www.jped.com.br
EDITORIAL
Rheumatic
and
other
musculoskeletal
manifestations
and
autoantibodies
in
childhood
and
adolescent
leprosy:
significance
and
relevance
夽
,
夽夽
Manifestac
¸ões
reumáticas
e
outras
manifestac
¸ões
musculoesqueléticas
e
autoanticorpos
em
crianc
¸as
e
adolescentes
com
hanseníase:
significado
e
relevância
Arvind
Chopra
CenterforRheumaticDiseases,Pune,India
Leprosy is an important communicable disease. Despite
aggressive control and eradication programs and rapidly
developing economies, countries such asIndia and Brazil
continuetobelargereservoirsforspreadofdisease.
Leprosy amongst children accounts for approximately
10%ofallcasesinendemicregions.In2010,thecoefficient
of detection of leprosy in Brazil was18.3/100,000 in the
generalpopulationand1.3/100,000inchildren(<15years
ofage).1Theproportionofchildren(<15yearsofage)was
12.9%amongstallleprosycasesinarecentprospectivestudy fromIndia.253%ofthechildrensufferingfromleprosywere
10yearsoldor lessinastudy fromColombia.3Leprosyin
infants,thoughrareandoftenmissed,hasbeenreported.4
Tounderstandmusculoskeletal(MSK)involvement,itis pru-denttoreviewleprosyinpediatricandadolescentsubjects
DOIoforiginalarticle:
http://dx.doi.org/10.1016/j.jped.2014.01.007
夽 Pleasecitethisarticleas:ChopraA.Rheumaticandother
mus-culoskeletal manifestations and autoantibodies in childhood and adolescentleprosy:significanceandrelevance.JPediatr(RioJ). 2014;90:431---6.
夽夽
SeepaperbyNederetal.inpages457---63. E-mail:[email protected]
(Table1).2,5---8Prevalencestatisticsareconfoundedbysmall
samplesizes,studysite,andmethodology.
Severalaspects of childhoodandadolescent onset dis-ease need tobe recognized and may be unique. Leprosy in children is a critical reflection of the extent of trans-mission(microbe)inthecommunity.Childrenarebelieved tobe the most vulnerable group toMycobacterium lepra
infection.Theincubationperiodofleprosyisgenerallylong (rangeoftwotosevenyears)andchildrenneedanintense prongedcontactwithacontagiouscase(usuallyinafamily) tocontractthedisease.Severaladolescentandyoungadult casesarelikelytohavecontractedtheillnessasachild.The entirespectrumofleprosycanalsobeobservedinchildren, thoughproportionsoftypesmayvary.Tuberculoid, border-line,andindeterminateformspredominate.SignificantMSK articularinvolvement is predominantly found in leproma-tous forms and lepra reactions, which are somewhat less observed amongpediatric cases.9,10 Single hypo-aesthetic
skinlesions,paucibacillary formsandlowskinsmear posi-tivity(acidfastbacillus)appeartobehallmarkofchildhood cases.
MSKinvolvementis frequentandvariable(Table2).9---14
The extent is largely influenced by the geographical and endemicfactorsandstudysites;itvariesconsiderably.9,10,13
Itis second tocutaneous and neurologicalmanifestations
http://dx.doi.org/10.1016/j.jped.2014.06.003
432
Chopra
A
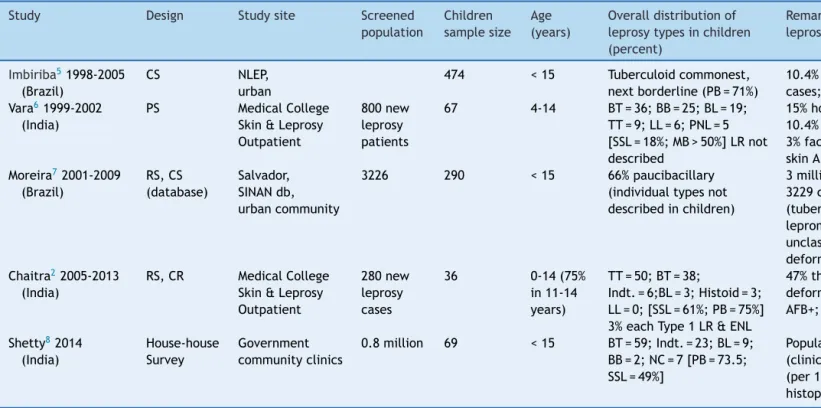
Table1 Selectedepidemiologicalstudiesofleprosywithspecialreferencetochildhoodonsetdisease.
