www.jped.com.br
ORIGINAL
ARTICLE
Treatment
of
Bartter
syndrome.
Unsolved
issue
夽
,
夽夽
Carla
Lessa
Pena
Nascimento
a,
Cecilia
Lopes
Garcia
a,
Benita
Galassi
Soares
Schvartsman
a,b,
Maria
Helena
Vaisbich
a,c,∗aUnidadedeNefrologia,InstitutodaCrianc¸a,HospitaldasClínicas,FaculdadedeMedicina,
UniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
bFaculdadedeMedicina,UniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
cUniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
Received17September2013;accepted28January2014 Availableonline27May2014
KEYWORDS Barttersyndrome; Non-steroidal anti-inflammatory drug;
Enalapril; Proteinuria
Abstract
Objective: Todescribetheresultsofalong-termfollow-upofBarttersyndromepatientstreated withdifferentdrugs.
Method: Patientswerediagnosedaccordingtoclinicalandlaboratorydata.Treatmentprotocol waspotassiumsupplementation,sodium,spironolactone,andnon-steroidalanti-inflammatory drug.Patientswhodevelopedproteinuriawere convertedtoangiotensinconversionenzyme inhibitor.ThevariablesevaluatedforeachdrugwereZ-scoreforweightandstature, protein-uria,creatinineclearance,gastrointestinalcomplaints,amountofpotassiumsupplementation, serumpotassiumandbicarbonatelevels,andfindingsofupperdigestiveendoscopy.
Results: 20 patients were included. Follow-up was 10.1 ± 5.2 years.17 patients received indomethacinfor5.9±5.3years;19receivedcelecoxib,medianof35months;andfivereceived enalapril,medianof23months.Duringindomethacin,astatisticallysignificantincreasewas observedintheZ-scoreforstatureandweight,withoutachangeinthecreatinineclearance. Sevenof17patientshadgastrointestinalsymptoms,andupperdigestiveendoscopyevidenced gastritisinthreepatientsandgastriculcerinfourpatients.Duringcelecoxibuse,asignificant increasewasdetectedintheZ-scoreforstatureandweightandareductionofhyperfiltration; sevenpatientspresentedgastrointestinalsymptoms,andupperdigestiveendoscopyevidenced mildgastritisinthree. Duringenalapril use,nosignificantchanges wereobservedinthe Z-scoreforstature,weightandcreatinineclearance.Theconversiontoenalaprilresultedina significantreductioninproteinuria.
夽 Pleasecitethisarticleas:NascimentoCL,GarciaCL,SchvartsmanBG,VaisbichMH.TreatmentofBarttersyndrome.Unsolvedissue.J
Pediatr(RioJ).2014;90:512---7.
夽夽
StudyconductedatUnidadedeNefrologia,InstitutodaCrianc¸a,HospitaldasClínicas,FaculdadedeMedicina,UniversidadedeSão Paulo(HCFMUSP),SãoPaulo,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](M.H.Vaisbich). http://dx.doi.org/10.1016/j.jped.2014.01.012
Conclusion: Theauthorssuggeststartingthetreatmentwithcelecoxib,andreplacingbyACEi if necessary,monitoringtherenalfunction.The safetyandefficacyofcelecoxibneedtobe assessedinlargercontrolledstudies.
©2014SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE SíndromedeBartter; Medicamento anti-inflamatórionão esteroide;
Enalapril; Proteinúria
TratamentodasíndromedeBartter.Problemanãoresolvido
Resumo
Objetivo: Descreverosresultadosdeumacompanhamentodelongoprazodepacientescom síndromedeBarttertratadoscomdiferentesmedicamentos.
Método: Pacientesdiagnosticadossegundoosdadosclínicoselaboratoriais.Protocolode trata-mento:suplementac¸ãodepotássio, sódio,espironolactona emedicamentoanti-inflamatório nãoesteroidal.Ospacientesquedesenvolveramproteinúriaforamsubmetidosainibidorda enz-imadeconversãodaangiotensina.Asvariáveisavaliadasduranteousodecadamedicamento foram:escoreZparapesoeestatura,proteinúria,depurac¸ãodacreatinina,queixas gastroin-testinais,quantidadedasuplementac¸ãodepotássio,níveisséricosdepotássioebicarbonatoe achadosdaendoscopiadigestivaalta.
