SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Acetabular
revision
in
total
hip
arthroplasty
with
tantalum
augmentation
and
lyophilized
bovine
xenograft
夽
Cristiano
Valter
Diesel
a,
Tiango
Aguiar
Ribeiro
b,
Marcelo
Reuwsaat
Guimarães
a,
Carlos
Alberto
de
Souza
Macedo
c,
Carlos
Roberto
Galia
a,c,∗aUniversidadeFederaldoRioGrandedoSul(UFRGS),ProgramadePós-Graduac¸ãoemMedicinaCiênciasCirúrgicas,PortoAlegre,RS,
Brazil
bUniversidadeFederaldeSantaMaria(UFSM),DepartamentodeCirurgia,Servic¸odeOrtopediaeTraumatologiadoHospital
UniversitáriodeSantaMaria(SOT-HUSM),SantaMaria,RS,Brazil
cUniversidadeFederaldoRioGrandedoSul(UFRGS),FaculdadedeMedicina(FAMED),HospitaldeClínicasdePortoAlegre(HCPA),
PortoAlegre,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received9December2016 Accepted26January2017 Availableonline23August2017
Keywords: Hiparthroplasty Bonetransplantation Surgicalinstruments Acetabulum Trabecularmetal Tantalum
a
b
s
t
r
a
c
t
Objective:Toevaluateamixedtechniqueofacetabularreconstruction,whichusestrabecular metalintheformoftantalumaugmentsassociatedwithlyophilizedbovinexenograft. Methods:Fifteenpatientswereevaluatedprospectively,whounderwentacetabular recon-structionwithimpactedlyophilizedbovinexenograftassociatedwiththeuseoftantalum augments.Themainoutcomewasthefailureofthetantalum–boneinterface.
Results:Thepopulationhadameanageof58.33years±14.27;themajoritywasfemale,80%. Ofthetotalsubjects,66.7%wereoperatedforfailureinprimaryarthroplasty.Themean follow-uptimewas45.2months±11.39.Thefailurerateofthemethodintheperiodand populationstudiedwas6.7%.
Conclusion:Anextremelyhighindex(93.3%)ofsuccesswasobservedinanaveragetimeof 45.2monthsoffollow-up.Datawerecomparabletocurrentliterature,demonstratingthat thetechniqueemployedandproposedisadequateforhipreconstructioninyoungpatients. ©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedatHospitaldeClínicasdePortoAlegre(HCPA),PortoAlegre,RS,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](C.R.Galia). http://dx.doi.org/10.1016/j.rboe.2017.08.009
rev bras ortop.2017;52(S1):46–51
47
Revisão
acetabular
em
artroplastia
total
de
quadril
com
cunhas
de
tântalo
associadas
a
enxerto
ósseo
bovino
liofilizado
Palavras-chave: Artroplastiadequadril Transplanteósseo Instrumentoscirúrgicos Acetábulo
Metaltrabecular Tântalo
r
e
s
u
m
o
Objetivo:Avaliarumatécnicamistadereconstruc¸ãoacetabularqueusametaltrabecularna formadecunhasdetântaloassociadascomenxertoósseobovinoliofilizado.
Métodos: Foram avaliados prospectivamente 15 pacientes submetidos à reconstruc¸ão acetabularcomenxertobovinoliofilizadoimpactadoassociadoaousodecunhasdetântalo. Oprincipaldesfechoavaliadofoiafalhadainterfacetântalo-osso.
Resultados: Apopulac¸ãoapresentouidademédiade58,33anos±14,27,amaioriadosexo feminino80%.Dototal,66,7%foramoperadosporfalhadaartroplastiaprimária.Otempo médiodeseguimentofoide45,2meses±11,39meses.Ataxadefalhadométodonoperíodo enapopulac¸ãoestudadafoide6,7%.
