w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Review
article
Economy
class
syndrome:
what
is
it
and
who
are
the
individuals
at
risk?
Luci
Maria
SantAna
Dusse
∗,
Marcos
Vinícius
Ferreira
Silva,
Letícia
Gonc¸alves
Freitas,
Milena
Soriano
Marcolino,
Maria
das
Grac¸as
Carvalho
UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received1September2016 Accepted2May2017 Availableonline26May2017
Keywords:
Economyclasssyndrome Airtravel
Thromboembolism Pregnancy
a
b
s
t
r
a
c
t
Theterm‘economyclasssyndrome’referstotheoccurrenceofthromboticeventsduring long-haulflightsthatmainlyoccurinpassengersintheeconomyclassoftheaircraft.This syndromeresultsfromseveralfactorsrelatedtotheaircraftcabin(immobilization, hypo-barichypoxiaandlowhumidity)andthepassenger(bodymassindex,thrombophilia,oral contraceptivesorhormonereplacementtherapy,cancer),actingtogethertopredisposeto excessivebloodcoagulation,whichcanresultinvenousthromboembolism.Severalrisk fac-tors,bothgeneticandacquired,areassociatedwithvenousthromboembolism.Themost importantgeneticriskfactorsarenaturalanticoagulantdeficiencies(antithrombin, pro-teinCandproteinS),factorVLeiden,prothrombin andfibrinogengenemutationsand non-Obloodgroupindividuals.Acquiredriskfactorsincludeage,pregnancy,surgery, obe-sity,cancer,hormonalcontraceptivesandhormonereplacementtherapy,antiphospholipid syndrome,infections,immobilizationandsmoking.Peoplewhohavetheseriskfactorsare predisposedtohypercoagulabilityandaremoresusceptibletosuffervenous thromboem-bolismduringairtravel.Fortheseindividuals,asuitableoutfitforthetrip,frequentwalks, calfmuscleexercises,elasticcompressionstockingsandhydrationareimportant preven-tivemeasures.Hence,itisessentialtoinformabouteconomicclasssyndromeinanattempt toencourageBrazilianhealthandtransportauthoritiestoadoptmeasures,inpartnership withthepharmaceuticalindustry,topreventvenousthromboembolism.
©2017Associac¸ ˜aoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Venousthromboembolism(VTE) isa clinicalconditionthat involves two related situations, venous thrombosis and
∗ Correspondingauthorat:FacultyofPharmacy,UniversidadeFederaldeMinasGerais(UFMG),Room4104-B3,Av.AntônioCarlos,6627,
CampusPampulha,31270-901BeloHorizonte,MG,Brazil. E-mailaddress:[email protected](L.M.Dusse).
pulmonary embolism.1 Itaffects approximately 2–3 people
per1000individualsperyear.VTEisthethirdcauseofdeath byvasculardiseases,onlysurpassedbymyocardialinfarction andischemicstroke.Inaddition,itisthemostcommoncause ofpreventabledeathinhospitalizedpatients.2,3
http://dx.doi.org/10.1016/j.bjhh.2017.05.001
Theterm ‘economyclasssyndrome’referstothe occur-renceofthromboticeventsduringlong-haulflights,mainly in economyclass passengers. This syndrome results from severalfactorsrelatedtothe aircraftcabin(immobilization, hypobarichypoxiaandlowhumidity)andtothepassenger (suchasobesity,thrombophilia,oralcontraceptiveuse, hor-mone replacement therapy and cancer), that act together predisposingtoexcessivebloodcoagulation,whichcanresult inVTE.4
Severalriskfactors,bothgeneticandacquired,are asso-ciated with VTE. The most important genetic risk factors are natural anticoagulant deficiencies: (1) Deficiency of antithrombin,proteinCorproteinS;(2)FactorV(FV)Leiden, whichisresistanttoproteinCinactivation;(3)TheG20210A mutationintheprothrombingene,whichleadstoanincrease ingeneexpressionandprothrombin plasmalevels;(4) The C10034T mutation in the fibrinogen gene, which produces avariantformoffibrinogen;and (5)Non-Oblood group(A, BandAB)asindividualshavehighervonWillebrandfactor andfactorVIIIplasmalevelsthanOgroupsubjectsandhave increasedriskofthrombosis.
