jcoloproctol(rioj).2017;37(4):328–331
w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Technical
Note
Double
single-port
transanal
pouch
surgery:
a
novel
technique
for
rectal
excision
and
ileo-anal
pouch
anastomosis
for
ulcerative
colitis
Janindra
Warusavitarne
a,
Paulo
Gustavo
Kotze
b,∗aSt.Mark’sHospital,DepartmentofColorectalSurgery,London,UnitedKingdom
bPontifíciaUniversidadeCatólicadoParaná(PUCPR),HospitalUniversitárioCajuru,UnidadedeCirurgiaColorretal,Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received15July2017 Accepted20July2017
Availableonline6September2017
Keywords:
Colitisulcerative Rectum
Minimallyinvasivesurgical procedures
a
b
s
t
r
a
c
t
Surgeryforileoanalpouchhasevolveddramaticallyoverthelast30years.Manyofthe advancesrelatetominimallyinvasiveapproachesthatnotonlyoffercosmeticbenefitsbut alsohaveadvantagesthatarewelldescribedintheliterature.Inthistechnicalnote,the authorsdescribethedoublesingle-porttransanalpouchoperation.Anabdominal single-portisusedfortotalcolectomy,atthesiteoftheileostomy.Atransanalsingle-portisused forthe‘bottom-up’rectalresection.Thetechnicalstepsandpotentialadvantagesofthe techniquearediscussedindetail.Doublesingle-porttransanalpouchsurgeryistechnically feasibleandcanhavesignificantbenefitsinulcerativecolitispatients.
©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Cirurgia
de
reservatório
ileal
com
duplo
single-port:
uma
nova
técnica
para
a
ressecc¸ão
retal
e
anastomose
ileo-anal
na
retocolite
ulcerativa
Palavras-chave:
Coliteulcerativa Reto
Procedimentoscirúrgicos minimamenteinvasivos
r
e
s
u
m
o
Acirurgiaparabolsaileoanalevoluiuexcepcionalmentenosúltimos30anos.Muitosdos avanc¸osreferem-seaabordagensminimamenteinvasivas,quenãosóoferecem benefí-ciosestéticos,mastambémsignificamvantagensjádevidamentedescritasnaliteratura. Nestanotatécnica,osautoresdescrevemaoperac¸ãodereservatórioilealtransanalcom duploacessoporsingle-port.Umportalúnicoabdominaléutilizadoparaacolectomiatotal, nolocaldaileostomia.Umsegundoportalúnicotransanaléusadoparaaressecc¸ãorectal
∗ Correspondingauthor.
E-mail:[email protected](P.G.Kotze).
http://dx.doi.org/10.1016/j.jcol.2017.07.005
jcoloproctol(rioj).2017;37(4):328–331
329
“debaixoparacima”.Asetapastécnicasepotenciaisvantagensdatécnicasãodiscutidas emdetalhes.Acirurgiadereservatórioilealtransanalcomduploacessoporportaúnicaé tecnicamenteviávelepoderepresentarbenefíciossignificativosempacientescomcolite ulcerativa.
©2017SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
Surgeryforileoanalpouchhasevolvedconsiderablyoverthe years.Minimally invasivetechniques have been the main-stayof recentdevelopments and low stapledanastomoses have been possible with the advent of advanced stapling devises.1,2 Thelatestadvanceinminimallyinvasivesurgery
isthetransanalrectalresection,andthistechniquehasbeen welldescribedinpouchsurgery.3
There are several potential advantagestothe transanal approach.Theadvantagesareprobablybestconferredinthe narrow male pelvis and in obese patients. This dissection laparoscopicallyisfrequently difficultand mayoften leads toconversion.Inaddition,thetechniqueavoidsmultiple sta-plerfiringsacrossthedistalrectumwhichcanincreasethe riskofanastomoticleak.4 Subsequentreinforcementofthe
anastomosisthroughtheanushasthetheoreticaladvantage offurtherreducingtheleakrate.