Resultados: Foramincluídos20pacientes.Oacompanhamentofoide10,1±5,2anos.Nototal, 17pacientesreceberamindometacinapor5,9±5,3anos,19receberamcelecoxibpor aproxi-madamente35mesesecincoreceberamenalaprilporaproximadamente23meses.Duranteo usodeindometacina,observamosumaumentoestatísticosignificativonoescoreZparaestatura epeso,semalterac¸ãonadepurac¸ãodacreatinina.7/17pacientesapresentaramsintomas gas-trointestinais,eaendoscopiadigestivaaltamostrougastriteemtrêspacienteseúlceragástrica emquatro.Duranteousodecelecoxib,detectamosumaumentosignificativonoescoreZpara estaturaepesoeumareduc¸ãodahiperfiltrac¸ão;setepacientesapresentaramsintomas gas-trointestinaiseaendoscopiadigestivaaltamostrougastriteleveemtrêspacientes.Durante ousodeenalapril,nãoobservamosalterac¸õessignificativasnoescoreZparaestatura,peso edepurac¸ãodacreatinina.Amudanc¸adamedicac¸ãoparaenalaprilresultouemumareduc¸ão significativanaproteinúria.
Conclusão: Sugerimosiniciarotratamentocomcelecoxibe,casonecessário,substituí-lopor ACEi,monitorandoafunc¸ãorenal.Aseguranc¸aeaeficáciadocelecoxibprecisamser compro-vadascomgrandesestudoscontrolados.
©2014SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Barttersyndrome(BS)encompassesagroupofraregenetic, autosomal recessive, renal tubular diseases characte-rized by urinaryloss of sodium, potassium, and chloride; hypokalemicmetabolicalkalosis;highplasmalevelsofrenin and aldosterone; and high levels of prostaglandins (PGs) in bloodand urineasa secondary phenomenon.Clinically patientspresentpolyuria,polydipsia,failuretothrive, life-threateningepisodesofdehydration,episodesoffever,and normalorlowbloodpressure.Frequently,pediatriciansare thefirstprofessionalstoattendtothesepatientsanditis therefore important to be aware of this condition, since prognosis is better with earlier diagnosis and treatment. TherearedifferenttypesofBS,andclinicaland laborato-rial variability dependson the affected tubularcarrier.1,2
Accordingtotheaffectedregion,somedifferencescanbe observedin themanagementofthe disease,forinstance, typeIIBSisassociatedwithverymildhypokalemia,whereas in type IV BS, treatment with indomethacin is muchless effective.3
Thepresentstudyaimedtodescribetheresultsofa long-termfollow-upofBSpatientstreatedwithdifferentdrugs.
Patients
and
methods
Thisretrospective study,basedona prospectiveprotocol, enrolled patients with clinical and laboratorial diagnosis of BS from 1993 until 2012, and adherent to the treat-ment,whichwasevaluatedbyadherencetoscheduledclinic appointmentsandserumbicarbonateandpotassiumlevels. Geneticanalysisisnotavailableinthisservice.
Treatmentprotocol
symptoms;4 and since 2003, it was decided to adopt a
selectiveNSAID(sNSAID), celecoxib,inordertoavoid gas-trointestinalcompromise.
Patientswhodevelopedproteinuriawereconvertedtoan angiotensinconversionenzymeinhibitor(ACEi),enalapril,in replacementtoNSAID.Thisconversionwasmadeduring hos-pitalization,sincepatientscanpotentiallydevelopserious hypotensionwithACEi.
Variables
The following variables were evaluatedduring treatment witheach drug:Z-score for weightand stature, glomeru-larfiltrationrate(GFR)throughcreatinineclearance(using Schwartz’sformula, sinceurinarycollection of24hoursis difficult, especially in polyuric patients),5 average
potas-siumsupplementation,andserumlevelsof potassiumand bicarbonate.The presenceof proteinuria,gastrointestinal (GI)complaints,andfindingsofupperdigestiveendoscopy (UDE)werealsoevaluated.
In this study, hyperfiltration wasdefined as creatinine clearance≥ 145mL/min/1.73m2BS (mL/min/1,73 m2Body Surface).6
Statisticalanalysis
Datawithhomogeneous distributionwere shown asmean andstandard deviation. All otherswere shown asmedian andrange.Student’st-testforpairedsampleswasemployed to compare variables with normal distribution, and the Wilcoxon test was used to compare non-normal distribu-tionvariables.Thelatterwasalsoemployedtocomparethe microalbuminurialevels beforeand after the substitution ofcelecoxibtoenalapril.Thechi-squaredtestwasusedto comparethefindingsinUDEinsymptomaticpatientsduring indomethacinandcelecoxibuse.
