w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Quality
of
life
of
patients
with
inflammatory
bowel
disease
Thais
Karla
Vivan
a,∗,
Bianca
Mariz
Santos
a,
Carlos
Henrique
Marques
dos
Santos
baHospitalRegionaldoMatoGrossodoSul,CampoGrande,MS,Brazil
bColégioBrasileirodeColoproctologia,CampoGrande,MS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received13February2017 Accepted19June2017
Availableonline9September2017
Keywords:
Inflammatoryboweldiseases Crohn’sdisease
Ulcerativecolitis Colitis
Qualityoflife
a
b
s
t
r
a
c
t
Rationale:Crohn’sdiseaseandnon-specificulcerativecolitisarepartofinflammatorybowel diseases.Theyhaveachronicevolution,leadingtoimportantrepercussionsonpatients’ qualityoflife.Measuringthissubjectiveparameterrequiresanevaluationtoolinclinical trialsandhealthprograms.The“InflammatoryBowelDiseaseQuestionnaire”isanAmerican instrumentofMcMasterUniversity,whichhaditsreproducibilityandvaliditydetermined instudiesinothercountriesasameasureofthequalityoflifeinIBD.
Objective:Toevaluatethequalityoflifeofpatientswithinflammatoryboweldiseasethrough theInflammatoryBowelDiseaseQuestionnaire,andtocorrelatetheresultswith sociode-mographicdataofthepatients.
Methods:This is a prospective cross-sectional study carried out with 58 patients; the patients’follow-upwasconductedattheoutpatientclinicofColoproctology.
Results:Amongthe58patientsevaluated,70.1%hadDC,62.1%werewomen,themeanage was46.08years,96.6%werenon-smokers,and24.1%weresubmittedtosurgeryforthe underlyingdisease.43%wereinacombinationtherapyscheme,44%inmonotherapy,and 12%werenotusingmedication.Significantchangeinqualityoflifewasobservedinpatients takingprednisone.
Conclusion: Thepatientswithbetterqualityoflifearethosewhoweretakingprednisone. Therewasnoothercorrelationwithsignificanceinthepatients’qualityoflife.
©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Qualidade
de
vida
dos
pacientes
com
doenc¸a
inflamatória
intestinal
Palavras-chave:
Doenc¸ainflamatóriaintestinal Doenc¸adeCrohn
Coliteulcerativa
r
e
s
u
m
o
Racional: Fazpartedasdoenc¸asinflamatóriasintestinaisadoenc¸adeCrohneaRetocolite UlcerativaInespecíficaPossuemevoluc¸ãocrônica,gerandorepercussões importantesna qualidadedevidadosdoentes.Mediresseparâmetrosubjetivorequeruminstrumentode avaliac¸ãoemensaiosclínicosedeprogramasdesaúde.O“InflammatoryBowelDisease
∗ Correspondingauthor.
E-mail:[email protected](T.K.Vivan). http://dx.doi.org/10.1016/j.jcol.2017.06.009
Colite
Qualidadedevida
Questionnaire”éuminstrumentonorte-americanodaMcMasterUniversity,quetevesua reprodutibilidadeevalidadedeterminadaemestudosemoutrospaíses,comomedidada qualidadedevidaemdoenc¸asinflamatóriasintestinais.
Objetivo: Avaliaraqualidadede vidadospacientescomdoenc¸ainflamatória intestinal atravésdoquestionário“InflammatoryBowelDiseaseQuestionnaire”,ecorrelacionaros resultadoscomdadossociodemográficosdospacientes.
Método: Estudoprospectivotransversal,realizadocom58pacientes,acompanhamentono ambulatóriodeColoproctologia.
Resultados: Dentreos58pacientesavaliados,70,1%possuíamDC,62,1%mulheres,idade médiade46,08anos,96,6%nãotabagistas,24,1%submetidosàcirurgiapeladoenc¸adebase. Estavamemusodeterapiacombinada43%,monoterapia44%esemusodemedicamento 12%.Foiobservadaalterac¸ãosignificativadaqualidadedevidanospacientesemusode prednisona.
Conclusão: Ospacientescommelhorqualidadedevida sãoosqueestavamemusode prednisona.Nãohouveoutracorrelac¸ãocomsignificâncianaqualidadedevida.