Currently,onlytechnicaldescriptionsandsmallcaseseries discussthefeasibilityandoutcomesofthetransanalpouch procedure.3,5,6 There are also different anal platforms that
canbeused:TEM(TransanalEndoscopicMicrosurgery,Richard Wolff,Germany),TEO(TransanalEndoscopicOperation,Karl Storz,Tuttlingen,Germany)ordetachablesingleportdevices. TEMandTEOarefixedplatformsthatcanmaketheprocedure challenginginsomecases.Detachabledevicesdonothave fix-ation,andallowthesurgeontohavebettertriangulationand comforttoperformtheprocedure.
The aim of this technical note is to describe in detail thesurgicalstepsofthedoublesingle-porttransanalpouch surgery,andtodiscusspossibleadvantagesofthetechnique.
Surgical
technique
Inthedoublesingle-portprocedure,aGelPointPort(Applied Medical,RanchoSantoMargarita,California)isplacedatthe ileostomysite, and a GelPoint Path (Applied Medical, Ran-cho Santo Margarita, California) is used for the transanal procedure.Inordertoestablishapneumoperitoneum,a sin-gleincision isperformedatthestomasite,generallyinthe right iliac fossa. If the patient had a previous colectomy withmucousfistula,thefistulawiththerectalstumpcanbe mobilisedandreleasedintotheabdominalcavity,afterwhich theGelPointisinserted.Thishasaring tosecureit tothe abdominalwallandalidthroughwhichportsareinserted.
TheGelPointdevicehasthreeworkingportsandastandard 10mm30◦ laparoscopiccamera(KarlStorz,Tuttlingen,
Ger-many)isused,whichcanbeinsertedintoanyoftheports.
Anadditional5mmportcanbeplacedintheleftiliacfossato allowbettertriangulationandretraction,ifnecessary.Thissite isusuallyusedtoplacethepelvicdrainattheendofthe proce-dure.Pneumoperitoneumisusuallymaintainedatapressure of12mmHg.
TherectaldissectioncanbecommencedintheTME(total mesorectalexcision)planeorthecloserectalapproachfrom theabdominalport.Thesuperiorrectalarteryisthendivided. Therectalphaseoftheoperationiscommencedconcurrently andapursestringsutureisplacedapproximately3–4cm prox-imaltothedentatelinewiththeaidofaLonestarretractor (CooperSurgical,Trumbull,USA).Theamountofrectalmucosa thatisleftbehindaftertheinitialdistalrectaldivisionisbased onthedegreeofproctitisandthepresenceorabsenceof dys-plasia. When dysplasiaisnot theindicationforsurgery or whenthedistalproctitisisnotsevere,a1–2cmrectalcuffis lefttoreducetheriskofstoolleakage.
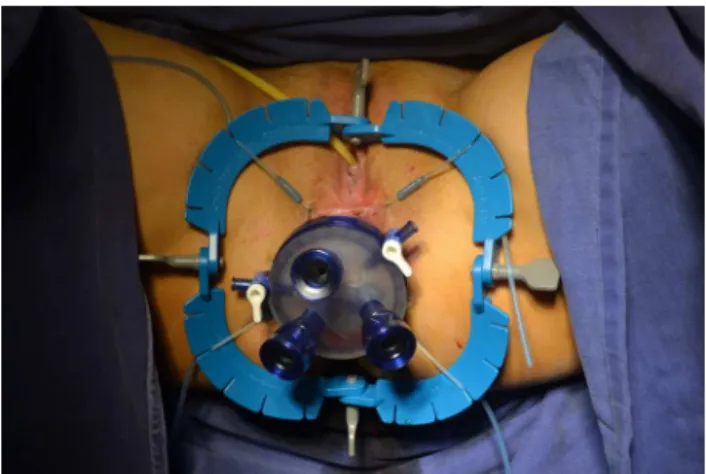
TheGelPointPathtransanaldeviceisplacedintheanal canal(Fig.1).Two standardportsare placedwithinthe gel followedbya12mmAirsealport(ConmedUSA).Airseal insuf-flationiscommencedat5mmHguntilthedeviceisactiveand thenincreasedto20mmHg.Thedissectionisstartedlaterally usingadiathermyhook.Weprefertouseahookratherthana harmonicscalpel,asithelpstoreducesmokeandfacilitates endoscopicviewing(Fig.2).Thecloserectaldissectionis con-tinuedsuchthattheabdominalandrectaloperatorsapproach themidrectumfromoppositedirections.Incaseswith associ-ateddysplasia,theTMEplanemustberespectedandfollowed. Duringthispartoftheprocedure,thetwooperatorscanassist eachothertoensuresafetyandadequateretraction(Fig.3). Simultaneousdissectionalsoreducestheoperationtimeand canmaketheoperationeasier.Oncetheproctectomyis com-pletedthespecimenisbroughtoutthroughthestomasite,or
330
jcoloproctol(rioj).2017;37(4):328–331Fig.2–Commencingthedissection.