Thestudywasapprovedbylocalethicscommittee.
Results
Twentypatientswereincluded,ofwhom12werefemales. Follow-uptimewas10.1±5.2years,ageatdiagnosishad a median of 17.5 months (3---178) and at last evaluation was14.0 ± 5.3 years.Five patients were born from con-sanguineousparentsandtwopatientsweresiblings.Seven patients, five of whom females, presented with polyhy-dramnioand/orprematurity,characteristicsofneonatalBS. Neurosensorialdeafnesswasobservedintwopatients(one female),andtheyareclassifiedasBSwithdeafness.Eleven patientsshowedcharacteristicsofclassicBS.Nopatient pre-sentedwithhypocalciuria, thusexcluding thediagnosis of Gitelmansyndrome.
Periodofindomethacintreatment
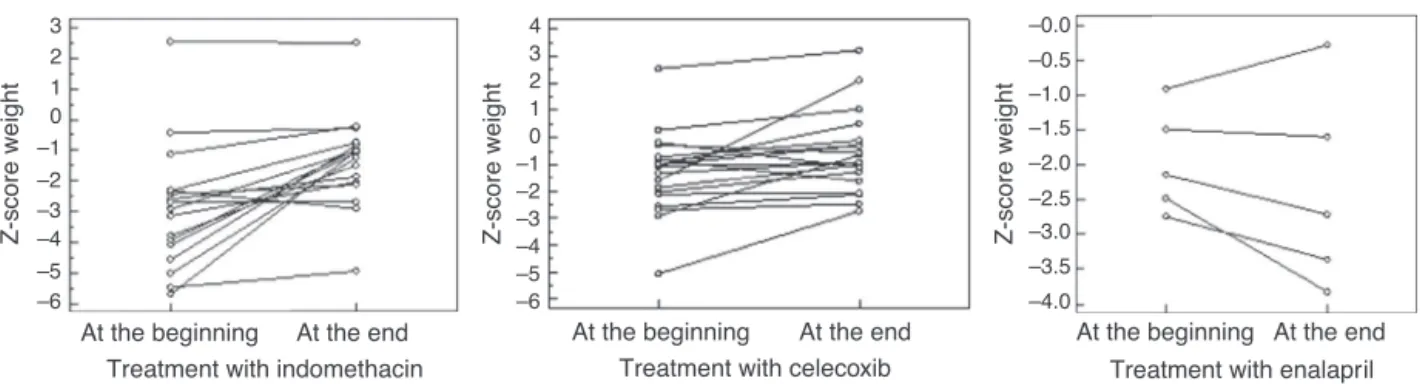
Seventeen patients received indomethacin for 5.9 ± 5.3 yearsinadosageof2.1± 0.6mg/Kg/daydividedinthree doses.Anincreasewasobservedinheight-for-ageZ-score, from-3.3± -2.1 to-2.2± 1.2 (p =0.01), andin weight-for-ageZ-score,frommedian=-2.9(-5.7---2.5)tomedian=
-1.05(-4.9-2.5)(p=0.0004),withoutasignificantchangein thecreatinineclearance,whichvariedfrommedian =105 (64-277) tomedian =144 (71-279)mL/min/1.73m2BS(p = 0.34);andwithmetabolicandelectrolytestability.However, fourpatientshadhyperfiltrationatthebeginningandeight presentedhyperfiltrationattheendofthetreatment.Seven of17patientshadGIsymptoms,andUDEevidencedgastritis inthreecasesandgastriculcer,aseverefinding,infour.
Periodofselectiveprostaglandininhibitor
Nineteen patients received celecoxib,during a median of 35months(8-144).Anincreasewasobservedin height-for-ageZ-scorefrom-2.4±-1.7to1.8±1.3(p=0.02)andin weight-for-ageZ-scorefrom-1.3± 1.5to-0.81±1.2(p= 0.01),aswell asareductionin creatinineclearancefrom 147 ± 52to 119 ± 31mL/min/1.73m2BS (p = 0.04). Nine patientspresentedwithhyperfiltrationatthebeginningof treatment;attheend,hyperfiltrationwasdetectedinonly twopatients.Sevenof19patientspresentedGIsymptoms, butUDEevidencedmildgastritisinthreecasesandnocase ofulcer.