Conclusão: Observou-seumíndiceextremamenteelevado(93,3%)desucessoemumtempo médiode45,2mesesdeseguimento.Osdadossãocomparáveisàliteraturacorrente,oque demonstraqueatécnicaempregadaepropostaéadequadaparareconstruc¸ãodequadril empacientesjovens.
©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Withtheincreasingnumberofhiparthroplastiesperformed
worldwide, a likely proportional increase in the number
of arthroplasty revisions is expected.1 The term revision
suggests the simple inspection or discrete adjustment of
arthroplasty, andunderestimates theactual scope ofthese procedures.Mostofthesecasespresentseverebonedefects,
which require large reconstructions of the bone structure
aboutthehip,especiallytheacetabulum.
Severaltechniquescanbeusedforacetabular reconstruc-tion.AmongthemostcommontechniquesistheuseofJumbo cups,2reconstructionsthatuse structuralhomologousgraft (allograft)3 orimpacted morselized homologous graft, with orwithoutgraftprotectiondevicessuchasontherenowned technique described bySlooff et al.4 The use ofautograft, althoughbiologicallyconsideredideal,isnotpossibleinmost casesduetoitsinsufficientamountandtheneedforanother procedure,whichisnotriskfree.
Otherbonesubstitutealternativesaregraftsderivedfrom speciesotherthanhuman(xenograft);thoseofbovineorigin arethemostroutinelyused.5 Toavoidimmunological reac-tionsintherecipientarea,animalbonegraftsarepreparedin variouswaysinordertoeliminateorminimizetheir antigenic-ity.Onesuchmannerislyophilization,theprocessinwhich theboneisdegreased,decellularized,andultimately steril-ized.Regardlessoftheseveralmanufacturingprotocols,the finalproductshouldmaintainitspotentialfor osseointegra-tionandosteoinduction,aswellasbeingphysicochemically similartohumanbone.6,7
Inthepasttenyears,theuseoftrabecularmetalhasgained groundinhipreconstructions.Thesemetalstructuresare pro-ducedusingcutting-edgetechnologyandmadeoftitaniumor tantalum;theyseektoimitatethebonemicrostructure,with porositiesbetween400and600microns,whichtheoretically facilitatestheirintegrationintothehostbone.8,9
Reconstructions using large grafts, whether autologous, homologous,orxenologousarethosewiththehighestnumber offailures.10Moreover,thetypeofacetabulardefectalso influ-encesthesuccessofthereconstruction.Defectsconsideredas contained,i.e.thoseinwhichtheacetabularstructure(walls, roof,andfloor)ispreserved,aremorelikelytohavegood per-formancewhencomparedwithseveresegmentaldefects(loss ofwallsandespeciallylossofacetabularroof)11orthosewith pelvicdiscontinuity.12
Theauthorsbelievethat,wheneverpossible,boneshould bereplacedbybone,especiallyinyoungindividuals.Despite thisreconstructionphilosophy,failuresareobserved, particu-larlyinseveredefects,especiallythoseinvolvingthelossofthe acetabularroof11andwhencombinedwiththeneedforalarge
amount ofgraft.Thus,encouraged bythestudy byGerhke
etal.,13theauthorsdecidedtostudyatechniquethat com-binestheuseoftrabecularmetalintheareaofhighershearing force(acetabularroof),associatedwiththeuseofgraft, replac-ingthefillingoftheremainingdefectswithlyophilizedbovine (insteadofhuman)bonegraft.
Material
and
methods
Thiswasaprospectivecohortstudyconductedfrom Septem-ber2011toNovember2016.Theprojectwasapprovedbythe ResearchEthicsCommitteeoftheinstitutionandregistered undernumber15.0248;theethicalpreceptsoftheDeclaration ofHelsinkiof1975werefollowed.
Thestudyincludedpatientswithacetabularroofdefectin whomlargegraftswereexpectedtobenecessaryfor recon-struction.Patientswhohadoneormorefailuresinprevious acetabularreconstructionswerealsoincluded.
