w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Results
of
surgical
treatment
of
colorectal
cancer
in
nonagenarian
patients
Arthur
Manoel
Braga
de
Albuquerque
Gomes
∗,
Fábio
Lopes
de
Queiroz,
Rodrigo
de
Almeida
Paiva
HospitalFelícioRocho,BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received9May2017 Accepted12July2017
Availableonline12August2017
Keywords:
Colorectalcancer Surgery
Nonagenarian Morbidity Mortality
a
b
s
t
r
a
c
t
Purpose:Theobjectiveofthepresentstudywastocomparetheresultsofsurgicaltreatment ofnonagenarianpatientshavingcolorectalcancerwithpatientsyoungerthan90years.
Methods:A total of622patientswho underwent curativesurgery wereincludedin the presentstudy.Thedatabaseofthesurgicalservice,intheperiodfrom2007to2013,was usedtoobtainthesample.Thisisadescriptive,retrospectivestudythatcomparedthe pro-filesof17nonagenarianpatients(GroupI)with605patientsyoungerthan90years(Group II).Thegroupswerecomparedregardingsurgicalcomplications,lengthofhospitalstay,type ofsurgeryperformedandASAclassification.
Results:Themeanagebetweenthegroupswas92.2yearsand61.2years.Themeanlength ofhospitalstayinGroupsIandIIwas17.3daysand8.75days,respectively.Thesurgery performedmostfrequentlywastherightcolectomy,inbothgroups.Themostcommon postoperativecomplicationwassepsis(11.8%)amongthenonagenarians,andparalyticileus (4.5%)amongthoseyoungerthan90years.Laparoscopicsurgerywasperformedon5out ofatotalof17patientsevaluatedinGroupI.Amongthethreemortalitiesregisteredinthis lattergroup,twowereclassifiedasASAIIIandonlyoneasASAI.
Conclusion: Theresultsindicatethatcolorectalsurgerymaybeperformedinthisgroup,with acceptablemorbidityandmortalityrates,inpatientswithlowpreoperativerisk(ASAI/II).
©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Resultados
do
tratamento
cirúrgico
do
câncer
colorretal
em
pacientes
nonagenários
Palavras-chave:
Câncercolorretal Cirurgia
r
e
s
u
m
o
Finalidade:Oobjetivodopresenteestudofoicompararosresultadosdotratamentocirúrgico depacientesnonagenáriosportadoresdecâncercolorretalversuspacientescommenosde 90anos.
∗ Correspondingauthor.
E-mail:[email protected](A.M.Gomes). http://dx.doi.org/10.1016/j.jcol.2017.07.002
Nonagenário Morbidade Mortalidade
Métodos: Oestudoenvolveu622pacientesqueforamsubmetidosàcirurgiacurativa.Para obtenc¸ãodaamostra,utilizamosobancodedadosdoservic¸odecirurgia,abrangendoo períodode2007-2013.Esteéumestudoretrospectivodescritivoquecomparouosperfisde 17pacientesnonagenários(GrupoI)versus605pacientescommenosde90anos(Grupo II).Osgruposforamcomparadosparacomplicac¸õescirúrgicas,durac¸ãodapermanênciano hospital,tipodecirurgiarealizadaeclassificac¸ãoASA.
Resultados: AmédiadeidadeparaosGruposIeIIfoi,respectivamente,92,2e61,2anos. Adurac¸ãomédiadepermanêncianohospitalnosGruposIeIIfoi,respectivamente,17,3 diase8,75dias.Acirurgiamaisfrequentementerealizadafoicolectomiadireita,nosdois grupos.Acomplicac¸ãopós-operatóriamaiscomumfoisepse(11,8%)entreosnonagenários, eíleoparalítico(4.5%)entreospacientescommenosde90anos.Cirurgialaparoscópicafoi realizadaem5pacientes,emumtotalde17pacientesavaliadosnoGrupoI.Considerando astrêsmortalidadesregistradasnesseúltimogrupo,duasforamclassificadascomoASAIII eapenasumacomoASAI.
Conclusão: Osresultadosobtidosindicamque,nessegrupo,acirurgiacolorretaléopc¸ão válida,compercentuaisaceitáveisdemorbidadeemortalidade,empacientescombaixo riscopré-operatório(ASAI/II).
