w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Pre-sarcopenia
and
bone
mineral
density
in
adults
submitted
to
hematopoietic
stem
cell
transplantation
Cristiane
Pavan
Pereira,
Denise
Johnsson
Campos
Amaral,
Vaneuza
Araujo
Moreira
Funke,
Victória
Zeghbi
Cochenski
Borba
∗UniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14March2017 Accepted6June2017 Availableonline27July2017
Keywords:
Pre-sarcopenia BMD
GVHD
Hematopoieticstemcell transplantation
a
b
s
t
r
a
c
t
Background:Theaimofthisstudywastoevaluatetheprevalenceofpre-sarcopeniaandbone
mineraldensityafterhematopoieticstemcelltransplantation.
Methods:Thestudygroupconsistedofover18-year-oldpatientswhohadbeensubmittedto
allogeneictransplantationatleastoneyearpreviously.Patientsandhealthycontrolswere matchedbysex,ethnicbackground,age,andbodymassindex.Bodycompositionandbone mineraldensityweremeasuredbydual-energyX-rayabsorptiometry.A24-hfoodrecall andfoodfrequencysurveywereperformed.Thebiochemicalevaluationincludedcalcium, parathormoneandvitaminD.Eighty-sevenpatients(52men;age:37.2±12.7years;body massindex:25±4.5kg/m2)werecomparedto68controls[31men;age35.4±15.5years (p=0.467);bodymassindex25.05±3.7kg/m2(p=0.927)].
Results:There wasnosignificant differencein thedietaryintakebetweenpatientsand
controls.ThemeanlevelsofvitaminDwere23.5±10.3ng/mL;29patients(41.0%)had insuf-ficientand26(37.14%)deficientlevels.Ahigherprevalenceofreducedbonemineraldensity wasobservedin24patients(25%)comparedto12controls(19.1%–p<0.001).Pre-sarcopenia wasdiagnosedin14(14.4%)patientsandnoneofthecontrols(p=0.05).Therewasahigher prevalenceofpre-sarcopenia(66%)inpatientswithgradesIIIandIVcomparedtothosewith grades0-IIgraft-versus-hostdisease(10.9%)(p=0.004).
Conclusion: patientssubmittedtotransplantationhadahigherprevalenceofpre-sarcopenia
andgreaterchangesinbonemineraldensitycomparedtocontrols;theseverityof graft-versus-hostdiseasehadanimpactontheprevalenceofpre-sarcopenia.
©2017Associac¸ ˜aoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthorat:AvAgostinhoLeãoJunior,285–AltodaGlória,80030-110Curitiba,PR,Brazil.Tel.:+55412141173.
E-mailaddress:[email protected](V.Z.Borba). http://dx.doi.org/10.1016/j.bjhh.2017.06.005
Introduction
Hematopoietic stemcell transplantation (HSCT) isa thera-peuticmodalityusedtotreatmalignantorbenigndiseases. Scientific advances have allowedan increasing number of transplantsand longer disease-free survival.Consequently, thereisanincrementinpost-transplantcomorbidities sec-ondarytothedisease,conditioningregimenorcomplications, suchasgraft-versus-hostdisease(GVHD). Changes inbone mineraldensity(BMD)mayoccurduetotheuseof glucocor-ticoids,reduced physicalactivity,lowexposuretosunlight, reductioninleanbodymass,andvitaminDdeficiency.These changes are observed as early as the first months after HSCToraslateastenyearsaftertheprocedure.1–4Recently,
sarcopeniahasbeen describedafterseveral typesof trans-plantssuchasliver,kidneyandlung,andmayinfluencethe outcome.5–8
Thetermsarcopeniacharacterizeslossoffunctionrelated to loss of skeletal muscle mass. It is denominated pre-sarcopeniawhenonlylossofmusclemassisdetected.The etiologyismultifactorial,butusuallyoccursdueto neurode-generative,endocrineorchronicdiseases,malnutritionorlack ofexercise,whichleadstomuscleatrophy.9AfterHSCT,the
associationofpre-sarcopeniaand sarcopeniawiththe pre-existingdiseasemayworsenthepatient’sbaselinecondition, increasingtherisk offractures,especially whenassociated withreductionsinBMD.Theearlydiagnosisofsarcopeniamay allowpreventiveand/orcurativetreatmentofthesepatients. Thisresearchevaluatedtheprevalenceofpre-sarcopeniaand changesinBMDinagroupofHSCTpatients.