Fig.3–Retractionanddissection,withcommunication withtheabdominalteam(sponge).
Fig.4–Transanalextractionofthespecimen.
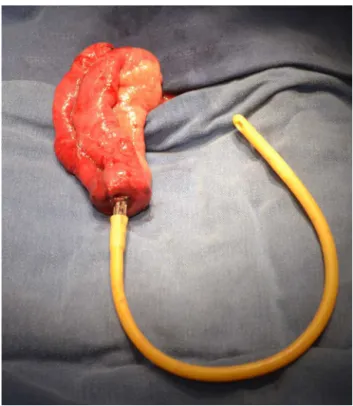
transanally(Fig.4).TheJ-pouchisthencreated,bystandard stapling,afterbringingtheileumoutthroughthestomasite, andtheanvilofthestaplingdeviceissuturedandconnectedto anextender,usuallyanumber18Foleycatheter(Fig.5).Afull thicknesspursestringsutureisthenplacedintheremaining rectalcuff.Werecommendastrong suturewith0prolene, thatallowsstrongtractionwithouttissuerupture.Thisisalso examinedtoensurethatthevaginaisnotincorporatedinthe females.Theanvilwithitsextender, asshowninFig.5, is placedinthepouchandtheproximalpursestringissecured. Thepouchisthenreturnedtotheperitonealcavity.The patientispositionedintherightsideuppositiontoensurethat
Fig.5–Pouchcreationatstomasite,extensorandanvil.
Fig.6–Staplinganastomosis.
tro-jcoloproctol(rioj).2017;37(4):328–331
331
carsite,andusuallyaloopileostomyismaturedinthesingle portsiteattherightlowerquadrant.
Comments
and
final
messages
Minimallyinvasivesurgeryforinflammatoryboweldiseases shouldbethe mainstay,notonlyforthe cosmetic benefits forthepredominantly youngpopulationbut alsoformany otherclinicalreasons.Minimallyinvasiveproceduresare rec-ommendedfortotalcolectomywithorwithout completion proctectomyintheEuropeanCrohn’sand Colitis Organisa-tion(ECCO)guidelines,owingtoreducedhospitalstay,faster returntonormalactivitiesandenhancedrecoverypathways.7
Single-portapproaches canalsobetechnically feasibleand performedinthisgroupofpatientsandtheadvantagessuch asreducedconversionratesandreducedpainrelief require-mentshaverecentlybeendescribed.
Therecanbetechnicaldifferencesbetweenthetransanal approachtorectalexcision betweenpatientswithlow rec-talcancerandulcerativecolitiswithoutdysplasia.Inpatients withcancer,thetransanaltotalmesorectalexcision(TaTME) istheapproachofchoice,withfullexcisionofthe mesorec-tumbasedonsoundoncologicprinciples.8Thistechniqueis
beingadoptedworldwideasanalternativetotheabdominal dissectionoftherectum,thatcanbesometimeschallenging andtimeconsuming.Inthemanagementofulcerative coli-tis,acloserectaldissectioncanbeperformed,ifthereareno signsofcancerordysplasiaintherectum.9,10Thisisdueto
thepossibilityofhavingsmallerpre-sacralsinusesincases ofileoanal anastomoticdehiscence.Oneprospectivestudy demonstratedthatthecloserectaldissectionwasassociated withlowercomplicationratesascomparedtoTME.9Onthis
basis,forbenigndiseaseswhererectalresectionisrequired closerectaldissectioncanberecommended.7
Acaseseriesincluding16patientswiththedouble single-portapproachforulcerativecolitiswasrecentlypublished.5
Theearlysurgicalcomplicationrate(upto30daysafterthe procedure),wasacceptableandcomparablewithother min-imallyinvasiveapproaches.BasedontheClavienandDindo classificationofcomplications,fourpatientshadgrade1,one patienthadgrade2andonepatienthadgrade3 complica-tion.Fivepatientshadminorcomplications(31.25%)andone patienthad ananastomoticleakage2weeksafterthe pro-cedure,and was considered tohavea majorcomplication. AllthecasesfromthisserieswereoperatedwiththeTaTME approach,andcloserectaldissectionwasnotperformed.