©2017SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
Colorectalcancer(CRC)ismoreprevalentinpeopleaged65 ormoreanditsincidenceincreaseswithage.Consideringthe increaseinlifeexpectancyofthepopulation,accordingtodata providedbytheWorldHealthOrganization,thediagnosisof CRCintheelderlyhasincreasedconcomitantly.Alower physi-ologicalreservetoaddresshomeostasisimbalances,whether incardiovascular,metabolicorrespiratoryareas,associated withamuchgreatercoexistenceofcomorbidities,makesthis agegroupmoresubjecttocomplications.Thus,thebenefitof surgeryandanesthesiamustbecarefullyevaluated,aswell as the prognosis and survivalrates. Cancerin this elderly populationisanethicaldilemma forsurgeonsand oncolo-gistsregardingthedecisionabouttheaggressivenessofthe treatment,balancingthebenefitofsurgeryandtheincrease ofassociatedrisks,inanagegroupwithshortexpectancyof survival.1
Therearefewavailablestudiesonthepostoperativeresults ofsurgicaltreatmentofcolorectalcancerinpatientsover90 yearsormore,bothofthelaparoscopicandtheconventional procedures.2
Ingeneral,therandomizedtrials,inthemedicalliterature, haveshownthatlaparoscopiccolorectalresectionforcancer hadsurvivalandrecurrenceratessimilartothoseshownin openresectionsurgery,butwithareductioninhospitalstay, postoperativepainandmorbidity.3
Theobjective of the present study wasto compare the resultsofsurgicaltreatmentinnonagenarianpatientswith colorectal cancer,with patients of less than 90 years. The little evidence available in the literature on the subject, associated with the fact that there is a predominance of articleswithsmall samples, confirmsthe relevanceofthis study.
Materials
and
methods
Thisisaretrospectiveanddescriptivestudy,with622patients with colorectal cancer, undergoing curative surgery in the periodfrom2007to2013.Theservicedatabasewasusedto obtainthesamplewhichcomparedtheprofileof17 nonage-narianpatients(GroupI)with605patientslessthan90years ofage(GroupII).Thegroupswereanalyzedastothe occur-renceofpostoperativecomplications,lengthofhospitalstay, thetypeofsurgeryperformedandtheASAclassification.The Clavien-Dindoclassificationwasalsousedtocategorize com-plicationsthatoccurred.
Thosewithoutindicationforemergencysurgery,withno history ofrecurrentcolorectal cancer,withnofixed, palpa-ble mass and without involvement of adjacent structures were consideredsuitable forthe laparoscopicapproach. All surgeonsinvolvedhadperformed20ormorecolorectal laparo-scopicsurgeriesandhadthenecessaryknowledgeregarding theprinciplesofcancersurgery.
StatisticalanalysiswasperformedusingStata(version9.1) and SPSS (version 20.0). Thelevel ofsignificancewas0.05. Thestatisticaltestsusedwere theasymptoticPearson Chi-square,tocomparegenderbetweenthegroups,andthetests ofproportionsforpostoperativecomplicationsandtypesof surgicaltechniques.TheMann–Whitneytestwasusedto com-parelengthofhospitalstay,andtheexactPearsonChi-square testwasusedtocompareASA.
Results
Table1–Levelofsignificanceaccordingtosex distribution.
Gender <90years
n(%)
>90years
n(%)
p-valuea
Female 314(51.8) 10(58.8) 0.568
Male 291(48.2) 7(41.2)
Total 605 17
a AsymptoticPearsonChi-squaredtest.
Table2–Age(years).
<90years >90years
Mean±SD 62.1±13.2 92.2±1.9
Median(Q1;Q3) 62.0(53.0;72.5) 92.0(91.0;93.5)
Table3–Lengthofhospitalstay(days).
<90years >90years p-valuea
Mean±SD 8.8±10.6 16.7±14.7 0.001
Median(Q1;Q3) 6.0(5.0;9.0) 9.0(7.0;27.0)
a Mann–Whitneytest.
theyoungestpatientwas20yearsoldandtheoldestwas89 (Table2).