Study Design Studysite Screened
population
Children samplesize
Age (years)
Overalldistributionof leprosytypesinchildren (percent)
Remarks/descriptorsforchildhoodonset leprosy
Imbiriba51998-2005 (Brazil)
CS NLEP,
urban
474 <15 Tuberculoidcommonest, nextborderline(PB=71%)
10.4%childhoodcasesofallleprosy cases;2.9%disability
Vara61999-2002 (India)
PS MedicalCollege
Skin&Leprosy Outpatient
800new leprosy patients
67 4-14 BT=36;BB=25;BL=19; TT=9;LL=6;PNL=5 [SSL=18%;MB>50%]LRnot described
15%householdcontact;70%thicknerve; 10.4%gradeIIdeformity;6%ulnarclaw; 3%facialpalsy;1.5%weakfoot;46%slit skinAFB+
Moreira72001-2009 (Brazil)
RS,CS (database)
Salvador, SINANdb, urbancommunity
3226 290 <15 66%paucibacillary
(individualtypesnot describedinchildren)
3millionurbanpopulationscreenedand 3229casesofleprosyidentified
(tuberculoid=32;Indt.=17; lepromatous=18;borderline=29; unclassifiable=4);18%childrenwith deformity
Chaitra22005-2013 (India)
RS,CR MedicalCollege Skin&Leprosy Outpatient
280new leprosy cases
36 0-14(75%
in11-14 years)
TT=50;BT=38;
Indt.=6;BL=3;Histoid=3; LL=0;[SSL=61%;PB=75%] 3%eachType1LR&ENL
47%thicknerves;fivecasesofminimal deformity(1footdrop);8%slitskin AFB+;75%conclusivehistopathology
Shetty82014 (India)
House-house Survey
Government communityclinics
0.8million 69 <15 BT=59;Indt.=23;BL=9; BB=2;NC=7[PB=73.5; SSL=49%]
Populationstudy;childrenprevalence (clinicalexam):urban=1.5;rural=10.5 (per10,000)clinical+smear+
histopathological.
Studiesareofgeneralnatureandmostlywithmixedchildrenadultpopulation(exceptforthestudybyImbiribaetal.),andarenottargetedtomusculoskeletal/articularinvolvement.
NLEP,Nationalleprosyeradicationprogram;PS,prospectivestudy;RS,retrospectivestudy;CS,crosssectionalanalysis;CR,caserecord;SINAN,NotifiableDiseasesInformationSystem
Database;db,database;TT,polartuberculoid;BT,borderlinetuberculoid;BB,borderline/dimorphous;BL,borderlinelepromatous;LL,polarlepromatous;PNL,pureneuriticleprosy;
and other musculoskeletal manifestations and autoantibodies in childhood 433
Table2 Selectedstudiesofleprosyinchildren&adolescentswithreferencetomusculoskeletal(MSK)articularinvolvement.
Study Design Studysite Sample
size
MSKPrev. (%)
Ageinyears Distributionof leprosytypesinMSK (%)
RF ANA MSKprofile
(percent)
Remarks
Vengadakrishnan11 2003(India)
PS,CS Hospital leprosy outpatient (teaching)
70 61.4 9cases<20 BB=39;Indt.=17; Tuberculoid=23; lepromatous=21
34.9% (21% MSK)
ND PA(RA-like)=44; OLA=10;STR=17; arthralgias=8;En=3
82%thicknerves;Indt commonestin<20years age(nonelepromatous); 47%LR(noneENL)with arthritisin55% Ribeiro13 2004-2006 (Brazil) PS,CS, Follow Commleprosy Clinic
158 48% mean
39.88±15.77
LL=38;BT=21; BL=20;BB=16; TT=3;Indt.=3
3% - Arthralgias=20; PA=80
82controlleprosypatients withoutMSK;69controlRA patients;89healthy controls Pereira9 2004 (Brazil) PS,CS, follow Commleprosy Clinic
1,257 (i)9.1c (ii)6.3c
mean40±16 LL=34;BL=23; BT=20;BB=17; Indt.=3.8;TT=2.5
4.5% - PA=57;OLA=36; MA=7
70%men;nonewith arthritishadtuberculoidor Indtforms;91%presented LR(largelyENL)
Salvi10 1998-2012 (India) RS,CS, follow ReferralComm ArthritisClinic
33a NA median49
(19-72)
Lepromatous=67; Tuberculoid=27; polyneuritic=6
27%d 38%d RA=21;NSA=12; vasculitis=3; IA-U=64
