w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Postoperative
complication
rates
between
Crohn’s
disease
and
Colorectal
cancer
patients
after
ileocolic
resections:
a
comparative
study
夽
Larissa
Boaron
a,
Luiza
Facchin
a,
Mariella
Bau
a,
Patricia
Zacharias
a,
Diogo
Ribeiro
a,
Eron
Fábio
Miranda
a,
Ivan
Folchini
de
Barcelos
a,
Renato
Vismara
Ropelato
a,
Álvaro
Steckert
Filho
b,
José
Donizeti
de
Meira
Junior
c,
Ligia
Sassaki
c,
Rogério
Saad-Hossne
c,
Paulo
Gustavo
Kotze
a,∗aPontifíciaUniversidadeCatólicadoParaná(PUCPR),HospitalUniversitárioCajuru,Servic¸odeColoproctologia(SeCoHUC),Curitiba,PR,
Brazil
bGastroMedicalCenter,Florianópolis,SC,Brazil
cUniversidadeEstadualPaulista(UNESP),AmbulatóriodeDoenc¸asInflamatóriasIntestinais,Botucatu,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received13June2017 Accepted17July2017
Availableonline12August2017
Keywords: Crohn’sdisease Colorectalcancer Complication Postoperative
a
b
s
t
r
a
c
t
Introduction:Ileocolicresection(ICR)isthemostcommonsurgicalprocedureperformedfor Crohn’sdisease(CD).Similarly,right-sidedColorectalcancer(CRC)istreatedbythesame operation.Theprimaryaimofthisstudywastoanalyzeandcomparethefrequencyand profileofearlypostoperativecomplicationsofICRbetweenpatientswithCDandCRC. Methods:RetrospectiveandobservationalstudywithpatientssubmittedtoICRfromtwo Braziliantertiaryreferralunitsincolorectalsurgery.Weincludedpatientswith diagno-sisofCDorCRC,treatedwithICR,atanystageoffollow-up.Variablesanalyzed:ageat surgery,gender,diagnosis, surgicalapproach (open or laparoscopy),typeof anastomo-sis(hand-sewn/stapled;end-to-end/side-to-side),presenceandtypeofearlypostoperative complications(30days)andmortality,amongothers.
Results:109patientswereincluded,73withCD(67%)and36withCRC(33%).CDpatientswere younger(42.44±12.73yearsvs.66.14±11.02yearsintheCRCgroups,p<0.0001)andhad morepreviousresections(20±27.4inCDand0inCCR,p=0.001).Therewerenosignificant differencesbetweenthegroupsintermsofoverallearlypostoperativecomplications[17/73 (23.3%)intheCDand5/36(13.9%)intheCRCgroups(p=0.250)].Therewasnosignificant differencebetweenthegroupsinrelationtoanastomoticleakage(p=0.185),surgicalsite infections(p=0.883),othercomplications(0.829)anddeaths(p=0.069).
夽
StudiedcarriedoutatPontifíciaUniversidadeCatólicadoParaná(PUCPR),HospitalUniversitárioCajuru,Servic¸odeColoproctologia (SeCoHUC),Curitiba,PR,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](P.G.Kotze). http://dx.doi.org/10.1016/j.jcol.2017.07.004
Conclusions: Therewasnosignificantdifferenceinearlypostoperativecomplicationsin patientswithCDorCRCsubmittedtoICR.
©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.Thisis anopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Complicac¸ões
pós-operatórias
após
ressecc¸ões
ileocólicas
na
doenc¸a
de
Crohn
e
no
câncer
colorretal:
um
estudo
comparativo
Palavras-chave: Doenc¸adeCrohn Câncercolorretal Complicac¸ões Pós-operatório
r
e
s
u
m
o
Introduc¸ão: Aileocolectomiadireita(ICD)éaoperac¸ãomaisrealizadanomanejocirúrgico dadoenc¸adeCrohn(DC).Damesmaforma,éoprocedimentodeescolhanotratamentodo câncercolorretal(CCR)quandolocalizadoàdireita.Oobjetivodesteestudofoianalisare compararascomplicac¸õescirúrgicasempacientessubmetidosaICDporDCeCCRemuma coortedepacientes.