ThemeanlengthsofhospitalstayinGroupIandinGroup II, considering only patients who received discharge, were 17.3daysand 8.75days, respectively.OnepatientinGroup I was admitted for 56 days due to several complications, suchasAMI,woundinfection,andbronchospasmcrises.The patient with the shortest hospital stay in this group was
6days (Table3). Comparing the same variable only inthe
nonagenariangroup,amongthoseundergoing laparoscopic orconventional procedures,demonstrated ashorter hospi-talstayinthosewithminimallyinvasiveaccess(5patients, 13days)inrelationtothosewithopensurgery(19.5days,12 patients),butwithp>0.05(Table4).
Table4–Lengthofhospitalstaybetweenopensurgery andlaparoscopyinGroupI.
GroupI Conventional
method
Laparascopic method
p-valuea
Time(days)/ patients
19.5d/12p 13d/5p 0.599
Median(Q1;Q3) 9.5(7.0;28.3) 7.5(6.0;22.5) Mean±SD 16.50±16.55 12.00±10.10
a Mann–Whitneytest.
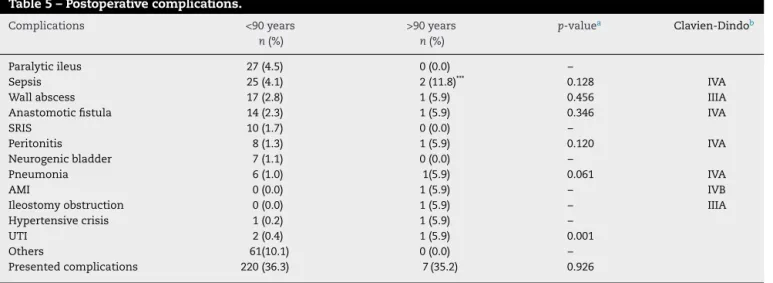
GroupIhadcomplicationsin36.2%ofthecases,withthree mortalities,whileGroupIIhadcomplicationsin36.3%ofthe sample.SepsiswasthemostprevalentcomplicationinGroup I(2cases);onewasofpulmonaryetiologyandtheotherdue toananastomoticfistula.Inthelatter,therewasnoevidence ofeventssuchasparalyticileus,SRISandneurogenic blad-der.InGroupII,paralyticileuswasmoreprevalent(27cases). Evaluatingstatisticalsignificance,theonlyvariablethat pre-sentedp<0.05wastheurinarytractinfection(5.9%and0.4%,
p=0.001)(Table5).
Nostatisticaldifferencewasfoundwhenthemostsevere complicationssuchassepsis,anastomotic fistulaand peri-tonitiswereanalyzedseparately.However,whenthesewere puttogetherforbetween-groupscomparison(Clavien-Dindo IIIandIV),adifferenceofp<0.05wasfound,denoting pre-dominanceoftheseadversitiesinGroupI(Table6).
Regarding theASAclassification,therewas asignificant differenceatthe0.05level.Thegroupover90hasmoreASAIII andIVthanthegroupyoungerthan90.Amongthe17patients inGroupI,fourwereASAI,sevenASAII,fiveASAIIIandone ASAIV.Examiningtherateofcomplications,onlythose iden-tifiedasASAIIIappearedmorefrequentlyinGroupIthanin GroupII,withp<0.05(Tables7and8).
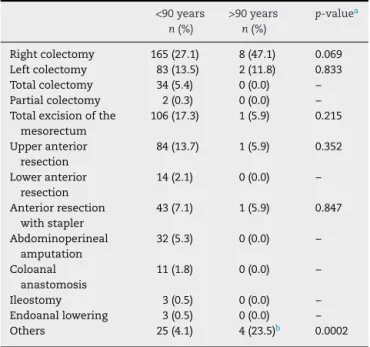
Regardingtypeofsurgery,therightcolectomywasthemost frequently performed procedure in both groups (p=0.069), followed by left colectomy (p=0.833) and total mesorectal
Table5–Postoperativecomplications.