Acquired risk factors include age, pregnancy, surgery, obesity, cancer, hormonal contraceptives and hormone replacementtherapy,antiphospholipidsyndrome,infections, immobilizationandsmoking.5,6
Venous
thromboembolism
and
air
travel
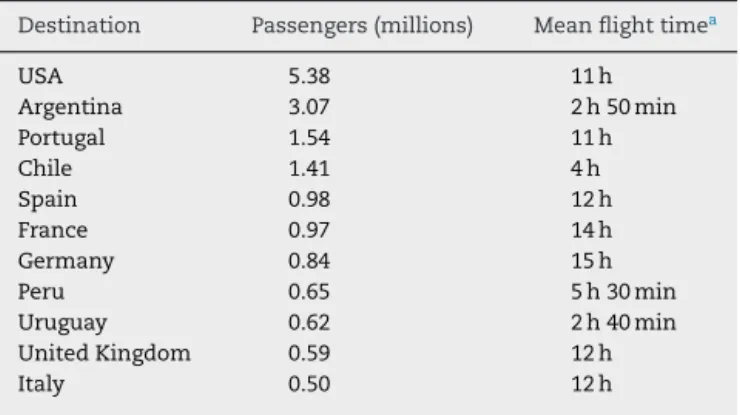
DatafromtheBrazilianNationalCivilAviationAgency(ANAC) revealedthatthenumberofpassengerscarriedbycivil avia-tionin2015surpassed100million.7Tables1and28–10show
themaindomesticandinternationalflightsinandfromBrazil in2015.Theaircraftmicroenvironmentprovidesveryspecific conditions,suchasreducedoxygentension,immobilization (ingeneral,peopleareintightuncomfortableseats)and cir-cadiandysrhythmia,duetodifferencesintimezones(jetlag).
Table1–MajordomesticflightsofBrazilin2015.
Route Passengers
(millions)
Meanflight time
SãoPaulo(CGH)–Riode Janeiro(SDU)
4.05 1h
SãoPaulo(CGH)–Brasília(BSB) 2.23 1h45min SãoPaulo(GRU)–Salvador
(SSA)
2.2 2h20min
SãoPaulo(GRU)–PortoAlegre (POA)
2.02 1h35min
SãoPaulo(GRU)–Recife(REC) 1.98 3h30min SãoPaulo(CGH)–Belo
Horizonte(CNF)
1.82 1h20min
SãoPaulo(CGH)–PortoAlegre (POA)
1.7 1h35min
SãoPaulo(CGH)–Curitiba (CWB)
1.52 1h00min
SãoPaulo(CGH)–Brasília(BSB) 1.35 1h45min RiodeJaneiro(GIG)–Salvador
(SSA)
1.34 2h15min
Total 20.21
Table2–MajorinternationalflightsfromBrazilin2015.
Destination Passengers(millions) Meanflighttimea
USA 5.38 11h
Argentina 3.07 2h50min
Portugal 1.54 11h
Chile 1.41 4h
Spain 0.98 12h
France 0.97 14h
Germany 0.84 15h
Peru 0.65 5h30min
Uruguay 0.62 2h40min
UnitedKingdom 0.59 12h
Italy 0.50 12h
a FlighttimedepartingfromthecityofSãoPaulo.
These factors may disturb the passenger’s health, causing fatigue,anxietyandnausea.11,12
The first cases of VTE associated with air travel were reported in 1954, and since then, other cases have been described.4 The vast majority of victims suffer pulmonary
embolismand/ordeepveinthrombosis,butcasesof subcla-vianveinthrombosis,13cerebralveinthrombosis,14strokeand
arterialthrombosis15havealsobeenreported.
TheactualincidenceofVTEinairtravelisunknown.Itis difficulttoarriveatanestimationgiventhatthiscondition may beasymptomatic or maydevelopdays orevenweeks aftertheflight.16Inacohortofhealthysubjects,theabsolute
riskofVTEonflightslastingmorethan4hwas1in6000.17
A meta-analysis18 involving14 studies reported4055cases
ofVTEintripslastingupto8h.Thesestudiesincludedboth airandoverlandtripswiththefollow-uptimeafterthe jour-neyrangingfromtwotoeightweeks.TherelativeriskofVTE was2.8[95%confidenceinterval(95%CI):2.2–3.7]andateach incrementof2hintraveltime,therewasanapproximate18% increaseintheriskofVTE.Consideringonlyairtravel,thisrisk increasedto26%,suggestingacumulativeeffectofflighttime inthegenesisofVTE.