Método: Estudolongitudinal,retrospectivoeobservacional,deumacoortedepacientes submetidosaICDprovenientesde2centrosdereferênciaemcoloproctologia.Oscritérios deinclusãoforampacientescomDCouCCR,submetidosaICD,emqualquerestágiode acompanhamento.Asvariáveis analisadasforam: idadeà cirurgia,gênero, diagnóstico, abordagem(abertaoulaparoscópica),tipodeanastomose,presenc¸aetipodecomplicac¸ões pós-operatóriasprecoces(até30dias)eóbito.
Resultados: Foram incluidos 109 pacientes,73 comDC (67%) e 36 com CCR(33%). Os gruposforamhomogêneos em todasas variáveis,à excec¸ãoda idade (42,44±12,73na DCe66,14±11,02noCCR,p<0,0001).Nãohouvediferenc¸aentreosgruposemrelac¸ão àscomplicac¸õesprecoces,com17/67(23,3%)naDCe5/36(13,9%)noCCR,p=0,250.Da mesmaforma,nãohouvediferenc¸aentreosgruposemrelac¸ãoadeiscênciade anasto-mose(p=0,185),infecc¸õesdosítiocirúrgico(p=0,883),outrascomplicac¸ões(0,829)eóbitos (p=0,069).
Conclusões: Nãohouvediferenc¸anascomplicac¸õespós-operatóriasempacientes submeti-dosaICDentreportadoresdeDCeCCR.
©2017SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
Crohn’s disease (CD) is a systemic autoimmune chronic inflammationthataffectsthegastrointestinaltract,with cres-centincidenceandprevalenceindevelopingcountries.1This
diseasecan affectany portion ofthegastrointestinal tract. However,itismorefrequent(50%)intheterminalileumand caecum.1–3
StrategiesaimingdiseasecontrolinCDmanagementare evolving, mostly basedon novel therapeuticdrugs, as bio-logical agents (monoclonal antibodies). Despite significant advancesinmedicalmanagementofCD,surgeryisstill nec-essaryinasignificantproportionofpatients.4Upto50%of
patientsaresubmittedtoanintestinalresectionafter10years ofdiagnosis.5
ThemostcommonperformedsurgicalprocedureforCD istheileocolicresection(ICR),thatcanbeeitherperformed withminimallyinvasive techniques(multiportlaparoscopy, single-portorrobotics)orbyconventionalapproach.2,3 This
operationcanoftenbechallenging.Thesignificant inflamma-toryprocesscausedbyfailuretomedicaltherapymayresult incomplicationsasabscesses,fistulasandadhesions,what
cantechnically leadtodifficultiesinthesurgicalapproach. Thesedifficultiesusuallytendtoincreasesurgical postopera-tivecomplicationrates.2,6
Colorectal cancer (CRC), when located in the cecum, ascendingorproximaltransversecolon(rightsegmentsofthe largebowel),isusuallytreatedbythesamesurgicalmethod (ICR). Similarly, this operationin the management of CRC canbeperformedbyopenapproach,orbyminimally inva-sivetechniques.7Someoncologicalprinciplesmaybedifferent
betweencancerandCD,buttheoperationsperseare consid-eredsimilarinthemanagementofbothdiseases.6,7
PatientssubmittedtoICRmaypresentnumerous postop-erativecomplications.Minorones,suchasfever,surgicalsite and urinary tract infections canusuallybemanaged with-outsignificantproblems.However,majorcomplicationssuch asanastomotic leakage,sepsisand pneumoniacanleadto prolonged hospitalization or even to death.8,9 These
com-plications canbe aresult ofmany variables:patient’s age, smoking habits, previous use of certain types of medica-tion,othercomorbidities,surgicalcharacteristics(electiveor emergency),diseasephenotype(fistulas,stenosis,abscesses), typeoftheanastomosis,amongothers.6–11Multiport
complicationrates,asitensuredabetterpatientsatisfaction andshorterhospitalstayinthepostoperativeperiod,as com-paredtotheconventionalapproach.7–11
Duetothegreatercomplexityofthecases,asbig inflam-matory masses, internal, external fistulas and phlegmons can be a consequence of uncontrolled inflammation, it is speculatedthatpatientswithCD maypresent higherrates ofpostoperativecomplicationsincomparisontoother diag-noses,duetointraoperativetechnicaldifficulties.6,7Thiscan
also be related to associated medical therapy, leading to immunosuppressionatthetimeofsurgery.8,9 However,this
wasnotconfirmedintheliterature.AstudyfromtheUnited Stateswithmorethan700patientsdemonstratedthatdespite associatedimmunomodulatorsand biologics, postoperative complicationrateswerenothigherinICRforCDin compari-sontootherdiagnoses.6
Theprimaryaimofthis studywastoanalyzeand com-parethefrequencyandprofileofearlypostoperativesurgical complicationsofICRbetweenpatientswithCDandCRC.