Complications <90years
n(%)
>90years
n(%)
p-valuea Clavien-Dindob
Paralyticileus 27(4.5) 0(0.0) –
Sepsis 25(4.1) 2(11.8)*** 0.128 IVA
Wallabscess 17(2.8) 1(5.9) 0.456 IIIA
Anastomoticfistula 14(2.3) 1(5.9) 0.346 IVA
SRIS 10(1.7) 0(0.0) –
Peritonitis 8(1.3) 1(5.9) 0.120 IVA
Neurogenicbladder 7(1.1) 0(0.0) –
Pneumonia 6(1.0) 1(5.9) 0.061 IVA
AMI 0(0.0) 1(5.9) – IVB
Ileostomyobstruction 0(0.0) 1(5.9) – IIIA
Hypertensivecrisis 1(0.2) 1(5.9) –
UTI 2(0.4) 1(5.9) 0.001
Others 61(10.1) 0(0.0) –
Presentedcomplications 220(36.3) 7(35.2) 0.926
SIRS,systemicinflammatoryresponsesyndrome;AMI,acutemyocardialinfarction;UTI,urinarytractinfection. a Z-testforcomparisonofproportions.
Table6–Criticalcomplications,accordingto Clavien-Dindoclassification.
Clavien-Dindo GroupI GroupII p-valuea
III 2/17(11.76) 17/605(2.81) 0.0344
IV 6/17(35.29) 53/605(8.76) 0.0002
a Z-testforcomparisonofproportions.
Table7–ASAclassification.
<90years
n(%)
≥90years
n(%)
p-valuea
I 290(47.9)* 4(23.5)* 0.013
II 259(42.8) 7(41.2)
III 51(8.4)* 5(29.4)*
IV 5(0.8)* 1(5.9)*
a ExactPearsonChi-squaredtest.
Table8–Comparisonoftheindexofcomplications accordingtoASAclassification.
Indexofcomplications <90years >90years p-valuea
ASAI 74/605(12.23) 1/17(5.88) 0.428
ASAII 73/605(12.07) 2/17(11.76) 0.969 ASAIII 14/605(2.31) 3/17(17.65) 0.0001
ASAIV 3/605(0.50) 0(0.00) –
a Z-testforcomparisonofproportions.
Table9–Typeofsurgicaltechniqueperformed.
<90years
n(%)
>90years
n(%)
p-valuea
Rightcolectomy 165(27.1) 8(47.1) 0.069 Leftcolectomy 83(13.5) 2(11.8) 0.833
Totalcolectomy 34(5.4) 0(0.0) –
Partialcolectomy 2(0.3) 0(0.0) –
Totalexcisionofthe mesorectum
106(17.3) 1(5.9) 0.215
Upperanterior resection
84(13.7) 1(5.9) 0.352
Loweranterior resection
14(2.1) 0(0.0) –
Anteriorresection withstapler
43(7.1) 1(5.9) 0.847
Abdominoperineal amputation
32(5.3) 0(0.0) –
Coloanal anastomosis
11(1.8) 0(0.0) –
Ileostomy 3(0.5) 0(0.0) –
Endoanallowering 3(0.5) 0(0.0) –
Others 25(4.1) 4(23.5)b 0.0002
a Z-testforcomparisonofproportions.
b ThreeHartmannsurgeriesandarectosigmoidectomy.
excision (p=0.215). In Group I, 5 of the 17 nonagenarians underwent laparoscopy. There was statistical significance forbothHartmannandrectosigmoidectomysurgeries(23.5% and4.1%,p=0.0002),analyzingGroupsIandII,respectively (Table9).
Discussion
Elderly patientsclearlyhavea higherprevalenceof comor-bidities.Theriskinherentinsurgeryisdirectlyrelatedtothe numberofconcurrentdiseasesandtothepatient’s physiolog-icalreserve.2Thefactthatcolorectalcanceristhethirdmost
diagnosedintheworld,associatedwiththeagingtrendofthe population,leadstotheincreasinglyfrequentdiagnosisofthis disease.4
In a randomized, prospective study, the applicability of laparoscopic colorectalsurgery wasevaluated in16 elderly patients, with 9being 90 years or older and 7between 80 and89years.Inthistrial,therewerenostatistically signifi-cantdifferencesastotheanesthetic-surgicalrisk(ASAscore), postoperative morbidity,surgical time,blood lossand time requiredtoresumeoralintake.Therewasnoneedfor conver-siontoopensurgeryandnopatientdiedaftertheintervention. Allpostoperativecomplicationsweretreatedbyconservative methods,includingananastomoticfistulaintheoctogenarian group.2
In our study, 5 ofthe 17 nonagenarian patients under-wentthelaparoscopicapproachwithnoneedforconversion. Moreover,astherewerenostatisticallysignificantdifferences regarding most complications when evaluated separately, postoperative morbidity might notbe aparameter to con-traindicatesurgeryintheover-90population.However,itis worthrememberingthatintheanalysisofthewhole,ofthe mostseverecomplicationswithrespecttotheClavien-Dindo classification,GroupIprevailedwithp<0.05.