MacCallumetal.19demonstratedthatonflightslastingless
than 4h,theriskofVTEisapproximatelytwotimeshigher comparedtonon-travelersubjects[oddsratio(OR):2.20;95% CI:1.29–3.73]andremainedhighinthefoursubsequentweeks. Inlong-haulflights(greaterthan12hasoneormoreflights), theriskofVTEisaroundthreetimeshigher(OR:2.75;95%CI: 1.44–5.28).After12weeks,notime-flighteffectwasobserved intheoccurrenceofthromboticevents.
A number of factors associated both to the aircraft or passengershavebeensingledoutasresponsiblefor trigger-ingVTE.20Stasisandhypercoagulability,twocomponentsof
Virchow’striad,haveacrucialroleintheoccurrenceof throm-boembolisminflights.18
Thefactorsassociatedwiththeaircraftinclude:
• Hypobarichypoxia:Thehypoxiacausedbyreducedair
the pressure is usually 570mmHg and the partial oxy-genpressureis125mmHg,resultinginoxygensaturation of90–93%. However,intheelderly and peoplewithlung and/orheartdiseases,reductionsofupto80% ofoxygen saturation canoccur. Therelativehypoxiainthe aircraft leadstoadecreaseinfibrinolyticactivityandtherelease of venous relaxationfactors,which help toincrease the hemostasis.12
• Lowhumidity:Therelativehumidityinsidetheaircraftis
approximately10%,whileatsealevelis30–40%.Low humid-ity isassociatedwithincreasesinplasmaticandurinary osmolarity,whichresultinhemoconcentrationthatfavors VTE.12
Themainpassenger-relatedfactorsare:
• Immobilization: Lackofmovement inthesitting position
duringtheflightresultsinhemostasisofthelowerlimbs predisposing the individual to VTE.12 An evaluation of
coagulationbiomarkersshowedthatthereisanincreased generationofthrombinduringflightslastingmorethan8h; thisdoesnotoccurinothersituationswherethesubjectis immobilizedinthesittingposition.Itsuggeststhatthere isanadditionalmechanismresultinginhypercoagulability duringflights.20
• Body mass index (BMI) and height: In obese subjects
(BMI>30kg/m2),thereisareductioninbloodflowinthe
lowerlimbs,favoringhemostasis.Ithasbeenobservedthat individualsattheextremesofstature(>1.90mor<1.60m) haveanincreasedriskofVTEduringairtravel.12
• Thrombophilia: Thepresenceofgeneticthrombophilia is
anindependentriskfactorforVTE.Martinellietal.reported thattheriskofVTEis6.6(95%CI:3.9–11.3)timeshigherin patientswiththrombophilia,comparedtoindividuals with-out thesemutations.Inpatientswiththrombophilia,the riskofVTEwas16.8timeshigher(95%CI:3.8–74.7), com-paredtonon-thrombophilic,non-travelers,whichsuggests asynergisticinteractionresultinginanincreasein throm-boticrisk.21
• Oralcontraceptivesandhormonereplacementtherapy:The
useoforalcontraceptivesincreasestheriskofVTEbyabout fourfoldinthegeneralpopulation(OR:4.2;95%CI:1.9–9.3). Asynergisticassociationbetweenairtravelandoral con-traceptiveuseinthegenesisofVTEcanbeinferredsince theoccurrenceofthrombosisishighinwomenunderoral contraceptivesuseduringorafterairtravel(OR:23.4;95% CI:2.6–11.2).Similarly,hormonereplacementtherapy pre-disposestoVTE.2
• Cancer:Itiswellestablishedthatcancerpatientshavean
increasedriskofdevelopingVTEthroughoutthehistoryof thedisease,mainlyinthefirstthreemonthsafterthe ini-tialdiagnosis(OR:53.5;95%CI:8.6–334.3).22Kuipersetal.23
estimatedthatthepresenceofamalignantdiseaseis asso-ciatedtoan18-foldincreaseinthromboembolicriskduring flights.
• Otherfactors:Althoughitisadmittedthatfactorssuchas
diabetesandsmokingareassociatedwitha hypercoagula-blestate,24thereisalackofstudiesabouttheassociation
of these conditions and the incidence of VTE during flights.