©2017SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
Crohn’s disease (CD) and idiopathic ulcerative rectocolitis (IUR) are the forms of inflammatory bowel diseases (IBD), beingcharacterizedbyachronicinflammationoftheintestine. ThecauseofIBDisstillunknownandthereissome interac-tionbetweengenetic,environmentalandimmunefactors.1,2
Thesediseasesaffectyoungandoldpeople,withno predilec-tionasforraceandgender.3,4
AccordingtoOrdinanceNo.483ofApril1,2014mofthe BrazilianMinistryofHealth,chronicdiseasesarethose disor-derswithagradualonset,withalongoruncertainduration, and which, ingeneral,present multiplecauses and whose treatmentinvolveschangesofthepatient styleoflife,ina processofcontinuouscarethatusuallydoesnotleadtoone’s healing.
Theconceptofqualityoflife(QoL)referstohowwellpeople performtheirfunctionsindailylifeandthepersonal assess-mentoftheirwell-being,andtheformsofinflammatorybowel disease,bothIURandCD,haveimportantrepercussionsonthe QoLofthecarriers.5
ThemeasurementofQoLisanimportantparameterwhen oneassessestheimpactofchronicdiseases,sincethe physi-ologicalchanges,despiteprovidingimportantinformationfor theclinician,cancausevariouseffectsbothforpatientsand theirfamilies,astheyinfluencefunctionalcapacityand well-being–criticalaspectsforthepatient.6,7
InordertoevaluatetheQoLofpatientswithinflammatory bowel disease,the “Inflammatory Bowel Disease Question-naire”questionnaire,alreadyvalidatedinBrazil,wasapplied andsubsequentlywecorrelatedtheIBDQdatawith sociode-mographicandmorbiditydataavailable.
Methods
Thisisacross-sectional,prospectivestudy,withnoconflictof interest,andcostswillbebornebytheresearchers.Thestudy
wasconductedfromAugust2016toJanuary2017,andinvolved patientswithIBDregisteredintheexceptionalmedicine pro-gramoftheHealthDepartmentoftheStateofMatoGrosso doSul(MS),aftertheirevaluationbyanauditorphysicianand withthe Ordinancecriteria beingfulfilled.Patientswithan undeterminedcauseofcolitisandpatientsundergoing diag-nosticinvestigationwereexcluded.
ToevaluatetheQoL,theNorthAmericanformof McMas-ter University, “Inflammatory Bowel Disease Questionnaire (IBDQ)”, a questionnaire translated and validated in Por-tuguese, was the instrument applied, along with a small formonmorbidityandsociodemographiccharacteristics.The IBDQconsistsof32itemscoveringfour domains:intestinal symptoms,systemicsymptoms,socialaspects,andemotional aspects,andtheresponseoptionsarepresentedintheform ofmultiplechoice,withsevenalternatives.Thescores1and 7mean,respectively,theworseandthebetterstateofQoL.5,6
Thevolunteerpatientsansweredthequestionnaires with-out any externalhelp; oncecompleted, the questionnaires wereconfidentiallydepositedinabox.
After the data collection, the IBDQ results were cross-checked with the questionnaire on socio-demographic characteristics, as follows: age, gender, disease, diagnosis time,surgeryresultingfromthedisease,medicationinuse, smoking,anddiseaseactivity.TheresultsoftheIBDQwere submittedtostatisticaltreatmentwiththeuseofSPSS (ver-sion23)andGraphPadPrism(version6.01)programs,cluster analysis, and the chi-squaredtest, withsignificance estab-lishedasp<0.05.
Results
Descriptiveanalysis
Ageandgender
37,9%
62,1%
Male Female
Total = 58
Fig.1–Distributionofthepatientsstudiedbygender.
15,5%
19,0% 15,5%
5,2%
15,5% 25,9%
Total = 58
10 - 19 years 20 - 29 years 30 - 39 years 40 - 49 years 50 - 59 years 60 - 69 years 70 - 79 years 3,4%
Fig.2–Distributionofthepatientsstudiedbyagegroup.