Methods
Studydesign
Thiswasalongitudinal,retrospectiveandobservationalstudy withpatients submitted to ICRfrom twoBrazilian tertiary referralunitsincolorectalsurgery,ina5-yearperiod(between Januaryof2011andApril2016).
Inclusionandexclusioncriteria
TheeligibilitycriteriawerepatientswithdiagnosisofCDor CRC,confirmedbyimagingandendoscopictests,treatedwith ICR,byconventionalorlaparoscopicapproach(withprimary anastomosis)atany stageoffollow up.Patientswithother diagnosisexceptfromCDandCRC,orsubmittedtoother sur-gicalprocedures,thosewho wereyoungerthan18 yearsof age,withdivertingstomas,wholostfollow-uporhadlackof datainthechartswereautomaticallyexcluded.
Variablesofinterest
Concurrentlywithdatacollection,comparativeExcelcharts were created embracing patient’s name and other demo-graphic characteristics, such as age at surgery, gender, diagnosis, surgical approach (open or laparoscopy), type ofanastomosis(hand-sewn/stapled;end-to-end/side-to-side), presenceand typeofearly postoperativecomplications(30 days)andmortality,amongothers.
Groupdefinition
Afterinitialidentificationintheunits’operatinglists,patients hadtheirrecordsaccessed,andwereallocatedintotwogroups (CDand CRC).Earlypostoperative complicationswerethen analyzed(accordingtothefrequencyandtypeof complica-tion)andcomparedbetweenthetwogroups.
Statisticalanalysis
Pearsonchi-squaretestandMann–Whitney’sUtestwereused toverifygrouphomogeneity.Thestudent’sttestwasusedto comparethecomplicationratesbetweenthegroups.p<0.05 valueswereconsideredsignificant.
Ethicalconsiderations
Thestudyprotocolwasapprovedbytheethicscommitteeof theCatholicUniversityofParaná(PUCPR),inJune/2016,under protocolnumberCAAE56444216.7.0000.0020,attheministry ofhealthplataformabrasilwebsite.
Results
Initially, 118patientswereidentifiedfromthesurgicallists, andconsideredeligibleforthestudy.Fourpatientswere sub-sequentlyexcludedforlackofdatainthechartsandfivewere alsoexcludedduetodivertingstomas,asaresultofthe proce-dure.Therefore,thestudy’spopulationwascomposedby109 patients(Fig.1):73withCD(67%)and36withCRC(33%).
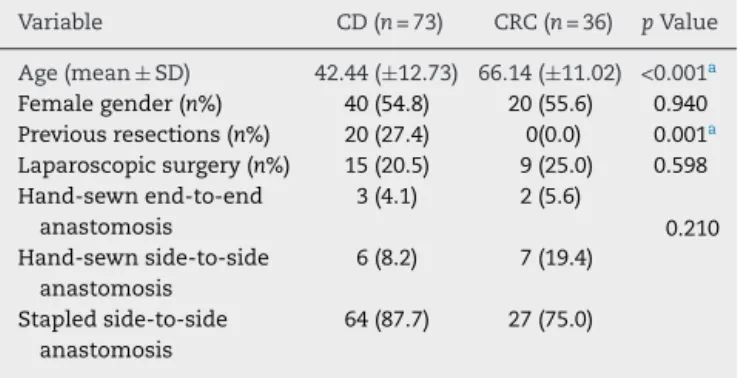
Table 1demonstratesthe baselinecharacteristics ofthe patients in detail. As observed, the groups were not 100% homogeneous.Therewasadifferenceinthemedianageat surgery(42.44±12.73intheCDand66.14±11.02intheCRC groups,p<0.0001)andinthenumberofpreviousresections (20±27.4inCDand0inCCR,p=0.001).Thesurgical charac-teristicsofthe patients werealsocomparablebetween the groups.Laparoscopicprocedureswereperformedin20–25% of thepatients, and the stapled side-to-side wasthe most frequentanastomosisperformed.Allpatientswithdiagnosis ofCDwereusingoranimmunomodulator(azathioprine),a biologicalagent,orbothincombination.
Initially selected n=118
CRC n=36 CD n=73 Excluded:
Lack of data (n=4) Stomas (n=5)
Fig.1–Studyflowchartandgroupdefinition.
