w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Splicing
factor
SF3B1
mutations
and
ring
sideroblasts
in
myelodysplastic
syndromes:
a
Brazilian
cohort
screening
study
Flávia
Sacilotto
Donaires
a,
Felipe
Martelli
a,
Raquel
de
Melo
Alves-Paiva
a,
Silvia
Maria
Meira
Magalhães
b,
Ronald
Feitosa
Pinheiro
b,
Rodrigo
Tocantins
Calado
a,∗aUniversidadedeSãoPaulo(USP),RibeirãoPreto,SP,Brazil
bUniversidadeFederaldoCeará(UFC),Fortaleza,CE,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received13May2016 Accepted7June2016 Availableonline4July2016
Keywords:
Myelodysplasticsyndromes Ringsideroblasts
SF3B1
a
b
s
t
r
a
c
t
Background:Myelodysplasticsyndromes(MDS)compriseagroupofmalignantclonal hema-tologicdisorderscharacterizedbyineffectivehematopoiesisandpropensityforprogression toacutemyeloidleukemia.AcquiredmutationsinthegeneencodingRNAsplicingfactor 3Bsubunit1(SF3B1)arehighlyassociatedwiththeMDSsubtypespresentingring siderob-lasts,andrepresentaspecificnosologicalentity.Theeffectsofthesemutationsonclinical outcomesarediverseandcontrasting.
Methods:Acohortof91BrazilianMDSpatients,includingpatientswithringsideroblastsin thebonemarrow,werescreenedformutationsintheSF3B1hotspots(exons12–15)bydirect Sangersequencing.
Results:SF3B1heterozygous mutationswereidentifiedin sixpatients (7%),all of them with ring sideroblasts, thusconfirming the association between SF3B1 mutations and myelodysplasticsyndromesubtypesbearingthismorphologicfeature(frequencyof6/13, p-value<0.0001).
Conclusion:ThisisthefirstscreeningofSF3B1mutationsinacohortofBrazilian myelodys-plastic syndrome patients. Our findings confirm that mutations in this splicing gene correlatewithbonemarrowringedsideroblasts.
©2016Associac¸ ˜aoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthorat:DepartmentofInternalMedicine,UniversidadedeSãoPaulo(USP),Av.Bandeirantes,3900,BlocoG,subsolo,
HCRP–Lab.Hematologia,14049-900RibeirãoPreto,SP,Brazil.Tel.:+551636022294. E-mailaddress:[email protected](R.T.Calado).
http://dx.doi.org/10.1016/j.bjhh.2016.06.002
Introduction
Myelodysplastic syndromes (MDS) are defined as clonal hematopoieticstemcelldisorderscharacterizedbycytopenia, myelodysplasia,ineffectivehematopoiesis,andpropensityfor progressiontoacutemyeloidleukemia.1–4 TheMDS
diagno-sisisarrivedatafterexclusionofothermyeloidneoplasms suchasacutemyeloidleukemia(AML),chronic myelomono-cyticleukemia(CML),andmyelodysplastic/myeloproliferative neoplasms.Morphologiccriteriafordiagnosisinclude dyspla-siapresent in atleast 10% ofcells ofany myeloid lineage withoneormoreaffectedlineagesofthebonemarrow.5The
dysplasticchangesobservedinthemyeloidlineagesprobably arisefromageneticallytransformed,primitivehematopoietic stemcell,followedbyothergeneticandepigeneticchanges,as wellasstromalandimmuneresponsesinthehost,that con-tributetophenotypicdiversity,hematopoieticefficiency,and susceptibilitytoleukemictransformation.6MDSiscategorized
in six subtypes, according to the World Health Organiza-tion (WHO) criteria revised in 20087: refractory cytopenia
withunilineagedysplasia(includingrefractoryanemia, neu-tropenia,and thrombocytopenia),refractorycytopenia with multilineage dysplasia, refractory anemia with excess of blasts, MDS with isolated del(5q), unclassifiable MDS, and refractory anemia with ring sideroblasts (RS). In the lat-ter,RS (perinuclearring ofgranules formedbyiron-loaded mitochondria) are observed in ≥15% of bone marrow
ery-throidprecursors.LargenumbersofRSare observedinthe bonemarrowofmorethanaquarterofpatientswithMDS,8
highlighting the importance of this subgroup in the dis-ease.