Comparing indomethacin with celecoxib, positive find-ings in UDE were more present in indomethacin group, althoughnotsignificant(p=0.06);however,indomethacin wasassociated withmore severe compromise.During the treatment with celecoxib, no patient developed gastric ulcer.
PeriodofACEitreatment
Fivepatientsreceivedenalaprilbymedianof23months (3-80) in a dosage of 0.2 ± 0.1mg/kg/d,ym divided in two doses, despite we have tried in 6; one patientpresented severe hypotension and the drug was withdrawn. No sig-nificant changes were observed in height-for-age Z-score (medianatthebeginningoftreatment=-2.5[-4.3to-2.2]; medianattheend=-3.0[-3.9to-1.21];p=0.8),norinthe weight-for-age Z-score(median at thebeginning of treat-ment=-2.1[-2.7to-0.9];medianattheend=-2.7[-3.8to -0.3];p=0.4).Thecreatinineclearanceshowedno statisti-callysignificantdifferences,frommedian150(107-183)to 138(62-160)(p=0.18);however,adecreasewasobserved infourpatients,oneofwhombelow90mL/min/1.73m2BS. Inthiscase,thedoseofenalaprilwasreduced.
Fig.1presentstheweight-for-ageZ-score,Fig.2shows theheight-for-ageZ-scoreatthebeginningandattheendof thetreatmentwitheachdrug.Fig.3presentsthecreatinine clearanceduringthetreatmentwitheachdrug.
Proteinuriaduringeachdrug
Seven patients developed microalbuminuria during treat-ment with indomethacin; in five patients, the problem resolvedwhentheirtreatmentwasconvertedtocelecoxib; however,fourpatientsdevelopedmicroalbuminuriaduring the use of celecoxib. Patients with proteinuria had their treatment convertedtoACEi, and presented a significant reduction:medianwas76.2%(62.8%-80.6%).
3 2 1 0 –1 –2 –3 –4 –5
Z-score weight
At the beginning
Treatment with indomethacin
At the end At the beginning
Treatment with celecoxib
At the end At the beginning
Treatment with enalapril At the end –6
4 3 2 1 0 –1 –2 –3 –4 –5
Z-score weight
–6
Z-score weight
–4.0 –3.0 –2.0 –1.0
–3.5 –2.5 –1.5 –0.5 –0.0
Figure1 Z-scoreforweightatthebeginningandattheendofthetreatmentwithdifferentmedications.Barsrepresent95%CI (confidenceinterval).
1 0 –1 –2 –3 –4 –5
Z-score stature Z-score stature Z-score stature
At the beginning
Treatment with indomethacin At the end –7
–6
1 0 –1 –2 –3 –4 –5
–7 –6
At the beginning
Treatment with celecoxib
At the end At the beginning
Treatment with enalapril At the end –4.0
–4.5 –3.0 –2.0 –1.0
–3.5 –2.5 –1.5
Figure2 Z-scoreforheightatthebeginningandattheendofthetreatmentwithdifferentmedications.Barsrepresent95%CI.
Creatinine clearance (ml/min/1.73m
2BS)
Creatinine clearance (ml/min/1.73m
2BS)
Creatinine clearance (ml/min/1.73m
2BS)
At the beginning
Treatment with indomethacin (n = 17)
At the end At the beginning
Treatment with celecoxib (n = 19)
At the end At the beginning
Treatment with enalapril (n = 5) At the end
0 30 60 90 120 150 180
0 30 60 90 120 150 180
0 30 60 90 120 150 180 210
Figure3 CreatinineclearanceaccordingtoSchwartz’sformulaofBarttersyndromepatients,atthebeginningandattheendof treatmentwitheachmedication.Barsrepresent95%CI.
Table1 Serumpotassium,sodium,bicarbonate,andpotassiumsupplementationin20Barttersyndromepatientsduring dif-ferentschedulesoftreatment.