100
90
80
70
60
50
40
30
20
10
0
Male Female
70 years and over 60 - 69 years 50 - 59 years 40 - 49 years 30 - 39 years 20 - 29 years 10 - 19 years
Relativ
e frequency (%)
Fig.3–Distributionofthepatientsstudiedbyagegroup
andgender.
42.5±17.3 years; forwomen(n=36,62.1% of the total)the meanagewas48.3±13.4years.
Fig.1illustratesthedistributionbetweengenders,while Figs.2and3listtheagegroupsoftheparticipants.
Onlytwo(3.4%)patientsweresmokers(onewithCDand onewithURC)and56(96.6%)didnotsmoke.Only14(24.1%) patientsunderwentsurgeryduetoaninflammatorydisease; ofthesepatients,13hadadiagnosisofCDandonlyonepatient hadURC.
Regardingtreatment,sevenpatients(12.06%)werenoton medication,25(43.01%)werebeingtreatedwithcombination
Table1–DrugsinusebypatientssufferingIBD.
Druginuse Numberofpatients(%)
None 7(12.06%)
Salicylate,oral 13(22.41%)
Salicylate,suppository/enema 6(10.34%)
Methotrexate 1(1.7%)
Prednisone 12(20.68%)
Azathioprine 24(41.37%)
AntiTNF 22(37.93%)
Table2–Diagnosistimeandnumberofpatients.
Diagnosistime Numberofpatients(%)
Lessthan1year 10(17.2%)
1–2years 7(12%)
2–3years 13(22.4%)
Morethan5years 28(48.2%)
Table3–Distributionofdiseasefrequenciesaccordingto gender.
Gender Total
Male Female
Crohn’sdisease 16(27.6%) 25(43.1%) 41(70.7%) Ulcerativerectocolitis 6(10.3%) 11(19.0%) 17(29.3%)
Total 22(37.9%) 36(62.1%) 58(100.0%)
therapy,and26(44.08%)wereonmonotherapy.Table1lists thedrugsinuse.
Whenaskedaboutdiseaseactivity,31patientsthoughtthe diseasewasactive,13believedthatthediseasewasnotactive, and14didnotknowaboutit.Table2liststhediagnosistimes.
Disease
Table3showsthefrequencydistributionofdiseases, accord-ing to gender, while Table 4 shows the same distribution accordingtoagegroup.
QoL
Thesumofthescoresofeachdomainwasdividedbythe num-berofquestionsthat composedthedomain,andthesame procedurewasdoneforthetotalscore.Thesevaluesare pre-sentedinTables5–7,withrespecttogender,agegroup,and disease,respectively.
Inferentialanalysisofthedependentvariable“QoL”.
QoLversusgender. TheD’AgostinoandPearson normal-itytest,appliedtothetotalvaluesofQoL,revealedthatwe were facedwithaparametric sampling distribution, which authorizedustousetheStudent’sttesttotrytofindsignificant differencesbetweenthegroups.
The“t”testrevealednosignificantdifferencesbetweenthe groupstested(p=0.2374),indicatingthatthegenderdidnot influencetheQoLofthepatient.Fig.4illustratesthisfinding.
Table4–Distributionofdiseasefrequenciesaccordingtoagegroup.
Agegroup(years) Total
10–19 20–29 30–39 40–49 50–59 60–69 70–79
Crohn’sdisease 2(4.9%) 9(15.5%) 8(13.8%) 5(8.6%) 8(13.8%) 7(12.1%) 2(3.4%) 41(70.7%) Ulcerativerectocolitis 0(0.0%) 0(0.0%) 3(5.2%) 4(6.9%) 7(12.1%) 2(3.4%) 1(1.7%) 17(29.3%) Total 2(3.4%) 9(15.5%) 11(19.0%) 9(15.5%) 15(25.9%) 9(15.5%) 3(5.2%) 58(100.0%)
Table5–Meanandstandarddeviationofcorrectedscores,accordingtodomainsandgender.
Gender Domains
Bowel Systemic Social Emotional Total
Male 4.90±1.66 4.45±1.55 5.10±1.83 4.32±1.91 153±50
Female 4.54±1.49 3.96±1.67 4.58±1.75 4.33±1.55 137±46
Total 4.68±1.55 4.14±1.63 4.78±1.78 4.33±1.68 143.3±47.7
Table6–Meanandstandarddeviationofcorrectedscores,accordingtodomainsandagegroup.