TheincidenceofMDSincreasesatage70yearsandolder9
andthedirectcorrelationwithagesuggestsgeneticdamage causedbyhazardous exposure, e.g.chemotherapy, ionizing radiation, diesel fuel, and smoking.2,5 A wide diversity of
mutationsinindividualgeneshasbeendescribed,suggesting thatseveralmolecularmechanisms areinvolvedindisease development.10 Whole-exomesequencingstudiesidentified
recurrentsomaticmutationsinspliceosomecomplexgenesin asignificantproportionofadultMDSpatients,with empha-sisontheSF3B1 (splicingfactor3b, subunit1)gene,mutated inabout20%ofpatients.3,11–13 Highfrequencieswere
espe-ciallyobservedinpatientswhosediseaseischaracterizedby thepresenceofRS,inwhichSF3B1mutationsweredetected in65%,1175%,3and56%10ofpatients.
TheSF3B1geneencodesthesubunit1ofthesplicing fac-tor3bprotein complex,whichformsthe U2small nuclear ribonucleoprotein complex (U2 snRNP) along with splicing factor 3a and a 12S RNA unit. Thiscomplex playsa criti-calroleinthesplicingmachineryandregulatesthediversity ofsplicevariants.14SF3B1isalsoinvolvedinthealternative
splicingprogramofgenesthatcontrolcellcycleprogression andapoptosis,whichmayelucidatethecriticalcontribution ofmutantSF3B1inmodulatingproliferationandsurvivalof tumorcells.15 TheSF3B1proteinisubiquitouslyand highly
expressedinhematopoieticlineages.16Thecarboxy-terminal
two-thirdsofthesubunit1has22non-identical,tandemHEAT domain(HD)repeats,andthemajorityofmutationsinMDS areclusteredintheregionencodingtheimperfectHD4–9,16
encompassingexons12–15(codons513–741).Mutationsare usuallysomaticdenovo,andoftencorrespondingtomissense nucleotidechangesclusteredmainlyinthreehotspots:codons 662,666,and700.15
Inthisstudy,91BrazilianMDSpatientswerescreenedfor mutationsintheSF3B1hotspotstoobservetheheterogeneity, andtheincidenceinaBrazilianpopulation.
Methods
Samples,DNAextraction,andpolymerasechainreactions
Patientsseenattwotertiaryhematologycentersinuniversity hospitalslocatedintwoseparateregionsinthecountrywere evaluated:oneinthesoutheast(RibeirãoPreto,SãoPaulo)and theotherinnortheastofBrazil(Fortaleza,Ceará)thataremore than2600kmapart.Thepopulationsintheregionswherethe twocentersarelocatedaresocially,economically,and ethni-callydiverse.Bloodsampleswerecollectedfrom91patients withMDSdiagnosedandclassifiedaccordingtotheWHO cri-teria(2008).7Forty-fiveMDSpatientsseenbetween2009and
2011atthehematologyclinic,HospitaldasClínicasdeRibeirão Preto,UniversidadedeSãoPaulo,andfromwhomDNA sam-pleswerepreviouslycollectedandavailablefortestingwere included in the study afterMDS diagnosis was confirmed. Forty-sixconsecutiveMDS patientsseenatthehematology clinic,UniversidadeFederaldoCeará,diagnosedbetween2008 and 2010 were also enrolled. Samples were collected and storedafterpatientshadgiventheirinformed written con-sent and the study had beenapproved bytheLocal Ethics Committee(CEP-HCRPn.7147/2005).Thestudywasconducted in accordance withthe Helsinki Declaration, as revised in 2008.
TotalgenomicDNAwasextractedfromblood leukocytes using TRIzol reagent (Ambion, Foster City, USA). All DNA sampleswereamplifiedbypolymerasechainreaction(PCR) using specific primers for exons 12–15 of the SF3B1 gene (RefSeqNM012433.2)andPlatinumTaqDNAPolymerasekit (Invitrogen, Carlsbad,USA)accordingtothe manufacturer’s instructions. Primer sequences used inamplification reac-tionsweredesignedaccordingtoMalcovatietal.17Thequality
ofPCRproductswasassessedbydenaturing1.5%agarosegel electrophoresisunderstandardconditions.ThePCRproducts werepurifiedusingtheQIAquickPCRPurificationkit(Qiagen, Hilden,Germany)accordingtothemanufacturer’s recommen-dations.