Methods
Thisobservational,transversalstudyenrolledover18-year-old patients,regardlessofethnicbackgroundorsex,who under-wentallogeneicHSCTattheBoneMarrowTransplantUnitof theHospitaldeClinicas da UniversidadeFederaldoParaná (STMO-HC-UFPR).Thesamplewasselectedbyconvenience; patientswereinvitedtoparticipateduringtheirroutinevisit. Toavoidtheconsequencesofacutebonemarrow transplanta-tioncomplications,patientswhohadbeentransplantedless than one year previously were excluded, as were patients withadiagnosisofFanconianemia.Acontrolgroup(CG)was formedofhealthysubjectsmatchedwiththestudygroup(SG) bysex,age,ethnicbackground,andbodymassindex(BMI). Patientsand controls performeddual-energy X-ray absorp-tiometry(DXA)inawhole-bodyscanner(LunarProdigy;GE MedicalSystems,Madison,WI,USA)usedinconjunctionwith enCORE2002 software (GE Medical Systems) to assess the bodycomposition.Thesoftwareprovidesdataaboutleanbody mass(bone massplus fat-free mass), bone-free lean mass (leanmassminusfat-freemass),fatmass,andbonemineral density(BMD).Bloodsampleswerecollectedforbiochemical analysis,andareviewofhospitalrecordswascarriedoutto searchfordataregardingtheHSCT.
TheBMDoftotalbody,lumbarspine(LS),andfemur(neck andtotal)wereevaluatedwiththeresultsbeingcategorized asnormalorabnormalfollowingtheInternationalSocietyFor
ClinicalDensitometry(ISCD).10Thepercentageofleanmass
(%LM)andappendicularleanmass(ALM)werecalculated.
Diagnosisofpre-sarcopenia
Thediagnosisofpre-sarcopeniawasperformedconsidering threecriteriaavailableintheliterature.Patientswere cate-gorizedaccordingtoBMIasnormal(BMI<25kg/m2)orobese
(BMI>25kg/m2).AfterevaluatingtheALMandforthosewith
anormalBMI,thecriterionofBaumgartneretal.11wasused,
which defines the reductionofappendicular skeletal mus-clemassastwostandarddeviations(SDs)belowthemeanof younghealthycontrols,matchedwiththesameethnicgroup oftheNewMexicopopulation.Values<5.45forwomenand <7.26formenwereconsideredpositive.Forindividualswith BMI ≥25kg/m2, the diagnosis ofpre-sarcopenia was
calcu-latedbasedonthecriterionofDelmonicoetal.12Initially,a
linearregressionmodelwasadjustedforALM(kg)including height(m) andtotalfatmass(kg)asexplanatoryvariables. The residualsofthe regression were used toidentify indi-vidualswithaleanmasslowerthanthevaluepredictedfor a given fat mass (given by an equation derived from the model). A positive residual indicates a relatively muscular individual,whereasanegativeresidualindicatesanindividual withsarcopenia.Theequationsderivedfromthemodelwere the following: formales –ALM(kg)=−30.54+30.88×height (m)+0.0823×total fat mass (kg); and for females – ALM (kg)=−12.45+15.79×height(m)+0.1081×totalfatmass(kg). The20thpercentileofthedistributionofresidualswasused asthecut-offpointforthediagnosisofsarcopeniaaccording totheALMadjustedforfatmassaspreviouslydefined.Inthis patientsample,thecut-offpointcorrespondedtoresidualsof −2.021formenand−1.082forwomen.