67%clinicalneuropathy; 38%casespresentedfirst time(IA&usuallyENL];five casesclawhand;case rate=0.08/100rheum. cases
Prasad12 2001-2010 (India)
RS,CS HospitalRheum outpatient (teaching)
44b NA mean40
(16-71)
ENL=64%;PNL=18; LL=9;Charcot=2; Lucio=2;Others=5
4.5% 2% PA=32;SpAlike=16; SHFS=25;
Charcot=2;TS=20; SF=20;
Arthralgias=16
70%thicknerves;PAwasRA like5%clawhand;50% leprosypresentedwith acuteIA Neder14 2010-2012 (Brazil) PS,CS, follow HospitalSkin outpatient (university)
50 7 median12
(3-18)
94%skinlesions; MB=48;PB=52(86% MSKwasMB;58% non-MSKwasPB)
4% 2% MSK=14(arthritis=8; arthralgias=2; myalgia=6)
47healthycontrol;type1 LR=10%(nilENL);22% neuritis
Prev.,prevalence;Comm.,community;RF,rheumatoidfactor;ANA,antinuclearantibody;PS,prospectivestudy;CS,crosssectionalanalysis;RS,retrospectivestudy;TT,polartuberculoid;
BT,borderlinetuberculoid;BB,borderline/dimorphous; BL,borderlinelepromatous;LL,polarlepromatous;PNL:pureneuriticleprosy;Indt.,indeterminate;MB,multibacillary;PB,
paucibacillary;LR,leprareaction;ENL,erythemanodosumleprosum;IA,inflammatoryarthritis;U,undifferentiated;SpA,spondyloarthritislike,dominantlowerlimb;TS,tenosynovitis;
SHFS,swollenhandsandfeetsyndrome;OLA,oligoarticular;SF,swollenfeet;En,enthesitis;STR,softtissuerheumatism;Rheum.,rheumatology;RA,rheumatoidarthritis;PA,polyarthritis;
NA,notavailable;MA,monoarthritis;ND,notdone;NSA,non-specifiedarthralgias.
a 41,000electronicrheumatologycaserecordsscreenedtoidentifyleprosycases.
b numberofpatientrecordsscreenednotknown.
c 115patients(9.1%)ofleprosywitharthritis&79(6.3%)patientsofleprosyrelatedarthritisafterexcludingco-existentrheumaticdisorderslikerheumatoidarthritis.
434 ChopraA
bothinnon-reactionaryandreactionarystates.Mostofthe
MSKstudies inleprosyarefromBrazilandIndia(Table2).
Overall, MSK data is sparse and woefully dismal in chil-dren (Table 2). The antiquity of childhood leprosy was recently established by the discovery of two childhood leprosy cases with bony involvement in ancient skeletal remains.15
In-depth comparisons of case seriesin Table 2 arenot appropriatebecauseofdifferentmethodsusedandseveral other confoundingissues. The overall pattern of MSK dis-orders may not differ much in children and adolescents. Severalstudies9,10,12haveconfirmedthenon-erosivenature
ofleprosyassociatedinflammatoryarthritis.
Leprosyispredominantlymanagedbydermatologists.It islikelythatonlya proportionof patientswithsignificant MSKaffectionisattendedtobyarheumatologist(Table2). Childhood leprosy withsignificant arthritis appears tobe infrequent.Theauthorvisitedthesourcedatabaseofacase seriesreport (Table2).10 One case report found wasthat
ofa 19-year-old male(past history ofskin psoriasis at 10 yearsofage)whowasevaluatedforanacutefebrileonset ofrheumatoidarthritis(RA)-likepolyarthritis(seronegative forrheumatoidfactor[RF]),atypicalskinlesions,andafew suspiciousnodules,andfinallydiagnosederythemanodosum leprosum (ENL); around1,700 rheumatic referral patients (childrenand adolescents)hadbeen evaluatedduringthe studyperiod(1998-2013).Asignificantproportionofleprosy associatedinflammatoryarthritisexaminedby rheumatolo-gistsinleprosyclinic basedstudy9 wasreportedtoclosely
resembleRAorspondyloarthritis(SSA).