Variables Indomethacin SelectiveNSAIDS ACEi Serumpotassium
mEq/L(median±SD)
3.3±0.4 3.5±0.4 3.5±0.2
Serumsodium
mEq/L(median±SD)
138±3 138±2 137±3
Serumbicarbonate(median±SD) 26.7±1.7 26.8±2.1 25.4±1.8 Potassiumsupplementation
mEq/kg/day(median±SD)
6.6±3.2 6.8±4.4 11.0±4.6
amountofpotassiumsupplementationincludingdatafrom eachsixmonths.Nosignificant differenceswereobserved inserumpotassium,sodium,andbicarbonatelevelsduring theuseofthethreedrugs.Nosignificantdifferenceswere observedbetween theamount ofpotassium supplementa-tionduringtheuseofindomethacinandcelecoxib(p=0.8). Although no significant differences were detected in the amountofpotassiumsupplementationduringindomethacin andACEi(p=0.09)andcelecoxibandACEi(p=0.2),a ten-dencytosupplement alargeramountof potassiumduring ACEiwasobserved,asseeninTable1.
Discussion
InBS, an over activation ofrenin-angiotensin-aldosterone system (RAAS) and an over production of PGs can be observed. Those findings are the result of sodium, chlo-ride, and potassium urinary wasting. Therefore, the recommendedtreatmenthasbeenbasedonpotassium sup-plementation,aPGsinhibitor;7,8spironolactone1 isalsoan
option,butwithtransienteffect,andACEihasbeenusedin somestudies.9
Indomethacin has been long employed in the treat-ment of these patients. Studies have demonstrated that withindomethacin,spironolactone,andpotassiumchloride supplementationand,sometimes,sodiumchloride supple-mentation, patients experience improvement in growth speed, weight gain, and metabolic stability.10 However,
therearesignificantGIeffectsresultingfrominhibitionof cyclooxygenase(Cox)1.4Thesedataareinaccordancewith
thepresentfindingsduringtheuseofindomethacin.4Asan
option, selective inhibitors of Cox (Cox-2 inhibitors more thanCox-1,suchascelecoxib)havebeenemployed, seek-ingarenaleffect,withreductionofundesirableGIeffects.11
ThemajorityofstudieshaveobservedthatsNSAIDsare asso-ciatedwitha lower risk of ulcers andcomplications than nsNSAIDs.12Inthepresentstudy,celecoxibpromoteda
bet-tercompliancetothetreatmentandareductioninsevere GI involvement (such as gastric ulcers), with metabolic andelectrolytestabilityandimprovementingrowthspeed and weight gain.4 In addition, celecoxib was associated
with a lower rate of hyperfiltration than indomethacin. Hyperfiltration is associated to focal glomerulosclerosis occurrence.
Thus,theuseof celecoxibcanbeagoodoption forBS patients, although larger studies are needed in order to proveitssafetyandefficacy.
Inthelastdecade,anincreaseincardiovascularevents has been observed during the use of COX-2 selective inhibitors.Those studieswere madein patients withhigh cardiovascularrisk, suchasthe elderlyor those inuse of acetylsalicylicacid. Thereare few long-term trials evalu-atingcardiovascularsafetyofcelecoxib,butnoconclusion can be drawn.13,14 The balance between the production
ofprostacyclinandthromboxane is thoughttoplaya role inregulationof plateletaggregationandin vasculartone. BSisassociatedwithoverproductionofprostaglandinsand thromboxane.15 It can thus be speculated that the
side-effecton cardiovascular system is not a risk factor in BS patients.However,nosuchwell-definedclinicaltrialshave beenconducted.
Long-termfollow-upofpatientsundertheuseofsNSAID has demonstrated that alongside its beneficial effect, patients can develop proteinuria, which is an aggravating totheprogressiontoend-stagerenaldisease.2Inthis
situ-atio,nanRAASinhibitorcanbeusedasareplacementdrug toNSAID. Few reports have been publishedonthe use of thesedrugs.16 Seyberth& Schlingmann2 statedthat ‘‘only
in the case of persistent hypokalemia (plasma potassium <3.0 mEq/L) that occurs despite adequate and tolerated inhibitionofprostaglandinsynthesisandsaltandpotassium supplementation,onemightconsidertheuseofdrugsthat interfere with the RAAS’’. However, close monitoring of renalfunctionandbloodpressureismandatory.This supple-mentaltherapymighthaveanadditionalbeneficialeffecton proteinuria.17
Inthepresentstudy,inpatientswhodeveloped protein-uria duringtreatment withcelecoxib,thereplacement by enalapril providedelectrolyte andmetabolicbalancewith significantreductionofproteinuria.Inaddition,good toler-anceandcompliancewereobservedwiththistreatment.It isnoteworthythattheadministrationofaninhibitorofRAAS inthesepatientscandetermineseverehypotension.Thus, therecommendationisthatthetransitionfromNSAIDtoa RAASinhibitorshouldbeperformedinthehospitalsetting, undermedicalsupervision.