Finally, theALM/BMIcriterionofTheFoundationforthe NationalInstituteofHealth(FNIH)wasused,andthevalues of<0.789formenand<0.512forwomenwereconsidered pre-sarcopenia.13
Food intakewas assessedinaninterview conductedby aregistereddieticianwitha24-hrecallquestionnairebased on type and quantities of food consumed the day before theinterview,atoolappropriatetoassesstheconsumption of a nutrient with a specific dietary recommendation.14,15
Calcium, vitamin D, protein, and total calorie intake were calculated by AVANUTRI®, a nutritional assessment pro-gram,followingthereferenceofthe “recommendeddietary allowance” (RDA)accordingtosexandage.Theintakewas consideredadequatewhenitreachedorexceededtheRDA. TheRDAofcalciumforages19–50yearsis1000mgandfor >50years,itis1200mg;15gofvitaminDisrecommended forindividualsbetween19and70years.16
Biochemicalanalysis
insufficiency between 21 and 29ng/mL and normal over 30ng/mL.17
Statisticalanalysis
Data are presentedasmeans±SD exceptwhereotherwise specified.All statisticalanalyses wereperformed usingthe StatisticalPackagefortheSocialSciences(SPSS)version20.0 (IBMCorporation,Armonk,NY,USA).Forthevariables eval-uated,thenormalityofthedatadistributionwasevaluated usingtheKolmogorov–Smirnovtest.Student’st-testfor inde-pendentsamplesor thenonparametricMann–Whitneytest wasusedtocomparequantitativevariablesbetweenthetwo groups.Fisher’sexacttestandthechi-squaretestwereused toassesstheassociationbetweentwoqualitativevariablesin thepreliminarystatisticalanalysis.p<0.05wereconsidered statisticallysignificant.Correlations were sought using the PearsonandSpearmancoefficientsforvariableswithnormal andnon-parametricdistributions,respectively.Forall analy-ses,atwo-sidedp<0.05wasconsideredtoindicatestatistical significance.Morethantwogroupswerecomparedusingthe modelofanalysisofvariance(ANOVA)andtheleastsignificant difference(LSD)testformultiplecomparisons.
Results
Thesamplewasinitiallycomposedofthe first100patients (SG) who agreed to participateand who met the selection criteria. Asthreepatients didnotperform bone densitom-etry, theywere excluded and the final samplesizewas 97 patients (n=52–53.6% male). Themean age was 37.4±12.7 years,withanaverageweightof70.1±14kg,meanheightof 1.67±0.09mandmean BMIof25±4.5kg/m2.Basedonthe
BMI,14(14.4%)patientswereclassifiedasobese,29 (29.9%) overweight,four(4.1%)underweightand50 (51.6%)normal. Twenty-threepatientssufferedGVHD;fivepatientshadgrade I,12 gradeII, threegradeIII andthree gradeIV.A median cumulativedoseofglucocorticoidsof7181mg(55–37,275mg, equivalentofprednisone)wasusedby46outof89patients, andonlyeightpatientsweretakingglucocorticoidsatthetime ofthisevaluation.
TheCGconsistedof68apparentlyhealthyindividualswith ameanageof35.9±15.2years(n=31–45.5%males).Themean BMIwas25.05±3.7kg/m2with39(57.3%)controlsbeing
clas-sifiedasnormal,23(33.8%)asoverweight,andsix(8.9%)as obese,adistributionsimilartothatofthe patients.Table1 showstheclinicalcharacteristicsofpatientsandcontrolsand diagnosisoftheunderlyingdisease.
The mean consumption of protein was 78.7±38g/day (1.2±0.6g/kg),which was appropriatein80.4% ofpatients. Theaveragedailycalorieintakewas1892±852kcal,a suit-abletotalenergyexpenditure(TEE)in36%andgreaterthan thenecessityin26%ofthepatients.Themeandailyintakeof calciumwas456±347mgandthemedianintakeofvitamin Dwas1.91±6.95gconsideredinsufficientaccordingtothe RDAin96.4%and83.5%ofpatients,respectively(Figure1).
Nosignificantdifferencewasfoundinthefood consump-tionbetweenpatientsandcontrols.Inaddition,nodifference was observed in the food consumption between patients
Table1–Clinicalcharacteristicsofpatientsandcontrols.