Itis againstthisperspectivethattherecent study14 by
Neder etal. holds merit. Despite a relatively small sam-plesize,itwasawell-designedstudy.Bothdermatologists andpediatricrheumatologistswereinvolved.Thestudy pro-videdsomeimportantinsights.Unlikeothers(Table2),that studywastrulyfocusedonMSKandarthritisinchildrenand adolescentssufferingfromleprosy.Theprevalenceof MSK articular disorder (median duration 12 months) was 14%. Fivepatients,predominantly borderlineleprosy,showeda chronic asymmetric polyarthritis (hands). Despite severe articularpain,noneofthechildrenwerediagnosedwithMSK painsyndromes(likefibromyalgia).Asignificantfunctional impairment was observed. Lepra reactions (only Type 1) andsignificant neuropathy(oftensilent)weresignificantly (p<0.05)observedintheMSKgroup. Although paucibacil-lary forms were predominant, MSK patients were mostly diagnosedwithmultibacillaryleprosy.TheprevalenceofRF and antinuclear antibodies (ANA) was low (Table 2), and exceptforimmunoglobulin-M(IgM)anti-cardiolipinantibody (cases=8,controls=6),severalotherautoantibodies(AAb) wereabsentorinsignificant(<2%).
In a broad sense, based on personal experience and literature review, MSK articular involvement in leprosy maybeclassifiedintothefollowing categories:(i) inflam-matory arthritis, usually acute and commonly observed duringleprareactions,itcanmimicRA(juvenileidiopathic arthritisin thecase of children) or SSA;(ii)inflammatory swollenhandsandor feet(similar to‘remitting seronega-tivesymmetricalsynovitiswithpittingedema’ syndrome); (iii) neuropathic arthritis or Charcot’s joints, generally observedas chronic arthritis;(iv) septic arthritis;(v) non specificarthralgiasandmyalgias;(vi)softtissuerheumatism
affectionincludingtenosynovitisandenthesitis;(vii) inflam-matorymultisysteminvolvementsimilartocollagenvascular disease---includingvasculitis,myositis,purpurafulminans, Lucio’s phenomenon, cryoglobulinemia, digital vasculi-tis/gangrene;and(viii)co-existingchronicformsofarthritis which include RA, SSA, osteoarthritis, and other rheuma-tological disorders, which are often difficult to totally differentiatefromleprosyassociatedarthritis.
Patientsmayhaveanoverlapofcategoriesorexpress dif-ferentMSKdisordersover time.Severalstudies10,12,16from
rheumatologyclinicshaveunequivocallydemonstratedthat a significant proportion of leprosy patients may present forthefirsttimewithacutesevereinflammatoryarthritis, often a component of lepra reaction, and are mistak-enly treated for prolonged periods with anti-rheumatic drugs(with potentiallydisastrousconsequences).Articular involvementisgenerallyignoredinchildrenandadolescents withleprosy,anddifferentialdiagnosisofchronic polyarthri-tis includes juvenile idiopathic arthritis, acute leukemia, andchildhood-systemic lupuserythematosus.14 To
summa-rize,leprosyisthegreatmimicoftheMSK-articularsystem and can present with protean manifestations requiring a highindexofclinicalsuspiciontomakeacorrectandtimely diagnosis.10,12
Itiswellknownthatleprosypatientscanbefloodedwith antibodies.Fromarheumatologicalperspective,itis impor-tanttorecognizefalsepositiveAAb;theseincludeRF,ANA, antibodytoanti-citrullinatedcyclicpeptides(a-CCP), anti-bodytoanti-neutrophiliccytoplasmicantigens(ANCA),and antiphospholipidantibodies(APL)/anti-cardiolipin antibod-ies (ACL).The frequency of seropositive RF (Table 2) has variedconsiderably,whichisduetoassaymethods,patient selection,andotherreasons.Inacontrolledleprosystudy,17
35% and 55.8% of patients tested seropositive for RF and ANA,respectively;15.8%patientswereseropositiveforboth AAb.TherewasnocorrelationbetweenRF/ANAand arthri-tis(68%prevalence)inthelatterstudy.17 Thefrequencyof
seropositiveRFwasreported11 tovaryconsiderablyin
dif-ferentleprosytypes(lepromatous>borderline>tuberculoid >Indeterminate).
Ribeiroet al.13 (Table 2) demonstrated a lower
preva-lenceof a-CCP(2.6%) andIgMRF (1.3%).A Mexican adult leprosy study18 reportedsignificanta-CCPin5.9% patients
and RFin 16.8%patients; polarlepromatous (LL) patients hadhighera-CCPandRFlevelsthanpolartuberculoid(TT) patients. Thelow seropositivityof a-CCPcanusefully dif-ferentiatebetweenRAandleprosyassociatedinflammatory arthritis.