Insummary,doublesingleporttransanalpouchsurgeryis technicallyfeasibleandisaninterestingalternativeapproach for the surgical management of ulcerative colitis. This approachoffers the opportunityto performa pure laparo-scopicoperationinallpatientswhichhasthepotentialbenefit ofbetteroutcomesforpatientswhererectaldissectioncan bedifficultfromtheabdomen.Ifthisisextrapolatedbeyond theimmediatebenefitsoflaparoscopy,thetechniquehasthe potentialtoreducethe hybridprocedures wheretherectal
dissectionisperformedviaanabdominalincision.Thishas thepotentialtoimprovefertilityratesafterpouchsurgeryas thereducedfertilityratesaremostlydirectlyrelatedtopelvic adhesionsfromopensurgery.Moreprospectivestudies com-paringtheTaTMEapproachwiththecloserectaldissection can clarifythe best alternative forpatients withulcerative colitis.Combiningthetransanalapproachwithanabdominal single-portresultsinbettercosmesisandlesssurgicaltrauma, withfasterrecovery.Moreprospectivestudiesarewarranted inordertofirmlydemonstratethebenefitsofthisprocedure andplaceitasaprocedureofchoiceforIPAA.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BachSP,MortensenNJ.Revolutionandevolution:30yearsof ileoanalpouchsurgery.InflammBowelDis.2006;12:131–45.
2.BaekSJ,DozoisEJ,MathisKL,LightnerAL,BoostromSY,Cima RR,etal.Safety,feasibility,andshort-termoutcomesin588 patientsundergoingminimallyinvasiveilealpouch-anal anastomosis:asingle-institutionexperience.Tech Coloproctol.2016;20:369–74.
3.deBuckvanOverstraetenA,WolthuisAM,D’HooreA. Transanalcompletionproctectomyaftertotalcolectomyand ilealpouch-analanastomosisforulcerativecolitis:amodified singlestapledtechnique.ColorectalDis.2016;18:O141–4.
4.RoumenRM,RahusenFT,WijnenMH,CroisetvanUchelen FA.“Dogear”formationafterdouble-stapledlowanterior resectionasariskfactorforanastomoticdisruption.Dis ColonRectum.2000;43:522–5.
5.LeoCA,SamaranayakeS,Perry-WoodfordZL,VitoneL,FaizO, HodgkinsonJD,etal.Initialexperienceofrestorative proctocolectomyforulcerativecolitisbytransanaltotal mesorectalrectalexcisionandsingle-incisionabdominal laparoscopicsurgery.ColorectalDis.2016;18:1162–6.
6.CoffeyJC,DillonMF,O’DriscollJS,FaulE.Transanaltotal mesocolicexcision(taTME)aspartofileoanalpouch formationinulcerativecolitis–firstreportofacase.IntJ ColorectalDis.2016;31:735–6.
7.ØreslandT,BemelmanWA,SampietroGM,SpinelliA, WindsorA,FerranteM,etal.EuropeanCrohn’sandColitis Organisation(ECCO).Europeanevidencebasedconsensuson surgeryforulcerativecolitis.JCrohnsColitis.2015;9:4–25.
8.WolthuisAM,BislenghiG,deBuckvanOverstraetenA, D’HooreA.Transanaltotalmesorectalexcision:towards standardizationoftechnique.WorldJGastroenterol. 2015;21:12686–95.
9.BartelsSA,GardenbroekTJ,AartsM,PonsioenCY,TanisPJ, BuskensCJ,etal.Short-termmorbidityandqualityoflife fromarandomizedclinicaltrialofcloserectaldissectionand totalmesorectalexcisioninilealpouch-analanastomosis.Br JSurg.2015;102:281–7.