Agegroup Domains Total
Bowel Systemic Social Emotional
10–19years 4.90±1.98 4.20±1.98 4.70±1.56 4.50±1.65 145±47
20–29years 5.68±0.90 4.84±1.04 6.22±1.25 5.15±0.77 175±23
30–39years 4.12±1.71 3.84±1.51 4.31±1.88 4.39±1.51 130±53
40–49years 4.04±1.58 3.18±1.53 3.53±1.87 2.81±1.65 114±52
50–59years 4.35±1.51 4.01±1.97 4.55±1.67 4.29±1.60 141±46
60–69years 5.08±1.56 4.53±1.56 5.29±1.60 4.78±2.09 149±49
70–79years 5.87±1.27 5.47±1.10 5.60±1.25 4.89±2.01 179±35
Total 4.68±1.55 4.14±1.63 4.78±1.78 4.33±1.68 143.3±47.7
Table7–Meanandstandarddeviationofcorrectedscores,accordingtodomainsanddisease.
Disease Domains
Bowel Systemic Social Emotional Total
Crohn’sdisease 4.77±1.53 4.22±1.66 4.91±1.77 4.28±1.70 145±48
Ulcerativerectocolitis 4.45±1.63 3.95±1.57 4.47±1.82 4.43±1.67 138±48
Total 4.68±1.55 4.14±1.63 4.78±1.78 4.33±1.68 143.3±47.7
Male Female
Qua
lity of lif
e
210
180
150
120
90
60
30
0
Fig.4–Qualityoflifeaccordingtogender.
Theanalysisofvariancerevealednosignificantdifferences betweenthegroupstested(p=0.1122),indicatingthattheage groupdidnotexertinfluenceinthelifeofthepatient.Fig.5 illustratesthisfinding.
QoLversus domain. TheD’Agostino andPearson’s nor-malitytest,appliedtothecorrectedvaluesofthedifferent
250
200
150
100
50
10-19 years
Quality of lif
e
20-29 years
30-39 years
50-59 years
60-69 years
70-79 years 40-49
years 0
Fig.5–Qualityoflifeaccordingtoagegroup.
7
6
5
4
3
2
1
0
Corrected score
Bowel factors
Systemic factors
Social factors
Emotional factors
Fig.6–Qualityoflifeaccordingtodomain.
Model summary
Algorithm Twostep
4
2
-1,0 -0,5
Silhouette measure of cohesion and separation Poor Fair Good
0,0 0,5 1,0
Inputs
Clusters
Cluster quality
Fig.7–Clusteranalysisappliedtostudydomains.
Silhouetteindex=0.6.
Table8–Contingencetableforqualityoflifeaccording toprednisoneuse.
Useofprednisone Betterquality oflife
Poorerquality oflife
Total
No 19(32.7%) 27(46.6%) 46(79.3%)
Yes 11(19.0%) 1(1.7%) 12(20.7%)
Total 30(51.7%) 28(48.3%) 58(100.0%)
Theone-way ANOVA test revealed no significant differ-ences amongthe values of the domains tested (p=0.157), indicatingthatnoneofthedomainshaveagreaterimportance intheQoLofthepatient.Fig.6illustratesthisfinding.
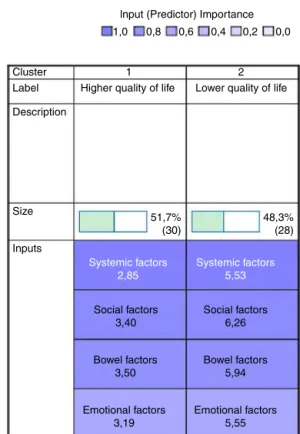
Domainsversusmedication. Theclusteranalysisapplied tothedomainsbytheTwoStepalgorithmrevealsthepresence oftwodistinctgroups,asshowninFigs.7and8.
Basedonthisdistributionofpatientsintwodistinctgroups, analyseswereperformedbasedonchi-squaredtests,inorder todeterminesignificantcorrelationsbetweenQoLandthe var-ioussociodemographicfactors,amongthemthemedication usedbythepatientsinthesample.