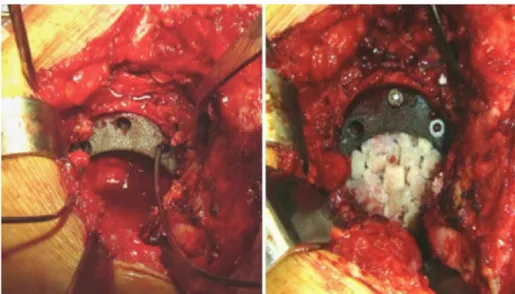
Fig.1–Ontheleft,provisionalpositioningofthetantalumaugmentwithKirschnerwires.Ontheright,positioningand definitivefixationofthewedge,followedbycavityfillingwithlyophilizedbovinebonegraft.
Fig.2–Pre-andpostoperativeradiographyofanarthroplastyreconstructioninapatientwithacetabulardefectclassifiedas d’AntoniotypeIII.Reconstructionplate,tantalumwedge,lyophilizedbovinebonegraft,andacetabularfloormeshwere used.
tod’AntonioapudvanHaarenetal.,10basedonradiographic images;patientswerereclassifiedintraoperativelywhen nec-essary.
After this stage, the acetabular reconstruction was
ini-tiated from the roof;the tantalum wedge(Zimmer Biomet
Holding,Inc.) waschosenaccording tothecomponent test
piece. The wedge was fixed with two or three screws, in
themoststableposition.Then,lyophilizedbovinebonegraft
(Orthogen-Baumer) was morselizedand impacted withthe
useofimpactorsorwithreversepositionreaming. Depend-ing on the severity of the acetabulardefect, other devices wereadded,suchasanacetabularreinforcementring,pelvic reconstruction plates,or acetabularmeshes. Subsequently, theacetabularcomponentZCA(ZimmerBiometHolding,Inc.)
orDelta(Baumer)wascemented(CementSimplex–
Howmed-ica)inaccordancetothestandardtechnique(Figs.1and2). The same antimicrobial prophylaxis (cefazolin, weight-adjusteddose)andthesameprophylaxisforthromboembolic events (enoxaparin) was adopted for all patients. At least
six culture samples were collected in all cases. In cases
of suspected septic loosening, the protocol of choice was
one-stage revision; broad-spectrum intravenous antibiotics (vancomycinandcefepime)wereusedaftercollectionof intra-operativeculturematerial.Theseantibioticsweremaintained forapproximately15days,untilthecultureresultsdescribed themicrobialprofile.Then,theantibioticswerewithdrawnby theinfectologyteamofthishospital.
Data regardinggender,age, andprevious surgeries were analyzed. Acetabular defects were classified preoperatively andintraoperativelybythed’Antonioclassification(AAOS).10 Radiographically, thefollowingaspectswere usedtodefine thepresenceoflooseningoftheacetabularcomponentandof thewedgeinthepost-operativeperiod:presenceof radiolu-centlines(apudDeLeeandCharnley)anddisplacementofthe
wedgeoracetabularcomponent.
Statistical
analysis
rev bras ortop.2017;52(S1):46–51
49
comparethemeansofnormalquantitativevariablesbetween genders,theANOVAtestwasused;toverifythe homogene-itybetweenthegroups,theLevinetestwasused.Alevelof significanceof5%(p≤0.05)wasadopted.
Results
Fifteenpatientsunderwentthedescribedsurgicaltechnique. Themeanagewas58.33±14.27years(mean±standard devi-ation),rangingfrom39to81.Mostpatientswerefemale(12; 80%).Nodifferenceswereobservedbetweengenders(p=0.96), andthegroupswereconsideredhomogeneous(p=0.04).
Ofthis total, 66.7% (ten) ofthe patients were operated forprimaryarthroplastyfailure;26.7%(four)hadpreviously
undergone one or more hip reconstructions, and one had
undergonetheGirdlestonesurgery.