Sangersequencingandanalysis
Purified PCR fragments were directly sequenced in both directions. Sequencingreactions were performedusing the DYEnamic ET Dye Terminator Cycle Sequencing kit and the MegaBACE Long Read Matrix equipment (GE Health-careLife Sciences,Uppsala,Sweden).Chromatogramswere analyzed through the CLC Main Workbench software v5.7 (CLCbio,Katrinebjerg,Denmark).ThePolyPhen-2.0tool18was
Exon 14 – E622D
A
B
G>T
A>G
Score of possibly damaging 0.93
0.87
0.00 0.20 0.40 0.60 0.80 1.00 0.00
ACTGGTATTAAGATTGTACAAC
ACTGGTATTAGGATTGTACAAC ACTGGTATTAAGATTGTACAAC
ATGAGCAGCAGNAAGT-CGGAC
ATGAGCAGCAGGAAGTTCGGAC
ATGAGCAGCAGGAAGTTCGGAC
ACATGGATGAGTATGTCCGTA
ACATGGATGATTATGTCCGTA ACATGGATGAGTATGTCCGTA
0.20 0.40 0.60 0.80 1.00 0.00 0.20 0.40 0.60 0.80 1.00
0.99
G>A
Exon 14 – K666R
Exon 15 – K700E
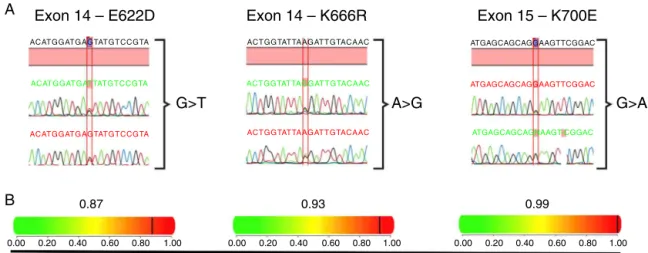
Figure1–HeterozygousmutationsinSF3B1foundinsixMDSpatients.(A)Chromatogramsofregionsofexons14and15 presentingnucleotidesubstitutionsthatleadtoaminoacidchangesintheSF3B1protein;onepatientexhibitedanE622D substitution,anotherone,aK666R,andfourpatientspresentedthemostcommondescribedsubstitution,K700E.(B) Representationoftheimpactofeachaminoacidsubstitutionontheproteinstructureandfunction,aswellasapredicted scorerangingfrom0to1,inwhich1representsthehigherprobabilityofdamagedprotein.
Statisticalanalysis
StatisticalanalysiswasperformedintheRsoftware environ-ment(http://www.r-project.org/).Pairwisecomparisonswere performedbyMann–Whitney test,and bytwo-sided Fisher exacttest(CI=0.95)forquantitativeandcategoricalvariables, respectively.
Results
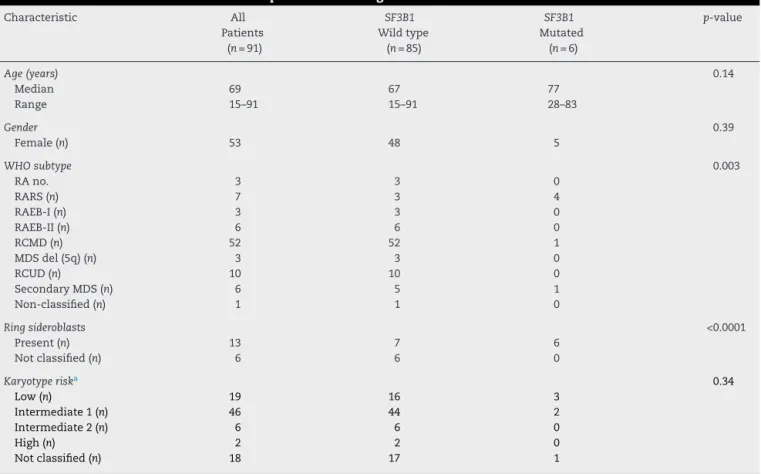
Sanger sequencing was performed in 91 Brazilian MDS patients and three non-synonymous SF3B1 heterozygous mutationswereidentified,leadingtomissensesubstitutions insixunrelatedpatients.ThemostcommonrecurrentSF3B1 mutationaffectedcodon700(K700E,fouroutofsixpatients); onepatientharboredamutationincodon622(E622D),and another one,incodon 666(K666R)(Figure 1A). The predic-tionofmutationmalignancyormildnessshowedmutations asprobablydamagingfortheproteinstructureandfunction, withhighscores,rangingfrom0.87to0.99(Figure1B). Con-sideringWHOsubtypes,differencesweredetectedcomparing wild type and mutated groups (p-value=0.003; Table 1). A strongassociationbetweenSF3B1mutationanddisease phe-notypewithRS(p-value<0.0001)wasobservedinthiscohort. Thirteenpatients(14.2%)werefoundwithRSandallsixSF3B1 mutatedpatients(6/13)presentedatleast15%ofRSinthe bonemarrow.ThecorrelationofSF3B1mutationsinMDSwith RS,themedianage,gender,karyotyperiskcomparisons,and clinicalcharacteristicsofpatientsareshowninTable1.