It was found that the use of prednisone significantly increasespatients’QoL(p=0.0026),asshowninTable8.
Clusters
Cluster
Label Higher quality of life Lower quality of life
Description
Size
51,7% (30)
48,3% (28)
Inputs
Systemic factors 2,85
Social factors 3,40
Bowel factors 3,50
Emotional factors 3,19
Emotional factors 5,55 Bowel factors
5,94 Social factors
6,26
Systemic factors 5,53
1 2
lnput (Predictor) Importance
1,0 0,8 0,6 0,4 0,2 0,0
Fig.8–Theimportanceofeachdomaininthepredictionof
qualityoflife.
Discussion
IBDscanpermanentlyaltertheQoLofpatients’lives, espe-ciallywhenthedisordergoesthroughaperiodofexacerbation. The symptoms presentedby patients with IBD can gener-atechangesthathaveagreatimpactonattitudes,behaviors, andproductivity,aswellasinphysical,emotional,andsocial aspects.
In this study, wecan observe the occurrence ofa peak incidenceofIBDbetween50and59yearsofage.The predom-inanceofCDinwomenandthebimodalpresentation(20and 50years)iscompatiblewithfindingsintheliterature.However, contrarytowhathasbeenobservedinsomestudies,IUGRwas predominantlyinwomen,notinmen.6
Smokingdidnotinfluencethisstudysincethenumberof patients(n=2)wasnotrelevant.
When scores taking into account the diagnoses were assessedseparately,nostatisticallysignificantdifferencewas observedforCDversusIUGR,andthisresultwassimilarto thatfoundinastudyconductedinSpain.8Also,nostatistical
relevancewasobservedwhentheIBDQscorewascorrelated withsociodemographicdata.
Conclusion
Therewasno statisticalsignificanceofthe QoLofpatients withIBDwhencomparedwithsociodemographicvariables. Onthe other hand,the clusteranalysisdemonstrated that thesystemicdomainofIBDQcanbeconsideredagood pre-dictorofQoLandthat,inaddition,patientswhoweretaking prednisonehadbetterscoresforQoL.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Appendix
A.
Supplementary
data
Supplementarydataassociatedwiththisarticlecanbefound, intheonlineversion,atdoi:10.1016/j.jcol.2017.06.009.
r
e
f
e
r
e
n
c
e
s
1.SilvaAF,SchieferdeckerMEM,AmaranteHMBS.Ingestão alimentarempacientescomdoenc¸ainflamatóriaintestinal. ABCDArqBrasCirDig.2011;24:204–9.
2.Kleinubing-JuniorH,PinhoMSL,FerreiraLC,BachtoldGA, MerkiA.Perfildospacientesambulatoriaiscomdoenc¸as inflamatóriasintestinais.ABCDArqBrasCirDig.2011;24:200–3. 3.BraunwaldE,FauciAS,HauserSL,LongoDL,KasperDL,
JamesonJL.Medicinainterna,vol.II,secc¸ão289,17ed.Riode Janeiro:McGraw-hill;2010.
4.WareJE.Standardsforvalidatinghealthmeasures:definition andcontent.JCrohnicDis.1987;40:473–80.
5.PontesRMA.Qualidadedevidaempacientesportadoresde doenc¸ainflamatóriaintestinal:traduc¸ãoparaoportuguêse validac¸ãodoquestionário“InflammatoryBowelDisease Questionnaire”(IBDQ).ArqGastroenterol.2004;41:137–43. 6.SouzaMM,BarbosaDA,EspinosaMM,BelascoAGS.Qualidade
devidadepacientesportadoresdedoenc¸ainflamatória intestinal.ActaPaulEnferm.2011;24:479–84.
7.DeBoerAG,BennebroekEvertsz’F,StokkersPC,BocktingCL, SandermanR,HommesDW,etal.Employmentstatus, difficultiesatworkandqualityoflifeininflammatorybowel diseasepatients.EurJGastroenterolHepatol.2016;28:1130–6. 8.CasellasF,ArenasJI,BaudetJS,FábregasS,GarcíaN,GelabertJ,