Pregnancy,
air
travel
and
venous
thrombosis
Pregnancy progresseswithimportantphysiologicalchanges inthehemostaticsystem,whichdeterminesa hypercoagula-blestate.Theseadaptivechangesaimtopreparethematernal organismtothegreathemostaticchallengeofplacenta expul-sionandsimultaneousdisruptionofnumerousbloodvessels topreventexcessivebleeding.25
Literaturedatasuggestthat1:6000youngpassengers with-outriskfactorsforthrombosishaveariskofsymptomaticVTE inafour-hourflight.26Pregnantwomeninfour-hourflights
have a thromboembolic risk five to ten times higher than non-pregnantwomenhave.Thisriskrisesexponentiallyon long-haultrips,byaroundfourfoldandeightfoldiftheflight timeexceedseightor12h,respectively.26
Forpregnantwomenwiththrombophiliawhoflyover4h, thethromboembolicriskis1:200.ForwomenwithFactorV Lei-deninhomozygosisorthoseheterozygosisforbothFactorV Leidenandtheprothrombinmutation,theriskisabout1:40.26
In addition to genetic thrombophilia, parturients with an acquiredthrombophiliasuchasantiphospholipidsyndrome alsohaveanincreasedriskforVTE.Thesefindingsraisethe debateabouttherelevanceoftheadoptionofpharmacological prophylaxisinpregnantwomenwhileflying.27,28
Ithasbeenreportedthathypoxiaduringflightsand, conse-quentlytrophoblasticinjury,favorstheoccurrenceofpreterm birthandintrauterinedeath,especiallyinpregnantwomen agedover35years,withpreeclampsia,abruptioplacentaeor intrauterinegrowthrestriction.29
Aware of the risks, many commercial airlines allow pregnantwomentotravelonlyuptothe36thweekof preg-nancy.Other companiesmakerestrictionsforinternational flights in early pregnancy and require evidentiary docu-mentationofgestational age orstate thatcases shouldbe evaluatedindividually.Pregnantcivilianormilitary crewmem-bers should check with regulatory bodies with regard to restrictionsontheirprofessionalactivities.However,themain concernwithpregnantwomenofairlinesisassociatedwith the risk of labor during the trip, which could disrupt or interrupttheflight.Inaddition,thereisalackofskilled profes-sionalstomanageobstetriccomplicationsoccurringaboard.27
Obstetricians advise at-risk pregnant women notto fly. All pregnant women should be informed of the obstetric emergenciesthatcanoccurinthefirstandthirdtrimesters ofpregnancyand itisprudenttoavoidtravelduringthese periods.30
Table3–Riskcategoriesfortheoccurrenceof thromboembolicevents.
Risk Riskcategory
Low Ageover40years,obesity,inflammatorydisease, recentminorsurgery(withinthreedays)
Moderate Varicoseveins,decompensatedheartfailure, recentacutemyocardialinfarction(withinsix weeks),hormonetherapy(including contraceptives),pregnancyorthepostpartum period,lowerlimbhemiparesis,lowerlimb trauma(withinsixweeks)
High Previousvenousthromboembolism,known thrombophilia,recentmajorsurgery(withinsix weeks),priorstroke,cancer,familyhistoryof venousthromboembolism.
Thechoiceofasuitableoutfitforthe tripisalso impor-tantandmustprioritizecomfort,avoidingtightgarmentswith elastic.Adequatehydrationshouldbeencouraged.27
Individualriskstratificationisessentialtodefinethemost appropriate measures. The Aerospace Medical Association (AsMA)haspublished guidelineson theuse ofprophylaxis inindividualswho travelbyair.Theriskgroupsdefinedin theseguidelinesareshowninTable3.31 Pregnancyandthe
puerperiumaredefinedasmoderaterisk.Forindividualswith moderaterisk,theguidelinessuggestacetylsalicylicacid asso-ciated or not with compression stockings.32 However, the
evidenceaboutacetylsalicylicaciduseiscontroversialasit crossestheplacentaandthereforeitcannotberecommended prophylacticallyinpregnantwomenaccordingtothe Ameri-canCollegeofChestPhysiciansGuidelines.33
Elastic compression stockings exert graduated pressure ofthelower limbwithgreaterpressureattheankle.When combined with muscle activity,they direct the blood flow from the superficial venous system to the deep system, reducingvenousstasisandpotentiallypreventingthe occur-renceofvenousthrombosis.ACochranesystematicreview includednine randomizedtrials(2821 individuals) compar-ingflyerswho usedcompressionstockingswiththosewho didnot(sevenstudies inlow-ormedium-risk individuals). Thestudynotedasignificantreductionintheriskof asymp-tomatictravel-relateddeepvenousthrombosiswiththeuse ofcompressionstockings(OR:0.10;95%CI:0.05–0.25).15The
tolerabilityofcompressionstockingswasgoodinallstudies andnoadverseeffectswerereportedwiththeexceptionof superficialthrombophlebitis.15,34
For high-risk individuals, frequent walking, calf mus-cle exercises and compression stockings should be encouraged.27,31
Despite the factthat thrombophilia constitutes a major riskfactor forVTE, routinescreening isnotrecommended inpregnantwomen,sincetherearemultipleriskfactorsin pregnantwomen(eventhougheachindividualfactorisnot associatedtohighrisk).35
ConsideringthelargeextensionoftheBrazilianterritory, thrombosisduringlongoverlandtrips(withimmobilization inasitting position)should beexpectedhoweveronlyone
casereportwasfoundintheBrazilianliteratureconcerning theoccurrenceofathromboembolicevent.36
Final
considerations
InthecontextofBrazil,themajorityofdomesticflightslast lessthan2h,althoughtripsfromthesouthtothenorthand northeastcanlastfrom8to10h.Withrespecttointernational travel,mostflightsareoflongdurationandthusrepresenta greaterriskofVTE.Despitethis,thereisnodataabout Brazil-ianindividualswhotravelwithariskofhypercoagulabilityor aboutVTErelatedtoflights.