ANCA,amarkerofvasculitis, wasreportedinleprosy19
andp-ANCA(31%lepromatous,16%borderline,nil tubercu-loid)hadahigherfrequency thanc-ANCA(5%lepromatous only). An Indian study20 (children included in borderline
tuberculoid [BT]group) demonstratedawidespectrum of AAb, including ANA, double-stranded DNA (dsDNA), and ANCA in different leprosy types. The high prevalence of ANCA antibodies (62.5% c-ANCA) in the latter study was intriguing.
A large-sample genome-wide association study from China demonstrated an unequivocal association of NOD2 locus, HLA-DRB1, LRRK2, TNFSF15 (tumor necrosis factor (TNF)---likemolecule),andPARK2withleprosy.22The
patho-genesisofarticularinvolvementinleprosyisstillnotfully clear.Itisevidentthatanintenseimmune-mediated inflam-mation driven by the unique genetic configuration and cytokine milieu in a susceptible host is at the core of inflammatory rheumatic syndromes andlepra reactions in leprosy.Severalpro-inflammatorycytokinesplay acritical role(Th1 cytokinesintype-I reactions, andTh2 cytokines andtumornecrosisfactor-alfainENL).Directinfiltrationof the synovium andperipheral sensoryneuropathy leads to destructivearthritis(Charcot’sorneuropathicjoints).Some molecularmechanismsof immuneinflammation appearto becommontoinfectionsandautoimmunedisorders.Serum concentrationofpro-inflammatorymyeloid-relatedproteins (MRPs) 8 and 14 were recently reported to be elevated in patients with juvenile idiopathic arthritis (> 40-foldin systemic onset type)and infections (almost seven-foldin leprosytype-IIreactions)ascomparedtohealthycontrols.23
Earlydiagnosisiscritical.Skinhistopathologyis diagnos-tic,but somehowneglectedin clinicalpractice.Recently, a new serological test for detection of antibodies to the M. leprae-specific phosphoglycolipid-1 was validated, but has not yet been used in routine practice.24 Other new
toolsvalidatedinpediatricleprosypatientsinclude detect-ing specific nucleic acid sequences by gene probes and amplificationtechniques(polymerasechainreaction[PCR]), immunocytochemistry,andin situhybridization(usingskin tissue).25
A recent retrospective study26 of 99 patient records
(several children and adolescents included) of leprosy with ENL concluded that in at least two patients, ENL was the direct cause of death. Although not described in detail, almost 70% of the cases appeared to have suffered from significant extra-cutaneous features that includedfever,neuritis,arthralgias,arthritis,tenosynovitis, osteitis, dactylitis, orchitis, lymphadenopathy, epistaxis, andproteinurea(>70%hadneuritis;eachotherfeaturewas recordedin<15%cases).
Althoughleprosyisendemicinsomepartsoftheworld, it continues to be a global problem. An important con-tributory factor is the large number of migrants seeking shelter in developed countries. The diagnosis may be a greaterchallengeinnon-endemiccountriesbecauseoflow awareness.Wheneverythingisconsidered,childhoodonset leprosyshouldringalarmbellsthatallisnotwellwiththe preventionanderadicationprograms.
Conflicts
of
interest
Theauthordeclaresnoconflictsofinterest.
References
1.LanaFC,FabriAdaC,LopesFN,CarvalhoAP,LanzaFM. Defor-mitiesduetoleprosyinchildrenunderfifteenyearsoldasan indicatorofqualityoftheleprosycontrolprogrammein Brazil-ianmunicipalities.JTropMed.2013;2013:812793.
2.ChaitraP,BhatRM.Posteliminationstatusofchildhoodleprosy: reportfromatertiary-carehospitalinSouthIndia.BiomedRes Int.2013;2013:328673.
3.Cardona-CastroN.LeprosyinColombia:posteliminationstage? LeprRev.2013;84:238---47.
4.MoorthyKV,DesikanKV.Indeterminateleprosyinaninfant.Lepr Rev.2006;77:377---80.
5.ImbiribaEB,Hurtado-GuerreroJC,GarneloL,LevinoA,Cunha M,daG,PedrosaV.Epidemiologicalprofileofleprosyinchildren under15 inManaus(Northern Brazil), 1998-2005.RevSaude Publica.2008;42:1021---6.
