoA,BeksacM,BezdickovaL,BrooimansRA, BumbeaH,etal.ReportoftheEuropeanMyelomaNetworkon multiparametricflowcytometryinmultiplemyelomaand relateddisorders.Haematologica.2008;93(3):431–8.
8.BatailleR,JégoG,RobillardN,Barillé-NionS,HarousseauJL, MoreauP,etal.Thephenotypeofnormal,reactiveand malignantplasmacells.Identificationofmanyandmultiple myelomasandofnewtargetsformyelomatherapy. Haematologica.2006;91(9):1234–40.
9.MateoG,MontalbánMA,VidrialesMB,LahuertaJJ,MateosMV, GutiérrezN,etal.Prognosticvalueofimmunophenotypingin multiplemyeloma:astudybythePETHEMA/GEMcooperative studygroupsonpatientsuniformlytreatedwithhigh-dose therapy.JClinOncol.2008;26(16):2737–44.
10.KonoplevS,MedeirosLJ,Bueso-RamosCE,JorgensenJL,LinP. Immunophenotypicprofileoflymphoplasmacytic
lymphoma/Waldenströmmacroglobulinemia.AmJClin
Pathol.2005;124(3):414–20.
11.PaivaB,GutiérrezNC,ChenX,VídrialesMB,MontalbánM, Rosi ˜nolL,etal.ClinicalsignificanceofCD81expressionby clonalplasmacellsinhigh-risksmolderingandsymptomatic multiplemyelomapatients.Leukemia.2012;26(8):1862–9.
12.RajkumarSV.Multiplemyeloma:2016updateondiagnosis, risk-stratification,andmanagement.AmJHematol. 2016;91(7):719–34.
13.TreonSP,XuL,YangG,ZhouY,LiuX,CaoY,etal.MYD88 L265PsomaticmutationinWaldenstrom’s