Variable Patients (n=97)
Controls (n=68)
p-value
Mean±SD
Age(years)-mean±SD 37.4±12.7 35.9±15.19 0.467
Sex(M/F) 52/45 31/37 0.423
Weight(kg)-mean±SD 70.05±14.04 70.5±11.67 0.918
BMI(kg/m2)-mean±SD 25.03±4.47 25.05±3.7 0.927
TypeofHSCT
Allogeneic–related 62(63.9%) Allogeneic–
non-related
35(36.1%)
Diagnosis
Leukemia 50(51.5%) SAA 32(33.0%) Othersa 15(15.4%)
TimesinceHSCT(years)
1–5 49(50.5%)
6–10 15(15.5%) >10 33(34.0%)
Typeofconditioning
Myeloablative 64(66%) Reducedintensity 33(34%)
Typeofimmunoprophylaxis
CSA+MTX 75(77.3%) WithGC 17(17.5%) Othersa 5(5.2%)
SD:standarddeviation;M:male;F:female;BMI:bodymassindex; HSCT:hematologicalstemcelltransplantation;SAA:severeaplastic anemia;CSA:cyclosporine;MTX:methotrexate.
a Others: myelofibrosis, myelodysplasia, adrenoleukodystrophy,
marrowaplasia.
with abnormal or normal BMD. The mean calorie intake was 1742±513kcal/day and 1951±938kcal/day in patients withabnormalandnormalBMD,respectively(p=0.989). Pro-teinintakewas73.7±38.1and80.7±38.2g/dayinthosewith abnormalBMDandnormalBMD,respectively(p=0.441). Cal-ciumintakewas387±323and473±353mg/dayinpatients withabnormalandnormalBMD,respectively(p=0.294)and
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
Energy
% of patients with adequate intake
Proteins Vitamin D Calcium
45
40
35
30
25
20
15
10
5
0
Sufficient Insufficient Deficient
% of Patients
Figure2–Distributionofpatientsaccordingtothe classificationofvitaminDlevels.
theintakeofvitaminDwas1.89±4.13and1.88±7.73g/day in patients with abnormal and normal BMD, respectively (p=0.991).
ThemeanserumlevelofvitaminDwas23.5±10.3ng/mL. Thelevelsweresufficientin16(22.8%)patients,withan aver-ageof37.59±8.19ng/mL;insufficientin29(41%),withamean of23.98±2.60ng/mL; and deficient in26 (37.14%), with an averageof13.65±4.85ng/mL(Figure2).ThemeanlevelofPTH was85.7ng/mL(range:29.9–179.0)andthemeanserum cal-ciumwas9.4±0.5mg/dL.
Consideringthe criteria of Baungartner and Delmonico, pre-sarcopeniawasdiagnosedin33(34%)patientsandinonly three(4.6%)controls(p<0.001)withnosignificantdifferencein respecttosex–18(40%)womenand15(28.8%)men(p=0.287). Atendencywasobservedforfewerdiagnosesovertimeafter HSCT:pre-sarcopeniawaspresentin44.9%,26.7%and21.2% ofcases1–5years,6–10yearsandmorethan10yearsafter HSCT,respectively(p=0.069).Usingthesediagnosticcriteria, theprevalenceofpre-sarcopeniawashigheramongpatients whounderwentunrelated(46.9%)comparedtorelated(24.6%) allogeneicHSCT(p=0.037).Theprevalenceofpre-sarcopenia didnotchangewiththetypeofconditioning, immunoprophy-laxis,diagnosis,serumcalcium,vitaminDandPTHlevels,or inrelationtodietaryintakeofcalcium,vitaminD,caloriesor protein.
Regardingassessmentsusingthediagnosticcriterionofthe FNIH,therewerefewdiagnosesofpre-sarcopenia:14(14.4%)of theSGandnoneoftheCG(95%confidenceinterval:7.4–21.4%;
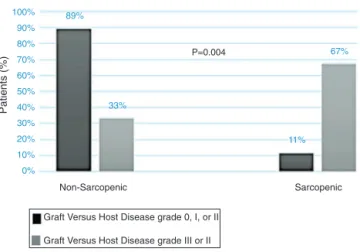
p=0.05).Inaddition,nodifferencewasobservedbetweensex [9(11.2%)womenand6(7.3%)men;p=0.428]andtimeafter HSCT,typeofHSCT,typeofconditioning,immunoprophylaxis, diagnosis,orothervariables.Theprevalenceofpre-sarcopenia wasdifferentaccordingtotheseverityoftheGVHD:foundin 67%ofpatientswithGVHDgradeIIIandIVandinonly11%of thosewithgradeIandII(p=0.004)(Figure3).