Table1–Baselinecharacteristicsofthe109patients.
Variable CD(n=73) CRC(n=36) pValue
Age(mean±SD) 42.44(±12.73) 66.14(±11.02) <0.001a Femalegender(n%) 40(54.8) 20(55.6) 0.940 Previousresections(n%) 20(27.4) 0(0.0) 0.001a Laparoscopicsurgery(n%) 15(20.5) 9(25.0) 0.598 Hand-sewnend-to-end
anastomosis
3(4.1) 2(5.6)
0.210 Hand-sewnside-to-side
anastomosis
6(8.2) 7(19.4)
Stapledside-to-side anastomosis
64(87.7) 27(75.0)
23.3
8.2
17.8
15.1
1.4 13.9
16.7 16.7 16.7
8.3
0 5 10 15 20 25 30
Overall complications
(p = 0.250)
Anastomotic leakage (p = 0.185)
Surgical site infections (p = 0.883)
Other complications
(p = 0.829)
Death (p = 0.069)
CD (n = 73) CRC (n = 36)
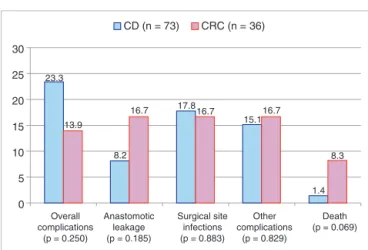
Fig.2–Postoperativecomplicationsbetweenthegroups.No significantstatisticaldifferencewasfound(Student’sttest).
Regarding the primaryoutcome ofour study,therewas no significant differences between the groups in terms of earlypostoperativecomplications.Overallcomplicationswere foundin17/73(23.3%)intheCDand in5/36(13.9%)inthe CRCgroups(p=0.250).Likewise,accordingtothespecifictype of complication analyzed, there was no significant differ-encebetweenthegroupsinrelationtoanastomoticleakage (p=0.185),surgicalsiteinfections(p=0.883),other complica-tions(0.829)anddeaths(p=0.069).Thesedataareillustrated indetailinFig.2.
Discussion
ICRs are widespread operations, performed due to a myr-iadofdifferentdiagnosisinthedailypracticeofgeneraland colorectalsurgeons.6Thesurgicalprocedureperseisnot
sig-nificantly differentbetweendifferent diseases.Peculiarities inCRC patientsshould alsobeofnotice, mainly regarding thediscussion ofextendedmesocolicresection inorder to respectoncologicalsurgicalprinciples.ICRcanbeperformed byconventional (open) approach or by minimally invasive techniques (multiport laparoscopy, single-port or robotics), independentlyofthediagnosis.Severalstudiesdemonstrated thefeasibilityofminimallyinvasiveproceduresevenin com-plicatedcasesofCD.3,10,11
In our study,the majority ofthe patients submitted to ICRhad adiagnosisofCD (67%)ascomparedtoCRC(only 33%ofthepopulation).Thiswasnotobservedinotherseries in the literature, as CRC tend to be a more common rea-sonforICRingeneralsurgicalpractice.Inasnapshotaudit fromtheEuropeanSocietyofColoproctology(ESCP)with3208 patients,only11.7%(n=371)wereoperatedduetoCD,whereas 78.4%(n=2515)hadright-sidedCRC.12Inaretrospectiveseries
(n=131)fromageneralsurgeon’sperspective,thesame pat-ternwasobserved:themajorityofpatientshadmalignancy (92/131–70.3%),whileCDwastheindicationforsurgeryin theminority(39/131–29.7%).13Oursamplehadamajorityof
patientsofCDpossiblyduetoareferralbias,asbothunitsare tertiaryreferralcentersforinflammatoryboweldiseases(IBD) medicalandsurgicalmanagement.Anotherpossiblereason isthatmoregeneraland digestivesurgeonsinourcountry
dooperationsforCRC,butnotasmuchforcomplicatedCD, whatcouldexplainthisimportantdifferenceofourstudyin comparisontootherseries.
In thepresent study,the groupswere homogeneousfor important surgical variables, mainly the surgical approach andthetypeofanastomosis.CRCpatientsweresignificantly older than CDpatients, whatclearly couldbe expected,as theprevalenceofCDisincreasedintheyounger,whilstthe incidence ofmalignancytends to behigher inthe elderly. Moreover,patientswithCDhadmorepreviousresectionsthan thosewithCRC,whatwasalsoexpected,asthenaturalhistory ofrecurrenceofCDusuallytendstowardrepeatedoperations overtime,mainlyifnotadequatepostoperativemedical ther-apywasused.