Itisessentialtoinformabouteconomicclasssyndrome inanattempttoencouragetheBrazilianhealthand trans-portauthoritiestoadoptsomemeasures,inpartnershipwith thepharmaceuticalindustry,topreventvenous thromboem-bolism.
Acknowledgments
Theauthorsthankthefinancialsupportgrantedbythe Con-selhoNacionaldeDesenvolvimentoCientíficoeTecnológico (CNPq) and Fundac¸ão de Amparo à Pesquisa doestado de MinasGerais(FAPEMIG).LSDandMGCaregratefultoCNPq forprovidingResearchFellowships.
r
e
f
e
r
e
n
c
e
s
1.TapsonVF.Acutepulmonaryembolism.NEnglJMed. 2008;358(10):1037–52.
2.ReitsmaPH,VersteegHH,MiddeldorpS.Mechanisticviewof riskfactorsforvenousthromboembolism.Arterioscler ThrombVascBiol.2012;32(3):563–8.
3.TakachLapnerS,KearonC.Diagnosisandmanagementof pulmonaryembolism.BMJ.2013;346:f757.
4.MendisS,YachD,AlwanA.Airtravelandvenous
thromboembolism.BullWorldHealthOrg.2002;80(5):403–6. 5.MackmanN.Newinsightsintothemechanismsofvenous
thrombosis.JClinInvest.2012;122(7):2331–6.
6.AlpoimPN,deBarrosPinheiroM,JunqueiraDR,FreitasLG, dasGrac¸asCarvalhoM,FernandesAP,etal.Preeclampsiaand ABObloodgroups:asystematicreviewandmeta-analysis. MolBiolRep.2013;40(3):2253–61.
7.BRASIL.AgênciaNacionaldeAviac¸ãoCivil.DemandaeOferta doTransporteAéreo–EmpresasBrasileiras-Dezembrode 2015.[Internet]2016[cited2017February12].Availablefrom: http://www.anac.gov.br/assuntos/dados-e-estatisticas/ mercado-do-transporte-aereo.
8.GOL–VRGLinhasAéreasS/A.[Internet]2013[cited2013May 11]Availablefrom:http://www.voegol.com.br/pt-br/Paginas/ default.aspx.
9.TAM.–TAMLinhasAéreasS/A–StarAllianceMember. [Internet]2013[cited2013May11]Availablefrom: http://www.tam.com.br/b2c/vgn/v/index.jsp?vgnextoid= 97981ed526b72210VgnVCM1000003752070aRCRD.
10.BRASIL.AnuáriodoTransporteAéreo2015,volumeúnico,1a
edic¸ão.AgênciaNacionaldeAviac¸ãoCivil.[Internet]2016 [cited2017February12]Availablefrom:http://www.anac. gov.br/assuntos/dados-e-estatisticas/mercado-do-transporte-aereo.
adaptationstoexerciseinpregnancyatsealevelandaltitude. AmJObstetGynecol.1995;1724Pt1:1170–8[discussion 1178–80].
12.SandorT.Travelthrombosis:pathomechanismsandclinical aspects.Pathophysiology.2008;15(4):243–52.
13.TeruyaT,ArfvidssonB,EklofB.Couldprolongedairtravelbe casuallyassociatedwithsubclavianveinthrombosis.JTravel Med.2002;9(1):17–9.
14.PfauslerB,VollertH,BoschS,SchmutzhardE.Cerebral venousthrombosis–anewdiagnosisintravelmedicine?J TravelMed.1996;3(3):165–7.