AbnormalBMDwasobservedin24(25%)ofpatientsinthe SGandin12patients(19.1%)intheCG(p=0.441).Comparedto men,morewomeninbothgroupshadabnormalBMD[18–40% women and 6–11.76% men in SG (p=0.002) and 11–31.4% women and 1–3.6% man in the CG (p=0.008)]. All women were amenorrheicafterHSCT.There wasnoassociation of BMDwiththediagnosis oftheunderlyingdisease (p=0.09), type of HSCT (p=0.805), conditioning regimen (p=0.329),
100%
90%
80% 89%
33%
P=0.004
Non-Sarcopenic
11% 67% 70%
60%
50%
40%
30%
20%
10%
0%
Sarcopenic
Graft Versus Host Disease grade 0, I, or II
Graft Versus Host Disease grade III or II
Patients (%
)
Figure3–Diagnosisofpre-sarcopeniaaccordingtothe degreeofthegraft-versus-hostdisease.
immunoprophylaxis (p=0.126),presenceofGVHD(p=0.417), cumulativedoseofcorticosteroid(p=0.416)oranyparameter offoodintakeorbodycompositionevaluated(p>0.05).
Discussion
This study evaluated lean mass, BMD, and food intake in patientsafterHSCTwiththeresultsshowingahighprevalence ofdecreasedBMDandpre-sarcopenia,especiallyinpatients withGVHDandlowlevelsofvitaminD.
Abnormal BMD was present in 25% of the SG, higher inwomen(40%),and similartothe prevalenceobservedin climactericwomenafterlivertransplantation(14.6%of osteo-porosisand35.4%oflowbonemass).18Variousmechanisms
explainchanges inbonemetabolismafterallogeneicHSCT such as the decreased bone formation related to the pre-HSCTconditioningregimen,aswellasmedicationssuchas cyclosporine and glicocorticoides,19 besides the severity of
the underlyingdisease,that cancompromisebonemineral densityandmusclestrength.20,21 Nevertheless,inthisstudy
neithertheunderlyingdiseasenortheuseofglucocorticoids oranyvariablerelatedtotheHSCTwascorrelatedtotheBMD. AnotherfactorthatmayexplainthehigherprevalenceofBMD changesinwomenisthattheuseofalkylatingagentssuch ascyclophosphamide,methotrexate,and busulfam,withor withoutovarianradiation,leadstoprematureovarianfailure, asnotedin18patientsinthisstudy.Bothchemotherapyand radiotherapyinunder20-year-oldwomenareassociatedwith ahigherprevalenceofearlymenopause:42%ofpatientsby age31comparedto5%incontrols.22,23
TheSGpatientshadlowserumlevelsofvitaminDwith secondaryhyperparathyroidism,and60%ofpatientsreported sporadic sunexposurefollowingmedicaladvicetoprevent GVHDafterHSCT.24 ThishighprevalenceofvitaminD
defi-ciency (77.2%) is similar to that found inrenal transplant patients(79%),alsojustifiedbylowexposuretosun.25
Although the literature associates sarcopenia with advanced age, the patients in this study were young (37.4±12.7years)andpre-sarcopeniawaspresentin15–34%, whichcan havea greatimpact onthe quality oflife. Esti-mationsoftheprevalenceofsarcopeniavarywithage,from 30%inover65-yearoldstomorethan50%inthoseaged80 ormore.25Althoughfewdataareavailableontheprevalence
ofsarcopeniaintheBrazilianpopulation,itisclearthatthe studypopulationhad sarcopeniaatalower ageand itwas moreprevalent inthe firstfive yearsafter transplantation. Studiesonhumansandanimalshaveshownmusclewasting andcachexiarelatedtocancer27–29possiblyduetothe
oxida-tivestressandchronicinflammationimmediatelyafterHSCT. Inthisstudy,theexclusionofpatientswhounderwentHSCT lessthanoneyearpriortotheevaluationwasanattemptto eliminatetheimpactofacutecomplicationsofHSCTon sar-copeniaandBMD.Sarcopeniawasobservedin66.2%patients before liver transplantation, with 75% of patients without sarcopeniabeforethetransplantdevelopingthediseaseafter withinamean of 19.3±9months; no association between nutritional status and post-transplant factors such as the immunosuppressionregimenwereidentified.30Inthisstudy,
wedidnotfindanyrelationshipoftheconditioningregimen or the use of immunosuppression with the prevalence of sarcopenia.