In regards to the primary objective of our study, no differenceswereobservedinoverallearlypostoperative com-plicationsbetweenCD(23.3%)andCRC(13.9%)–p=0.250.This was in accordance to a large series ofpatients with com-parison between the outcomes ofCD vs. non-CD patients. Mascarenhasetal.foundthatmajorcomplicationrateswere notdifferentbetweentheCD(5.4%)andnon-CDpatients(4%) –p=0.58.Thesamepatternwasobservedforminor complica-tions(5.4%vs.9.9%,respectively,p=0.16).Ourhigherratesof complications,incomparisontothisseries,canbeprobably explainedbytwofactors:first,referralbiasduetomore com-plicatedcasesofCDandadvancedtumorsintheCRCgroup, asbothunitsarereferralcentersfromthepublicsystemina developingcountry(tendencytomoreadvancedandsevere cases); secondly, the teaching hospital profileofthe units, whereresidentstendtoperformproceduresunder supervi-sion.
Inoursampleofpatients,anastomoticleakagewasfound in 8.2%ofthe CDand in 16.7%ofthe CRC resections per-formed.Inthe biggestseriesoftheliteraturetodate(ESCP snapshotstudy),theoverallleakageratewas8.1%(7.2%for CRCand9%forCD,with15.8%forotherindications).12The
expected tendency of higher anastomotic problems in CD incomparisontoCRC,mostlyduetothecomplexityofthe procedures(inflammatorymasses,phlegmons,fistulas) mal-nutrition,anemiaorpreoperativesteroids,wasnotfoundin ourstudy.Maybewithawidersampleofpatients,this differ-encecouldbeencountered(possibletypeIIerrorinourstudy, asnosamplecalculationcouldbemadeduetothe observa-tionaldesign).
Thereiscontroversyifthetypeofanastomosiscanaffect the rates of anastomotic leakage. A prospective study by McLeodetal.demonstratednodifferencesincomplications between the two different techniques.14 A meta-analysis
published in 2014 demonstrated that stapled side-to-side anastomosis tend to be safer than hand-sewn end-to-end anastomosis inseveralaspects,mainlyindehiscence,with anOddsRatio(OR)of0.45,with95%confidenceinterval(CI) 0.20–1.00.2TheESCPsnapshotstudycametooppositeresults,
withhigherriskfordehiscenceinpatientswithstapled anas-tomosis(OR 1.43,95% CI 1.04–1.95,p=0.03)in multivariate analysis.12 In our study, we could not check the relation
AnotherimportantpointisthatallCDpatientsinourstudy hadpreviousimmunosuppressionwithathiopurine,a biolog-icalagentorboth,and thisdidnotaffectthepostoperative complicationrates.Thisisinaccordancetothe studyfrom Mascarenhasetal.,6andwithothertworetrospectivestudies
wepublishedaimingtheimpactofimmunomodulatorsand biologicalagentsinpostoperativeoutcomesinCD.15,16
Ourstudyhasimportantlimitationsthatmightbe consid-eredintheanalysisoftheresults.Allbiasesfromretrospective chartreviewsfromtwodifferentunits,thatcouldimpairdata collection,shouldbetakeninto account.Thereduced sam-pleofpatientscould notleadtopropersubgroupanalysis, regardingtypeofanastomosisandlaparoscopicprocedures, forexample.Wealsocouldnothaveprecisedatafrom preop-erativemedicationintheCDgroup,whatcouldalsocontribute tothestudy’sresults.However,ourstudy’sstrengthisbased ontheprecisemethodology,asfewstudiesaimedthisspecific comparisonbetweenthetwodifferentdiseases.
Insummary,ourretrospectivecomparativestudydidnot demonstrateanydifferencesinpostoperativecomplications betweenCDandCRCpatientssubmittedtoICR.Nodifferences inanastomoticleakagewerefound,aswell asinmortality rates.Theexperienceofthesetwoteachinghospitalsin colo-rectalsurgerycanstimulateprospectivedatainourcountry intoorderoutlinepossibledifferencesinthesurgical man-agementofCDandCRC,whatcouldleadtooptimizationof individualizedtherapyforeachpatient.