NSAIDs,bothindomethacinandcelecoxib,areeffective in treating BS. The latter has demonstrated benefits on severityofGItractinvolvementanddecreasingin hyperfil-tration.However,thesafetyprofileofcelecoxibmay,inthe future,allowforitsuseasfirstdrugforthetreatmentofBS. Inpatientswhodevelopproteinuria,enalaprilwaseffective inreducingit.Thus,itissuggestedtostart thetreatment withcelecoxibandifnecessaryreplacingitbyACEi.
Thisstudyhassomelimitations,suchasthesmallnumber ofpatientsandlackofageneticassessment.Randomized, larger and controlled studies are needed to confirm the presentdata.However,itisararedisease,andthepresent studyhadoneofthelargestseriesintheliterature.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Lima CJ, Simões e Silva AC. Síndrome de Bartter: cinco casoscomdiferentesapresentac¸õesclínicas.JPediatr(RioJ). 2003;79:471---2.
2.SeyberthHW,SchlingmannKP.Bartter-andGitelman-like syn-dromes: salt-losing tubulopathies with loop or DCT defects. PediatrNephrol.2011;26:1789---802.
3.FinerG,ShalevH,BirkOS,GalronD,JeckN,Sinai-TreimanL, etal.Transientneonatalhyperkalemiaintheantenatal(ROMK defective)Barttersyndrome.JPediatr.2003;142:318---23. 4.VaisbichMH,FujimuraMD,KochVH.Barttersyndrome:
bene-fitsandsideeffectsoflong-termtreatment.PediatrNephrol. 2004;19:858---63.
6.Piepsz A, Tondeur M, Ham H. Revisiting normal (51) Cr-ethylenediaminetetraacetic acid clearance values in chil-dren.EurJNuclMedMolImaging.2006;33:1477---82.
7.Littlewood JM, Lee MR, Meadow SR. Treatment of Bartter’s syndrome in early childhood with prostaglandin synthetase inhibitors.ArchDisChild.1978;53:43---8.
8.ShalevH,OhaliM,KachkoL,LandauD.Theneonatalvariantof Barttersyndromeanddeafness:preservationofrenalfunction. Pediatrics.2003;112:628---33.
9.HeneRJ,KoomansH,DorhoutMeesEJ,StopleA,VerhoefGEG, Boer P. Correction of hypokalemia in Bartter’s syndrome by enalapril.AmJKidneyDis.1987;9:200---5.
10.AmirlakI, Dawson KP. Bartter syndrome: an overview. QJM. 2000;93:207---15.
11.HaasNA,NossalR,SchneiderCH, LewinMA,OckerV,Holder M,et al. Successfulmanagement ofanextreme example of neonatalhyperprostaglandin-Esyndrome(Bartter’ssyndrome) withthenewcyclooxygenase-2inhibitorrofecoxib.PediatrCrit CareMed.2003;4:249---51.
12.Silverstein FE, Faich G, Goldstein JL, Simon LS, Pincus T, Whelton A, etal. Gastrointestinaltoxicitywithcelecoxib vs
nonsteroidal anti-inflammatory drugs for osteoarthritis and
rheumatoid arthritis: the CLASS study: a randomized con-trolledtrial.CelecoxibLong-termArthritisSafetyStudy.JAMA. 2000;284:1247---55.
13.Frampton JE, KeatingGM. Celecoxib: a review of its usein themanagementofarthritisandacutepain.Drugs.2007;67: 2433---72.
14.White WB, West CR, Borer JS, GorelickPB, Lavange L, Pan SX,et al.Risk ofcardiovascular eventsinpatientsreceiving celecoxib:ameta-analysisofrandomizedclinicaltrials.AmJ Cardiol.2007;99:91---8.
15.YanQ,YangX,CantoneA,GiebischG,HebertS,WangT.Female ROMKnullmicemanifestmoresevereBartterIIphenotypeon renalfunctionandhigherPGE2production.AmJPhysiolRegul IntegrCompPhysiol.2008;295:R997---1004.
16.MoralesJM,RuilopeLM,Praga M,CotoA,Alcazar JM,Prieto C,NietoJ,etal.Long-termenalapriltherapyinBartter’s syn-drome.Nephron.1988;48:327.