The diagnostic criteria were concordant with a higher prevalenceofpre-sarcopeniaintheSG.However,themethod proposedbytheFINHprovedtobemoreconservativeinboth groups,comparedtotheBaungartnerand Delmonico crite-ria.Furthermore, the clinicalcorrelation observed between theseverityofGVHDandthediagnosisofpre-sarcopeniawas observedonlywiththeFNIHmethod,whichhasimportant clinicalrelevanceforthesepatients.
Conclusion
PatientsundergoingallogeneicHSCThadahigherprevalence ofBMDchangesandhigherpre-sarcopeniarateswhen com-paredtothecontrols.ConcerningthefactorsrelatedtoHSCT, thepresenceofsevere GVHDwasassociatedwithahigher prevalenceofpre-sarcopenia.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. SternJM,SullivanKM,OttSM,SeidelK,FinkJC,LongtonG, etal.Bonedensitylossafterallogeneichematopoieticstem celltransplantation:aprospectivestudy.BiolBloodMarrow Transplant.2001;7(5):257–64.
2. ChemaitillyW,BouladF,OeffingerKC,SklarCA.Disordersof glucosehomeostasisinyoungadultstreatedwithtotalbody irradiationduringchildhood:apilotstudy.BoneMarrow Transplant.2009;44(6):339–43.
3. BakerKS,GurneyJG,NessKK,BhatiaR,FormanSJ,Francisco L,etal.Lateeffectsinsurvivorsofchronicmyeloidleukemia
treatedwithhematopoieticcelltransplantation:resultsfrom theBoneMarrowTransplantSurvivorStudy.Blood.2004Sep 15;104(6):1898–906.
4.PierineDT,NicolaM,OliveiraEP.Sarcopenia:alterac¸ões metabólicaseconsequênciasnoenvelhecimento.RBrasCie Mov.2009;17(3):96–103.
5.SavaniBN,DonohueT,KozanasE,ShenoyA,SinghAK,Childs RW,etal.Increasedriskofbonelosswithoutfractureriskin long-termsurvivorsafterallogeneicstemcell
transplantation.BiolBloodMarrowTransplant. 2007;13(5):517–20.
6.KasteSC,ShidlerTJ,TongX,SrivastavaDK,RochesterR, HudsonMM,etal.Bonemineraldensityandosteonecrosisin survivorsofchildhoodallogeneicbonemarrow
transplantation.BoneMarrowTransplant.2004;33(4): 435–41.
7.EnglesbeMJ,PatelSP,HeK,LynchRJ,SchaubelDE,Harbaugh C,etal.Sarcopeniaandmortalityafterlivertransplantation.J AmCollSurg.2010;211(2):271–8.
8.CareyEJ.Sarcopeniainsolidorgantransplantation.NutrClin Pract.2014;29(2):159–70.
9.TeixeiraVO,FilippinLI,XavierRM.Mecanismosdeperda musculardasarcopenia.RevBrasReumatol.
2012;52(2):247–59.
10.SchousboeJT,ShepherdJA,BilezikianJP,BaimS.Executive summaryofthe2013InternationalSocietyforClinical DensitometryPositionDevelopmentConferenceonbone densitometry.JClinDensitom.2013;16(4):455–66. 11.BaumgartnerRN,KoehlerKM,GallagherD,RomeroL,
HeymsfieldSB,RossRR,etal.Epidemiologyofsarcopenia amongtheelderlyinNewMexico.AmJEpidemiol. 1998;147(8):755–63.