15.KakkosSK,GeroulakosG.Economyclassstrokesyndrome: casereportandreviewoftheliterature.EurJVascEndovasc Surg.2004;27(3):239–43.
16.ClarkeM,HopewellS,JuszczakE,EisingaA,KjeldstromM. Compressionstockingsforpreventingdeepveinthrombosis inairlinepassengers.CochraneDatabaseSystRev.
2006;(2):Cd004002.
17.WorldHealthOrganization(WHO).WrightProject.[Internet] 2013[cited2013May11]Availablefrom:http://www.who.int/ cardiovasculardiseases/wrightproject/phase1report/ WRIGHT%20REPORT.pdf.
18.ChandraD,ParisiniE,MozaffarianD.Meta-analysis:travel andriskforvenousthromboembolism.AnnInternMed. 2009;151(3):180–90.
19.MacCallumPK,AshbyD,HennessyEM,LetleyL,MartinJ, Mt-IsaS,etal.Cumulativeflyingtimeandriskofvenous thromboembolism.BrJHaematol.2011;155(5):613–9. 20.SchreijerAJ,CannegieterSC,MeijersJC,MiddeldorpS,Buller
HR,RosendaalFR.Activationofcoagulationsystemduringair travel:acrossoverstudy.Lancet.2006;367(9513):832–8. 21.MartinelliI,TaioliE,BattaglioliT,PoddaGM,PassamontiSM,
PedottiP,etal.Riskofvenousthromboembolismafterair travel:interactionwiththrombophiliaandoral
contraceptives.ArchInternMed.2003;163(22):2771–4. 22.KhoranaAA.Cancerandcoagulation.AmJHematol.2012;87
Suppl.1:S82–7.
23.KuipersS,VenemansA,MiddeldorpS,BüllerHR,Cannegieter SC,RosendaalFR.Theriskofvenousthrombosisafterair travel:contributionofclinicalriskfactors.BrJHaematol. 2014;165(3):412–3.
24.DominguetiCP,DusseLM,CarvalhoMddeSousaLP,Gomes KB,FernandesAP.Diabetesmellitus:thelinkagebetween oxidativestress,inflammation,hypercoagulabilityand vascularcomplications.JDiabetesCompl.2016;30(4):738–45. 25.BrennerB.Haemostaticchangesinpregnancy.ThrombRes.
2004;114(5-6):409–14.
26.CannegieterSC,RosendaalFR.Pregnancyandtravel-related thromboembolism.ThrombRes.2013;131Suppl.1:S55–8. 27.BrennerB.Prophylaxisoftravel-relatedthrombosisin
women.ThrombRes.2009;123Suppl.3:S26–9.
28.CannegieterSC,DoggenCJ,vanHouwelingenHC,Rosendaal FR.Travel-relatedvenousthrombosis:resultsfromalarge population-basedcasecontrolstudy(MEGAstudy).PLoSMed. 2006;3(8):e307.
29.BrennerB.Interventionstopreventvenousthrombosisafter airtravel,aretheynecessary?Yes.JThrombHaemost. 2006;4(11):2302–5.
30.PracticeA.CoO.ACOGCommitteeOpinionNo443:airtravel duringpregnancy.ObstetGynecol.2009;114(4):954–5. 31.MoyleJ.Medicalguidelinesforairlinetravel.AviatSpace
EnvironMed.2003;74(9):1009[authorreply1009]. 32.MedicalGuidelinesforAirlineTravel,2nded.AviatSpace
EnvironMed.2003;74(5Suppl):A1–19.
33.GeertsWH,BergqvistD,PineoGF,HeitJA,SamamaCM, LassenMR,etal.Preventionofvenousthromboembolism: AmericanCollegeofChestPhysiciansEvidence-Based ClinicalPracticeGuidelines(8thEdition).Chest.2008;1336 Suppl.:381s–453s.
34.ScurrJH,MachinSJ,Bailey-KingS,MackieIJ,McDonaldS, SmithPD.Frequencyandpreventionofsymptomless deep-veinthrombosisinlong-haulflights:arandomisedtrial. Lancet.2001;357(9267):1485–9.
35.BatesSM,GreerIA,MiddeldorpS,VeenstraDL,PrabulosAM, VandvikPO.VTE,thrombophilia,antithrombotictherapy,and pregnancy:AntithromboticTherapyandPreventionof Thrombosis,9thed:AmericanCollegeofChestPhysicians Evidence-BasedClinicalPracticeGuidelines.Chest.2012;1412 Suppl.:e691S–736S.