6.VaraN.Profileofnewcasesofchildhoodleprosyinahospital setting.IndianJLepr.2006;78:231---6.
7.Moreira SC, Batos CJ, Tawil L. Epidemiological situation of leprosy in Salvador from 2001 to 2009. An Bras Dermatol. 2014;89:107---17.
8.ShettyVP,GhateSD,WakadeAV,ThakarUH,ThakurDV,D’souza E.Clinical,bacteriological,andhistopathological characteris-ticsofnewlydetectedchildrenwithleprosy:apopulationbased studyinadefinedruralandurbanareaofMaharashtra,Western India.IndianJDermatolVenereolLeprol.2013;79:512---7.
9.PereiraHL,RibeiroSL,PenniniSN,SatoEI.Leprosy-relatedjoint involvement.ClinRheumatol.2009;28:79---84.
10.SalviS,ChopraA.Leprosyinarheumatologysetting:a chal-lengingmimictoexpose.ClinRheumatol.2013;32:1557---63.
11.VengadakrishnanK,SaraswatPK,MathurPC.Astudyof rheuma-tologicalmanifestationsofleprosy.IndianJDermatolVenereol Leprol.2004;70:76---8.
12.PrasadS,MisraR,AggarwalA,LawrenceA,HaroonN,WakhluA, etal.Leprosyrevealedinarheumatologyclinic:acaseseries. IntJRheumDis.2013;16:129---33.
13.RibeiroSL,PereiraHL,SilvaNP,NevesRM,SatoEI.Anti-cyclic citrullinatedpeptideantibodiesandrheumatoidfactorin lep-rosypatientswitharticularinvolvement.BrazJMedBiolRes. 2008;41:1005---10.
14.NederL,RondonDA,CurySS,SilvaCA.Musculoskeletal mani-festationsandautoantibodiesinchildrenandadolescentswith leprosy.JPediatr(RioJ).2014;90:457---63.
15.RubiniM,ErdalYS,SpigelmanM,ZaioP,DonoghueHD. Pale-opathological and molecular study on two cases of ancient childhoodleprosyfromtheRomanandByzantineEmpires.IntJ Osteoarchaeol.2012.DOI:10.1002/oa.2242.
16.SalviS,ChopraA.Lestwe forgetHansen’sdisease(leprosy): anunusualpresentationwithanacuteonsetofinflammatory polyarthritisandtherheumatologyexperience.IntJRheumDis. 2009;12:64---9.
17.DacasP, Picanso M,Mouchaileh G, Percegona L, SchultzMT, Silva MG, et al. Autoantibodies and rheumatic manifesta-tions in patients with Hansen’s disease. An Bras Dermatol. 2000;75:553---61.
18.Zavala-CernaMG,Fafutis-MorrisM,Guillen-VargasC, Salazar-Páramo M, García-Cruz DE, Riebeling C, et al. Anti-cyclic citrullinated peptide antibodies and rheumatoid factor sera titers in leprosy patients from Mexico. Rheumatol Int. 2012;32:3531---6.
19.MedinaF,CamargoA,MorenoJ,Zonana-NacachA,Aceves-Avila J,FragaA.Anti-neutrophilcytoplasmicautoantibodiesin lep-rosy.BrJRheumatol.1998;37:270---3.
20.PradhanV,BadakereSS,ShankarKumarU.Increasedincidence ofcytoplasmicANCA(cANCA)andotherautoantibodiesin lep-rosypatientsfromwesternIndia.LeprRev.2004;75:50---6.
21.ForastieroRR,MartinuzzoME,deLarra˜nagaGF.Circulating lev-elsoftissuefactorandproinflammatorycytokinesinpatients with primary antiphospholipid syndrome or leprosy related antiphospholipidantibodies.Lupus.2005;14:129---36.
436 ChopraA
23.Frosch M, Ahlmann M, Vogl T, Wittkowski H, Wulffraat N, Foell D, et al. The myeloid-related proteins 8 and 14 complex,anovelligandoftoll-likereceptor4,and interleukin-1beta formapositivefeedbackmechanisminsystemic-onset juvenile idiopathic arthritis. Arthritis Rheum. 2009;60:883---91.
24.Britton WJ, Lockwood DN. Leprosy. Lancet. 2004;363:1209---19.
25.KamalR, NatrajanM,KatochK,Parvez M,NagVK, DayalR. Evaluationofthediagnosticvalueofimmunocytochemistryand
in situ hybridization in the pediatric leprosy. IndianJ Lepr. 2013;85:109---14.