Discussion
ThisstudyfoundthatinaBraziliancohortofMDSpatients, SF3B1ismutatedinabout7%ofpatients,allofwhomhave RSinthebonemarrow.Thecurrentdiagnosticcriteria(WHO,
2008)forMDSaremainlybasedonmorphology4butMalcovati
etal.19demonstratedthefeasibilityofincludingamolecular
classificationinmyeloidneoplasms.Theinclusionof molec-ularanalysismightbevaluablenotjustfordiagnosis,butalso for prognosticpurposesand evaluationofdisease progres-sion. Therefore, the importanceofthe mutational analysis improves clinicaldecisionmaking,asdifferentpoint muta-tionsinMDShavedistincteffectsondiseasephenotypeand prognosis.19,20ApartfromtheWHOcategory,SF3B1mutation
statushasapositivepredictivevalue(97.7%)fordisease phe-notypewithRS,whereas the absenceofRShadanegative predictivevalue(97.8%)forthemutations.4,17
HowSF3B1 mutationscontributetoMDSpathogenesisis still unclear.Thepotentialmechanism responsibleforiron accumulation inthe mitochondriaoferythroblasts in MDS characterizedbyRSisthereducedexpressionoftheABCB7 gene,whichplaysessentialrolesinbothmitochondrialiron homeostasisandhematopoiesis.21,22Thedown-regulationof
ABCB7 haspreviouslybeen associatedwithover-expression ofFTMT (encodingmitochondrialferritin) inhematopoietic progenitors.23,24 The mitochondrial ferritin has ferroxidase
activity,capturingironintheferrousform,depositingasferric hydroxidesafteroxidation.Theaccumulationofthisprotein inerythroblastswasaccompaniedbymarkedlyreduced ery-throidgrowthinvitroduetothedown-regulationofABCB7.25
Theabnormal mRNAsplicingdueto mutatedSF3B1 might leadtoanabnormalABCB7protein,deregulating mitochon-drialferritinintheimmatureredbloodcells,thusculminating inthediseasephenotype.
Conversely,Visconteetal.26didnotobserveanydifferences
Table1–Clinicalcharacteristicsof91MDSpatientsaccordingtoSF3B1mutationstatus.
Characteristic All
Patients (n=91)
SF3B1
Wildtype (n=85)
SF3B1
Mutated (n=6)
p-value
Age(years) 0.14
Median 69 67 77
Range 15–91 15–91 28–83
Gender 0.39
Female(n) 53 48 5
WHOsubtype 0.003
RAno. 3 3 0
RARS(n) 7 3 4
RAEB-I(n) 3 3 0
RAEB-II(n) 6 6 0
RCMD(n) 52 52 1
MDSdel(5q)(n) 3 3 0
RCUD(n) 10 10 0
SecondaryMDS(n) 6 5 1
Non-classified(n) 1 1 0
Ringsideroblasts <0.0001
Present(n) 13 7 6
Notclassified(n) 6 6 0
Karyotyperiska 0.34
Low(n) 19 16 3
Intermediate1(n) 46 44 2
Intermediate2(n) 6 6 0
High(n) 2 2 0
Notclassified(n) 18 17 1
RA:refractoryanemia;RARS:refractoryanemiawithringsideroblasts;RAEB-I,II:refractoryanemiawithexcessblasts;RCMD:refractory cytopeniawithmultilineagedysplasia;MDSdel(5q):MDSwithisolated5qdeletion;RCUD:refractorycytopeniawithunilineagedysplasia.
a BasedontheInternationalPrognosticScoringSystem.
levelsofgenesrelevanttotheMDSpathophysiology(suchas ASXL1,CBL,EZH1,andRUNX3),thesegeneswerefound alter-nativelysplicedinatleastoneexon,suggestingthatSF3B1 mutationsare foundermutationsthatpromotesubsequent acquisitionofgeneticabnormalities.