Conflicts
of
interest
EFMisaspeakerforAbbvie,JanssenandTakeda.RSHandLS arespeakers forAbbvie andJanssen. PGKisaspeakerand consultantforAbbvie,Ferring,Janssen,PfizerandTakeda.
r
e
f
e
r
e
n
c
e
s
1. BaumgartD,SandbornWJ.Crohn’sdisease.Lancet. 2012;380:1590–605.
2. HeX,ChenZ,HuangJ,LianL,RouniyarS,WuX,etal.stapled side-to-sideanastomosismightbebetterthanhandsewn end-to-endanastomosisinileocolicresectionforCrohn’s disease:ameta-analysis.DigDisSci.2014;59:1544–51. 3. EshuisEJ,SlorsJFM,StokkersPCF,SprangersMAG,UbbinkDT,
CuestaMA,etal.Long-termoutcomesfollowing
laparoscopicallyassistedversusopenileocolicresectionfor Crohn’sdisease.BrJSurg.2010;97:563–8.
4. MunkholmP,LangholzE,DavidsenM,BinderV.Intestinal cancerriskandmortalityinpatientswithCrohn’sdisease. Gastroenterology.1993;105:1716–23.
5.OliveraP,SpinelliA,Gower-RousseauC,DaneseS, Peyrin-BirouletL.Surgicalratesintheeraofbiological therapy:up,downorunchanged?CurrOpinGastroenterol. 2017;33:246–53.
6.MascarenhasC,NunooR,AsgeirssonT,RivieraR,KimD, HoedemaR,etal.Outcomesofileocolicresectionandright hemicolectomiesforCrohn’spatientsincomparisonwith non-Crohn’spatientsandtheimpactofperioperative immunosuppressivetherapywithbiologicsandsteroidson inpatientcomplications.AmJSurg.2012;203:375–8. 7.SpinelliA,BazziP,SacchiM,DaneseS,FiorinoG,MalesciA,
etal.Short-termoutcomesoflaparoscopycombinedwith enhancedrecoverypathwayafterileocecalresectionfor Crohn’sdisease:acase-matchedanalysis.JGastrointestSurg. 2013;17:126–32.
8.SerradoriT,GermainA,ScherrerML,AyavC,PerezM,Romain B,etal.Theeffectofimmunetherapyonsurgicalsite infectionfollowingCrohn’sdiseaseresection.BrJSurg. 2013;100:1089–93.
9.AppauKA,FazioVW,ShenB,ChurchJM,LasnherB,RemziF, etal.UseofInfliximabwithin3monthsofileocolonic resectionisassociatedwithadversepostoperativeoutcomes inCrohn’spatients.JGastrointestSurg.2008;12:1738–44. 10.KotzePG,Abou-RejaileVR,BarcelosIF,MartinsJF,MirandaEF,
RochaJG,etal.Complicationsafterintestinalresectionin Crohn’sdisease:laparoscopicversusconventionalapproach.J Coloproctol.2013;33:139–44.
11.SoopM,LarsonDW,MalireddyK,CimaRR,Young-FadokTM, DozoisEJ.Safety,feasibility,andshort-termoutcomesof laparoscopicallyassistedprimaryileocolicresectionfor Crohn’sdisease.SurgEndosc.2009;23:1876–81. 12.PinkneyT,theEuropeanSocietyofColoproctology
collaboratinggroup.Therelationshipbetweenmethodof anastomosisandanastomoticfailureafterright
hemicolectomyandileo-caecalresection:aninternational snapshotaudit.ColorectalDis.2017,
http://dx.doi.org/10.1111/codi.13646[Epubaheadofprint]. 13.AhmedM,KirbyR.Electiverighthemicolectomy:a
twenty-yearretrospectiveanalysisofasinglegeneral surgeon’spractice.MinervaChir.2012;67:235–9. 14.McLeodRS,WolffBG,RossS,ParkesR,McKenzieM,
InvestigatorsoftheCASTTrial.RecurrenceofCrohn’sdisease afterileocolicresectionisnotaffectedbyanastomotictype: resultsofamulticenter,randomized,controlledtrial.Dis ColonRectum.2009;52:919–27.
15.KotzePG,SaabMP,SaabB,KotzeLMS,OlandoskiM,Pinheiro LV,etal.Tumornecrosisfactoralphainhibitorsdidnot influencepostoperativemorbidityafterelectivesurgical resectionsinCrohn’sdisease.DigDisSci.2017;62:456–64. 16.YamamotoT,SpinelliA,SuzukiY,Saad-HossneR,TeixeiraFV,