AsfortheclassificationoftheAAOS,typeIII(mixed)defect wasthemostprevalent,beingidentifiedin86.7%(13)patients. Pelvicdiscontinuity(typeIVdefect)wasdetectedinonly13.3% (two) ofthe patients. Six reconstructionsrequired associa-tionwithother orthopedicdevices,suchasacetabularfloor meshes,reinforcementrings,or acetabulumreconstruction plates.OthersamplecharacteristicsaredescribedinTable1.
Follow-upofonepatientfromtheinitialsamplewas
ter-minated due to death caused by complications of a liver
transplantation that occurred two years after hip surgery. Untilthelastfollow-upvisit,thispatient’sreconstructionwas intact,withoutfailure.
The mean follow-up was 45.2±11.39 months
(mean±standarddeviation),rangingfrom14to63.
Discussion
A6.7%failurerate(onecase)wasobserved;therefore,the suc-cessratewashigh,correspondingto93.3%inameanfollow-up of45.2months.
Totalhiparthroplastywasconsideredthesurgeryofthe century.14 Due to its success in relieving pain in patients withhiposteoarthritis,ithasbecomeacceptedand dissemi-natedworldwide.Asadirectconsequenceoftheincreasein thenumberofarthroplasties,anincreaseintherateof revi-sions(reconstructions)duetolooseningwasobserved.1This increaseisusuallyaccompaniedbyahigherseverityofbone defects–especiallyacetabular–andmoreparticularlyin insti-tutionalizedpatients.
Over the years, several reconstruction techniques have beenproposed.Casesinwhichbonedefectswerefilledonly withorthopediccementwereevaluated.Casesofsuccessful implantationofjumbocupswerefollowed-up,aswellasthe resultsofthereconstructionsusingstructuralhomograft.The authorshave subscribedtothe schoolofacetabular recon-structionwithimpactedmorselizedgraftdevelopedbySlooff etal.4andadoptedbytheschoolofExeter.
Oursuccessratewassimilartoresultsreportedinthe lit-eraturewiththetechniqueofimpactedgraft.Alsoaccording totheliterature,itwasobservedthatlargegraftsweremore pronetofailures,especiallywhenassociatedtomajordefects oftheacetabularrooforpelvicdiscontinuity.11,12
In the last ten years, metal implants with
similar-to-bone microstructure have been developed, manufactured,
and commercialized with a high success rate in hip
reconstructions.9,15,16 Although bone substitution with tra-becularmetalappearstobeapromisingoption,itdoesnot reconstructthebonestockapatientwhoissometimesyoung
and may requireanewhip replacement.Thisfact
encour-agedtheauthorstocontinuetosearchforoptionsthatwould increasesuccessratesandpromotethereconstructionofpart ofthebonestock.
Given the need for and the unavailability of adequate
amounts of homologous graft, for 20 years the authors
havebeendevelopingresearchprojectsfortheproductionof lyophilized bovinebone graft.The resultwas afinal prod-uctwithphysicochemicalcharacteristicssimilartothoseof humanbone,6,7 presentingabiological potentialand being easytoobtain.17Afterover16yearsoffollowing-uppatients whoreceivedthisgraft,itsusehasbecomecommonplacein theinstitution.18
Fewarticlesintheliteraturehaveassessedthetechnical
combinationofaugmentationwedgesandbonegraft.Gehrke
etal.13usedwedgesassociatedwithhomologousbonegraft in46 cases.Theyobserved agoodevolution in44ofthese patients,inameanfollow-upof46months.
Visually,whenthetantalumacetabulumiscomparedwith tantalum wedges,thereisclearlyasmallercontactsurface betweentheimplantandthehostbone.Thisfactorhasraised concernaboutitsosseointegrationcapacity,aswellasits sta-bility.Incaseswithlateralcoveragedeficiency,thetantalum wedgecouldundergoagreatshearforce,similartothegraft.11 Inthesecases,orinthosewithmedialwallloss,protection deviceswereusedinadditiontothebonegraft,suchas Ker-boullacetabularreinforcement,reconstructionplates,and/or acetabularreconstructionmeshes.