SF3B1mutationsmightleadtoproteinsexhibitinggain-or loss-of-function,whichmayfoster,forinstance,clonal expan-sionand dominance ofhematopoieticprogenitors carrying the mutation.Malcovatiet al.17 showed the assessmentof
SF3B1mutantalleleburdenrevealingthepresenceofa domi-nantclonewithaheterozygousmutationinmostofthecases. Moreover,patientscarryingthis molecularlesionpresented asignificantly better overall survival comparedwith those withoutthemutation,whichindicates thatSF3B1mutation analysisisanimportantpredictorofclinicaloutcomesinthese disorders.17
ThisstudyisthefirsttoreportonSF3B1genemutations inBrazilianMDSpatients.Thefrequencyofmutationsinthis splicinggeneinpatientspresentingRStendedtobelowerthan describedinpreviousstudiesinEuropeanandNorthAmerican populations.Thisapparentdisagreementmayreflectboththe heterogeneityoftheBrazilianpopulationdueto miscegena-tionand/ortherestrictedanalysisperformedinthisstudy,asit focusedonhotspotmutationsonly.MDSisunder-diagnosed inBrazil,27 whichmayalsocontributetothedifferences in
mutationfrequencyobservedinthepresentstudy.The impor-tanceofthemolecularanalysisinaheterogeneousgroupof diseasessuchasMDSisundisputable,especiallyforimproving diagnosisandprognosis.
Conclusion
SixheterozygousmutationsintheSF3B1genewereidentified inacohortof91BrazilianMDSpatients,whichwerehighly cor-relatedwiththepresenceofbonemarrowRS,similartowhat waspreviouslyreportedinstudiesofdifferentpopulations. Thisobservationhighlightstheimportanceofmolecular anal-ysisinthesediseasesbesidesmorphologicalandcytogenetics analysesofthehematopoieticlineages.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
r
e
f
e
r
e
n
c
e
s
1. VardimanJW.Hematopathologicalconceptsand controversiesinthediagnosisandclassificationof
myelodysplasticsyndromes.HematolAmSocHematolEduc Program.2006:99–204.
2. OraziA,CzaderMB.Myelodysplasticsyndromes.AmJClin Pathol.2009;132(2):290–305.
3. YoshidaK,SanadaM,ShiraishiY,NowakD,NagataY, YamamotoR,etal.Frequentpathwaymutationsofsplicing machineryinmyelodysplasia.Nature.2011;478(7367):64–9.
4. CazzolaM,DellaPortaMG,MalcovatiL.Thegeneticbasisof myelodysplasiaanditsclinicalrelevance.Blood.
2013;122(25):4021–34.
5. CoreySJ,MindenMD,BarberDL,KantarjianH,WangJC, SchimmerAD.Myelodysplasticsyndromes:thecomplexityof stem-celldiseases.NatRevCancer.2007;7(2):118–29.
6. TefferiA,VardimanJW.Myelodysplasticsyndromes.NEnglJ Med.2009;361(19):1872–85.
7. VardimanJW,ThieleJ,ArberDA,BrunningRD,BorowitzMJ, PorwitA,etal.The2008revisionoftheWorldHealth Organization(WHO)classificationofmyeloidneoplasmsand acuteleukemia:rationaleandimportantchanges.Blood. 2009;114(5):937–51.
8. NavarroI,RuizMA,CabelloA,ColladoR,FerrerR,HuesoJ, etal.Classificationandscoringsystemsinmyelodysplastic syndromes:aretrospectiveanalysisof311patients.LeukRes. 2006;30(8):971–7.
9. AulC,GiagounidisA,GermingU.Epidemiologicalfeaturesof myelodysplasticsyndromes:resultsfromregionalcancer surveysandhospital-basedstatistics.IntJHematol. 2001;73(4):405–10.