12.DelmonicoMJ,HarrisTB,LeeJS,VisserM,NevittM, KritchevskySB,etal.Health,AgingandBodyComposition Study.Alternativedefinitionsofsarcopenia,lowerextremity performance,andfunctionalimpairmentwithaginginolder menandwomen.JAmGeriatrSoc.2007;55(5):769–74. 13.StudenskiSA,PetersKW,AlleyDE,CawthonPM,McLeanRR,
HarrisTB,etal.TheFNIHsarcopeniaproject:rationale,study description,conferencerecommendations,andfinal estimates.JGerontolABiolSciMedSci.2014;69(5): 547–58.
14.WillettW,LenartE.FoodfrequencymethodsinWillettW. NutritionalEpidemiology,Vol.2nded.NewYork:OxfordU. Press;1998.
15.BuenoA,CzepielewskiMA.Orecordatóriode24horascomo instrumentonaavaliac¸ãodoconsumoalimentardecálcio, fósforoevitaminaDemcrianc¸aseadolescentesdebaixa estatura.RevNutr.2010;23(1):65–73.
16.IOM–InstituteofMedicine,FoodandNutritionalBoards. DietaryReferenceIntakeforcalciumandvitaminD.National AcademyPress;2010,448p.
17.HolickMF,BinkleyNC,Bischoff-FerrariHA,GordonCM, HanleyDA,HeaneyRP,etal.Evaluation,treatment,and preventionofvitaminDdeficiency:anEndocrineSociety clinicalpracticeguideline.JClinEndocrinolMetab. 2011;96(7):1911–30.
18.BaccaroLF,BoinIdeF,Costa-PaivaL,LealAG,RamosCD, Pinto-NetoAM.Islivertransplantationassociatedwith decreasedbonemassinclimactericwomen?RevBrasGinecol Obstet.2012;34(7):335–42.
19.ChoiYJ,ParkSY,ChoWK,LeeJW,ChoKS,ParkSH,etal. Factorsrelatedtodecreasedbonemineraldensityin childhoodcancersurvivors.JKoreanMedSci. 2013;28(11):1632–8.
21.HaltonJ,GabouryI,GrantR,AlosN,CummingsEA,Matzinger M,etal.Advancedvertebralfractureamongnewlydiagnosed childrenwithacutelymphoblasticleukemia:resultsofthe CanadianSteroid-AssociatedOsteoporosisinthePediatric Population(STOPP)researchprogram.JBoneMinerRes. 2009;24(7):1326–34.
22.Assumpc¸ãoCR.Falênciaovarianaprecoce.ArqBras EndocrinolMetab.2014;58(2):132–43.
23.ByrneJ,FearsTR,GailMH,PeeD,ConnellyRR,AustinDF, etal.Earlymenopauseinlong-termsurvivorsofcancer duringadolescence.AmJObstetGynecol.1992;166(3):788–93. 24.OliveiraLG,GuimarãesML.Osteoporosenohomem.RevBras
Ortop.2010;45(5):392–5.
25.EwersB,GasbjergA,MoelgaardC,FrederiksenAM,
MarckmannP.VitaminDstatusinkidneytransplantpatients: needforintensifiedroutinesupplementation.AmJClinNutr. 2008;87(2):431–7.
26.Mostoufi-MoabS,GinsbergJP,BuninN,ZemelBS,ShultsJ, ThayuM,etal.Bodycompositionabnormalitiesinlong-term survivorsofpediatrichematopoieticstemcell
transplantation.JPediatr.2012;160(1):122–8.
27.EvansWJ.Skeletalmuscleloss:cachexia,sarcopenia,and inactivity.AmJClinNutr.2010;91(4):1123S–7S.
28.MoylanJS,ReidMB.Oxidativestress,chronicdisease,and musclewasting.MuscleNerve.2007;35(4):411–29. 29.LeiteLE,ResendeTL,NogueiraGM,CruzIB,SchneiderRH,
GottliebGV.Envelhecimento,estresseoxidativoesarcopenia: umaabordagemsistêmica.RevBrasGeriatrGerontol. 2012;15(2):365–80.