Inaretrospectivestudy,289patientsbetween80and 95 years were evaluated. 150 patients underwent the laparo-scopic approach and 139 underwent open surgery, with colorectalcancerasthemostcommonindication.Thegroup thatunderwentopensurgeryshowedthegreaternumberof mortalities,longerhospitalstays,higherincidenceofparalytic ileusandincreasedmorbidity,withallthosevariables show-ingp<0.05.Thesedatasuggestthatlaparoscopiccolectomy maybeapreferableoptionfortheelderly,includingpatients over90.5,6
SimilarresultswerepublishedbyChaudharyetal., high-lighting thefactthatthelaparoscopicapproachshouldnot becontraindicatedforcolorectalcancerpatientsbasedonly onage,and thatelectivesurgeryintheelderlyissafewith acceptableratesofmorbidityandmortality.3,7,8
Another retrospective series, examined short-and long-term results in44 nonagenarianpatients havingcolorectal cancer whounderwent electiveor emergencysurgery.This series, in agreement with the present study, shows that femalesprevailedwith10/17cases.Thisresult,however,was withoutstatisticalsignificance(p=0.568).Thepredominance (48/74)wasattributedtothegreaterlifeexpectancyamong women.
rateforelectivesurgeries(12%vs17.6%)werelowerthanin thepresentstudy.1Inthelatter,onepatientfromGroupIwas
admittedfor56daysduetovariouspostoperative complica-tions.
Consequently,tothedetrimentofstatisticallysignificant evidenceastothegreaterlengthofhospitalstayinthe nona-genariangroup,suchhospitalstaywasnotaccompaniedbya higherrateofcomplications.Thissuggests,therefore,thatthis variablecannotbeadoptedasaparameterthat contraindi-catesthesurgicalapproachinthispopulation,asreportedby Roscioetal.9,10
Also in this context, due to the trend toward shorter hospitalstaysamongthoseundergoinglaparoscopy,the nona-genariangroupisrelatedtolowerhospitalcostscomparedto thosewithinthesame age rangeundergoingopensurgery, accordingtothereportofBottinoetal.11
Moreover,ofthethreemortalitiesreportedinGroupI,two wereclassifiedasASAIIIandonlyonewasclassifiedasASAI. Itisworthnotingthat,comparingtheprevalenceof complica-tionsaccordingtoASAclassification,therewaspredominance onlyamongASAIIIpatientsinGroupI.Therefore, consider-ingthefactthatthegreaternumberofASAIIIandIVpatients inGroupIwasstatisticallysignificant,thismakesASAa rea-sonabledeviceforpredictingtheresultsandevaluatingthe applicabilityornotofsurgicalinterventioninthesepatients. ThisissimilartotheresultsdescribedbyJeongetal.12Inthis
latterstudy,aninterestingaccountwasgivenofthe laparo-scopicpostoperativesuccessofa102-year-oldpatient with colorectalcancer.
Another descriptive, retrospective study, that compared the profile of 52 octogenarian patients (Group I) with 386 patientsyoungerthan80years(GroupII),from2007to2011, foundanaveragelengthofhospitalstayequalto9.3daysand arateofpostoperativecomplicationsof28.84%inthegroupof octogenarians.4Thus,accordingtothesedata,itwasobserved
that nonagenarianshave a hospital stay (17.3 days)and a postoperativecomplicationrate(36.2%)higherthan octoge-narians. Theright colectomy was also the most prevalent surgeryandsepsisthemostcommonpostoperative complica-tioninthegroupdescribed,aswiththenonagenariansample evaluatedhere.