10.DammF,KosmiderO,Gelsi-BoyerV,RennevilleA,Carbuccia N,Hidalgo-CurtisC,etal.MutationsaffectingmRNAsplicing definedistinctclinicalphenotypesandcorrelatewithpatient outcomeinmyelodysplasticsyndromes.Blood.
2012;119(14):3211–8.
11.PapaemmanuilE,CazzolaM,BoultwoodJ,MalcovatiL,VyasP, BowenD,etal.SomaticSF3B1mutationinmyelodysplasia withringsideroblasts.NEnglJMed.2011;365(15):1384–95.
12.VisconteV,MakishimaH,JankowskaA,SzpurkaH,TrainaF, JerezA,etal.SF3B1,asplicingfactorisfrequentlymutatedin refractoryanemiawithringsideroblasts.Leukemia.
2012;26(3):542–5.
13.MakishimaH,VisconteV,SakaguchiH,JankowskaAM,Abu KarS,JerezA,etal.Mutationsinthespliceosomemachinery, anovelandubiquitouspathwayinleukemogenesis.Blood. 2012;119(14):3203–10.
14.WahlMC,WillCL,LührmannR.Thespliceosome:design principlesofadynamicRNPmachine.Cell.
2009;136(4):701–18.
15.RossiD,BruscagginA,SpinaV,RasiS,KhiabanianH,Messina M,etal.MutationsoftheSF3B1splicingfactorinchronic lymphocyticleukemia:associationwithprogressionand fludarabine-refractoriness.Blood.2011;118(26):6904–8.
16.HahnCN,ScottHS.Spliceosomemutationsinhematopoietic malignancies.NatGenet.2011;44(1):9–10.
17.MalcovatiL,PapaemmanuilE,BowenDT,BoultwoodJ,Della PortaMG,PascuttoC,etal.ClinicalsignificanceofSF3B1 mutationsinmyelodysplasticsyndromesand
myelodysplastic/myeloproliferativeneoplasms.Blood. 2011;118(24):6239–46.
18.AdzhubeiIA,SchmidtS,PeshkinL,RamenskyVE,Gerasimova A,BorkP,etal.Amethodandserverforpredictingdamaging missensemutations.NatMethods.2010;7(4):248–9.
19.MalcovatiL,PapaemmanuilE,AmbaglioI,ElenaC,GallìA, DellaPortaMG,etal.Driversomaticmutationsidentify distinctdiseaseentitieswithinmyeloidneoplasmswith myelodysplasia.Blood.2014;124(9):1513–21.
20.BejarR,StevensonK,Abdel-WahabO,GaliliN,NilssonB, Garcia-ManeroG,etal.Clinicaleffectofpointmutationsin myelodysplasticsyndromes.NEnglJMed.
2011;364(26):2496–506.
21.YeH,RouaultTA.Erythropoiesisandironsulfurcluster biogenesis.AdvHematol.2010;2010.
22.PondarreC,CampagnaDR,AntiochosB,SikorskiL,Mulhern H,FlemingMD.Abcb7,thegeneresponsibleforX-linked sideroblasticanemiawithataxia,isessentialfor hematopoiesis.Blood.2007;109(8):3567–9.
23.CazzolaM,InvernizziR,BergamaschiG,LeviS,CorsiB, TravaglinoE,etal.Mitochondrialferritinexpressionin erythroidcellsfrompatientswithsideroblasticanemia. Blood.2003;101(5):1996–2000.
24.TehranchiR,InvernizziR,GrandienA,ZhivotovskyB,Fadeel B,ForsblomAM,etal.Aberrantmitochondrialiron
distributionandmaturationarrestcharacterizeearly erythroidprecursorsinlow-riskmyelodysplasticsyndromes. Blood.2005;106(1):247–53.
25.NikpourM,ScharenbergC,LiuA,ConteS,KarimiM, Mortera-BlancoT,etal.ThetransporterABCB7isamediator ofthephenotypeofacquiredrefractoryanemiawithring sideroblasts.Leukemia.2013;27(4):889–96.
26.VisconteV,RogersHJ,SinghJ,BarnardJ,BupathiM,TrainaF, etal.SF3B1haploinsufficiencyleadstoformationofring sideroblastsinmyelodysplasticsyndromes.Blood. 2012;120(16):3173–86.