In cases where the acetabulum adopts an oblong
mor-phology, there is usually a need for reconstruction of the roof and loweringofthe joint’s centerof rotation. Insuch cases,althoughtheliteraturesuggeststheuseofjumbocups
intrabecularmetal,withorwithoutaugmentationwedges,
the authors believe that a more biological reconstruction
ispossible, especiallyseekingthe restitutionofbonestock
inyoung patients, inwhom futurereconstructionsmay be
necessary.
Thepresentresults,albeitwithasmallsample,aresimilar tothoseofGehrkeetal.,13evenregardingthemeanfollow-up time.Todate,onlyoneisolatedreleaseoftheacetabular com-ponentthatrequiredfurthersurgeryhasbeenobservedinthis sample.Inthatcase,however,thetantalumwedgeremained fixatedatitsoriginalsite.Theauthorsbelievethatthisevent occurredduetotechnicalfailurecausedbyinsufficient cover-ageoftheacetabularcomponent.
Insixreconstructions,otherorthopedicdeviceswerealso used,suchasreconstructionplates,Kerboullacetabular rein-forcementrings,oracetabularreconstructionplates.Twoof thesereconstructionswereinpelvicdiscontinuities.Thegoal ofthesecombinationswastoreconstructtheacetabularfloor ortoassistwedgefixation,especiallywhenscrewfixationwas notconsideredadequate.
r
e
v
b
r
a
s
o
r
t
o
p
.
2
0
1
7;
5
2(S
1)
:46–51
Table1–Samplecharacteristics.
Patient Age Gender Side Prior
surgery
Classification ofthe acetabular
defect
Surgerydate Wedge size
Acetabular size
Useofother devices
Presenceof radiolucency atfollow-up
Presenceof migrationat follow-up
MZFS 81 F R THA III May7,2012 58×20 47×28 No No
AL 54 F R THA III April19,2012 54×10 43×22 No No
JEC 54 M L THA III October3,2012 58×10 53×32 No No
OPB 80 F R THA III March21,2013 54×15 55×28 No No
FA 54 F R THA III February27,2013 50×10 51×28 No No
NJOA 76 F R THA III April1,2013 58×10 49×28 Reconstruction
plate
No No
LSC 77 F L THA III September28,2014 62×10 49×32 No No
JACCT 63 M R THA IV March18,2013 54×20 47×28 Reconstruction
cage
No No
OCF 57 M R RTHA(3) III September5,2011 66×20 47×28 No No
DW 39 F R RTHA III October29,2012 54×15 51×28 Reconstruction
plate
No No
LMC 41 F L RTHA(2) III June2,2014 54×10 51×28 Reconstruction
mesh
Yes Yes
GMSP 53 F L Girdlestone III October8,2012 58×20 51×28 Reconstruction
mesh
No No
ATVP 40 F L RTHA IV November26,2012 58×20 55×28 Reconstruction
plate+mesh
No No
IS 57 F R THA III December18,2012 50×15 46×28 No No
EMS 49 F L THA III July20,2013 54×14 46×28 No No
rev bras ortop.2017;52(S1):46–51
51
looseningandreconstructionfailure.Nootherpatient under-wentfurthersurgeryexclusivelyduetoaugmentationwedge failure.Moreover,nocasesofacuteinfectionor caseswith intermediate infection signs were observed in any patient operatedwiththistechnique.