Regardingcolorectalcancer,theincreasedagewas associ-atedwithdecreasedspecificsurvivalandthisdifferencewas relatedtoadecreaseintheuseofradicalsurgery.However, studies haveshown that the5-year survivalrate hasbeen equalamongbothelderlyandyoungpatientswhenthe appro-priatesurgicaltreatmentisperformed.So,wheneverpossible, surgeryshouldbeofferedasthefirsttreatmentofchoiceto elderlypatientswithcolorectalcancer.13
The non-randomized and retrospective nature of the presentstudywereconsideredlimitingfactorsofthiswork, openingthepossibility forbiasintheselectionofpatients between the two groups. The data analyzed showed that nonagenarian patients present no greater rate of compli-cation,whencompared withyoungerpatients. Thisshows that advanced age, in and of itself, should not be a rea-son to contraindicate surgery for the elderly, unless their
clinicalconditionandphysiologicalparametersdonotpermit largeresections.However,theyspendmoretimehospitalized, resultinginhigherhospitalcosts.Allresultsindicatethat colo-rectalsurgerycanbeperformedinthisgroupwithacceptable rates ofmorbidity and mortalityin patients withlow pre-operativerisk(ASAI/II).Theclinicallysignificantadvantages of laparoscopic surgery, according to the evidence already largely consolidated in the literature, havesocial and eco-nomicimplicationsinanagingsociety,justifyingthereturn ofthesepatientstoaproductivelifeinatimelymanner.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.ArenalJ,TinocoC,LabargaF,MartínezR,GonzaloM. Colorectalcancerinnonagenarians.ColorectalDis. 2012;14:44–7.
2.SomaT,SuganoM,KawasakiC,TsujiM,FukuiI.Colorectal resectioninnonagenarians:effectivenessoflaparoscopic surgery.AsianJEndoscSurg.2014;7:222–6.
3.ChaudharyB,ShabbirJ,GriffithJ,ParvaizA,GreensladeG, DixonA.Short-termoutcomefollowingelectivelaparoscopic colorectalresectioninoctogenariansenonagenarians. ColorectalDis.2012;14:727–30.
4.OliveiraFH,LacerdaFilhoA,QueirozFL,LaumonierPCC, CastilhoBA,RabeloFEF,etal.Feasibilityofsurgicaltreatment ofoctogenarianspatientswithcolorectalcancer.J
Coloproctol.2013;33:131–4.
5.ArveuxI,BoutronMC,ElMriniT,ArveuxP,LiabeufA, PfitzenmeyerP,etal.Coloncancerintheelderly:evidencefor majorimprovementsinhealthcareandsurvival.BrJCancer. 1997;76:963–7.
6.KurianA,SuryadevaraS,VaughnD,ZebleyD,HofmannM, KimS,etal.Laparoscopiccolectomyinoctogenariansand nonagenarians:apreferableoptiontoopensurgery?JSurg Educ.2010;67:161–6.
7.MutchM.Laparoscopiccolectomyintheelderly:whenistoo old?ClinColonRectalSurg.2006;19:33–9.
8.HoblerK.Colonsurgeryforcancerintheveryelderly.Cost and3-yearsurvival.AnnSurg.1986;203:129–31.
9.XieM,QinH,LuoQ,HeX,LanP,LianL.Laparoscopic colorectalresectioninoctogenarianpatients:isitsafe?A systematicreviewandmeta-analysis.Medicine(Baltimore). 2015;94:e1765.
10.RoscioF,BertoglioC,DeLucaA,FrigerioA,GalliF,Scandroglio I.Outcomesoflaparoscopicsurgeryforcolorectalcancerin elderlypatients.JSLS.2011;15:315–21.
11.BottinoV,EspositoMG,MottolaA,MarteG,DiMaioV,Sciascia V,etal.Earlyoutcomesofcolonlaparoscopicresectioninthe elderlypatientscomparedwiththeyounger.BMCSurg. 2012;12Suppl.1:s8.
12.JeongD,HurH,MinB,BaikS,KimN.Safetyandfeasibilityof alaparoscopiccolorectalcancerresectioninelderlypatients. AnnColoproctol.2013;29:22–7.