Thepreliminaryresultsare encouraging.Ahigh success
ratewasobservedinameanfollow-uptimethatis
compa-rabletothecurrentliterature.Nonetheless,theseresultsare stillearlyandrequireagreatersamplesize.However, recon-structionusingtantalumaugmentassociatedwithbonegraft (xenologousorhomologous)appearstobeapromisingoption foryoungpatientswithassociatedpartiallossofthe acetabu-larroof.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. DixonT,ShawM,EbrahimS,DieppeP.Trendsinhipandknee jointreplacement:socioeconomicinequalitiesand
projectionsofneed.AnnRheumDis.2004;63(7):825–30. 2. VonRothP,AbdelMP,HarmsenWS,BerryDJ.Uncemented
jumbocupsforrevisiontotalhiparthroplasty:aconcise follow-up,atameanoftwentyyears,ofapreviousreport.J BoneJointSurgAm.2015;97(4):284–7.
3. GarbuzD,MorsiE,GrossAE.Revisionoftheacetabular componentofatotalhiparthroplastywithamassive structuralallograftstudywithaminimumfive-year follow-up.JBoneJointSurgAm.1996;78(5):693–7.
4. SlooffTJ,SchimmelJW,BumaP.Cementedfixationwithbone grafts.OrthopClinNorthAm.1993;24(4):667–77.
5. LevaiJP,BoisgardS.Acetabularreconstructionintotalhip revisionusingabonegraftsubstitute.Earlyclinicaland radiographicresults.ClinOrthopRelatRes.1996;(330):108–14. 6. GaliaCR,Lourenc¸oAL,RositoR,SouzaMacedoCA,Camargo
LM.Physicochemicalcharacterizationoflyophilizedbovine bonegrafts.RevBrasOrtop.2015;46(4):444–51.
7.GaliaCR,MacedoCA,RositoR,MelloTM,CamargoLM, MoreiraLF.Invitroandinvivoevaluationoflyophilized bovinebonebiocompatibility.Clinics(SãoPaulo). 2008;63(6):801–6.
8.IssackPS.Useofporoustantalumforacetabular
reconstructioninrevisionhiparthroplasty.JBoneJointSurg Am.2013;95(21):1981–7.
9.FlecherX,AppyB,ParratteS,OllivierM,ArgensonJN.Useof poroustantalumcomponentsinPaproskytwoandthree acetabularrevision.Aminimumfive-yearfollow-upoffifty onehips.IntOrthop.2017;41(5):911–6.
10.VanHaarenEH,HeyligersIC,AlexanderFG,WuismanPI.High rateoffailureofimpactiongraftinginlargeacetabular defects.JBoneJointSurgBr.2007;89(3):296–300.
11.García-ReyE,MaderoR,García-CimbreloE.THArevisions usingimpactionallograftingwithmeshisdurableformedial butnotlateralacetabulardefects.ClinOrthopRelatRes. 2015;473(12):3882–91.
12.García-CimbreloE,García-ReyE.Bonedefectdetermines acetabularrevisionsurgery.HipInt.2014;24Suppl.10:S33–6. 13.GehrkeT,BangertY,SchwantesB,GebauerM,KendoffD.
AcetabularrevisioninTHAusingtantalumaugments combinedwithimpactionbonegrafting.HipInt. 2013;23(4):359–65.
14.LearmonthID,YoungC,RorabeckC.Theoperationofthe century:totalhipreplacement.Lancet.
2007;370(9597):1508–19.
15.DelGaizoDJ,KancherlaV,SporerSM,PaproskyWG.Tantalum augmentsforPaproskyIIIAdefectsremainstableatmidterm followup.ClinOrthopRelatRes.2012;470(2):395–401. 16.FlecherX,PaproskyW,GrilloJC,AubaniacJM,ArgensonJN.
Dotantalumcomponentsprovideadequateprimaryfixation inallacetabularrevisions?OrthopTraumatolSurgRes. 2010;96(3):235–41.
17.RibeiroTA,CoussiratC,PagnussatoF,DieselCV,MacedoFC, MacedoCA,etal.Lyophilizedxenograft:acaseseriesof histologicalanalysisofbiopsies.CellTissueBank. 2015;16(2):227–33.