rev bras hematol hemoter. 2017;39(4):357–359
w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Case
Report
Autoimmune
hemolytic
anemia
and
hyperglobulinemia
leading
to
the
diagnosis
of
multiple
myeloma
Rafael
Lopes
Pacca
a,∗,
Jiviane
Beatriz
Cunha
Barretto
da
Silva
b,
Kallen
de
Carvalho
e
Souza
a,
Rebeca
Barbosa
Carbinatto
aaPontíficeUniversidadeCatólicadeCampinas(PUC),Campinas,SP,Brazil
bClínicaMédicaMedeiros,Campinas,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received29December2016
Accepted17July2017
Availableonline4September2017
Introduction
Autoimmunehemolyticanemia(AIHA)isaconditioninwhich
self-antibodiesboundtoantigensonthemembranesofred
bloodcellsinitiatetheirdestruction(hemolysis)viathe
com-plementandreticuloendothelialsystems.Multiplemyeloma
(MM),ontheotherhand,ischaracterizedbyaclonal
expan-sion ofplasma cells in bone marrow, causing bone tissue
destruction, renal failure and hematopoietic suppression.
AlthoughtheassociationofMMandanemiaiscommon,AIHA
astheanemicmanifestationofMMisrare.1
Case
report
Herein we report on the case of a 69-year-old, black
patientundertreatmentwithprednisoneandmethotrexate
∗ Correspondingauthorat:BancodeSanguedeSertãozinhoRuaEpitácioPessoa1401,Centro,14160-180Sertãozinho,SP,Brazil.
E-mailaddress:[email protected](R.L.Pacca).
for rheumatoid arthritis over the ten years leading up to
this report. Six years ago, the patient was investigatedby
the hematology department due to an unstable
leukope-nia (2.86×103/L), without the involvement of any other
series. Since the beginning of treatment for rheumatoid
arthritis,theleukocyte countofthepatientwascontrolled,
withvariationsbeingattributedtotherheumatoidarthritis
itself.
However, other alterations were found duringa routine
appointment in the Rheumatology Department including
anemia(hemoglobin:7.2g/dL),low hematocrit(22.6%), high
ferritinlevels(732mg/dL),positivedirectcoombstest,and
ele-vatedtotalandindirectbilirubin.Byproteinelectrophoresis,
thetotalproteinwaselevated(11.8g/dL),thealbumin/globulin
ratiowaslow(0.50),thealbuminwaslow(3.94g/dL)andthe
gammaglobulinwashigh(6.25g/dL)withamonoclonal
com-ponent. The patient was referred back to the hematology
department and diagnosed with hypergammaglobulinemia
http://dx.doi.org/10.1016/j.bjhh.2017.07.005
1516-8484/©2017Associac¸ ˜aoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.PublishedbyElsevierEditoraLtda.Thisisan
358
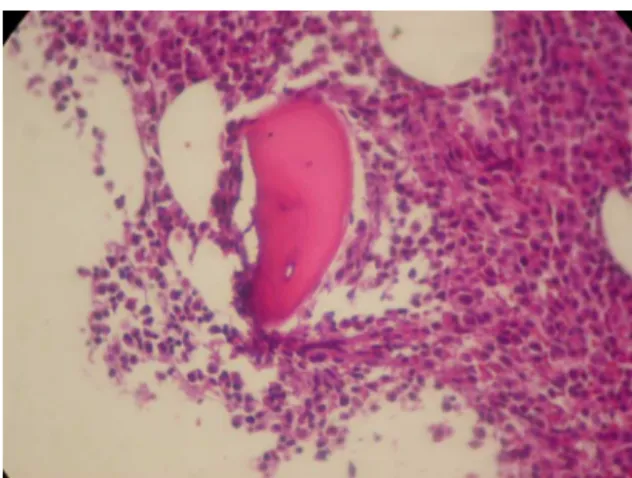
revbrashematolhemoter.2017;39(4):357–359Figure1–Hypercellularbonemarrowattheexpenseof plasmacellinfiltration(Hematoxylinandeosinstain: Magnification:100×).
Figure2–CD138plusplasmocytes.
andAIHAatwhichtimeabonemarrowbiopsywasperformed
thatidentifiedMM(Figures1and2).
Discussion
Normocyticand normochromicanemia, withmultifactorial
origin, such as a red cell series maturation disorder, iron
deficiency,decreasederythropoietinresponseor
erythropoi-etindeficiency, isafrequentfinding inpatientswithMM.2
AIHAisoftenassociatedwithBcelllymphoproliferative
dis-orders.Itcanbeobservedinapproximately8–15%ofpatients
with chronic lymphocytic leukemia (CLL),3 as well as in
otherpathologiessuchasnon-Hodgkinlymphomaincluding
Waldenstrom’smacroglobulinemia,4butitsconnectionwith
MMhasnotyet beenwell elucidated.AreviewbyPirofsky
40years ago showedthatonly4%ofAIHAcaseswere due
toMM.5 There are lessthan adozenreported cases,6 with
nonebeingBrazilian,butrecentlyaprospectivestudywas
car-riedoutthatshowedthat10.6%ofpatientswithMMhadtheir
pathologycomplicatedbyAHAI.4Despitethis,anacceptable
conclusionhasnotyetbeenreachedaboutthepathogenesis
thatrelatesthesetwoconditions.ThefactthatMMisaBcell
disease,similartoCLL,whichismoreassociatedwithAHAI,
isbeingtakenintoaccounttoconductsomestudies.7Oneof
thehypothesesisthedevelopmentofautoantibody-producing
clonesagainstthesurfaceantigensofredbloodcells,
origi-natingfromthesignificantimmunedisordercausedbyMM.7
However, no study hasbeen able to provethat the
mono-clonalprotein,ofwhichveryhighlevelsareseeninMM,isthe
antibodyresponsibleforAHAIandthe pathogenesisofthis
progressionisstillunclear.8Moreover,duetothelackof
con-cretedata,thepossibilityofthispathogenesis,thatis,AHAI
asthecause ofMMcannotberuledout.8 Theinvolvement
ofimmunosuppressants,suchasinterferon-alpha,whichare
usedinthetreatmentofMMandotherlymphoproliferative
disorders,mayalsoplayanimportantroleinthedevelopment
ofAHAI,anautoimmunephenomenonsimilartoEvans-like
syndrome.9 Thenumberofreportedcasesisextremelylow,
whichrestrictstheprogressofresearch.
Conclusion
Thiscase describesarare condition, AIHAassociatedwith
MM.Thelownumberofreportedcasesandconsequentlythe
few studieson thisassociation hindersourunderstanding.
However,ongoingstudiesshouldclarifyboththepathogenesis
andtheintimacyoftherelationshipbetweenthetwoentities
inthefuture,therebyallowingearlierdiagnosisandtreatment
thatismoreeffective.Themedicalcommunityshould
con-sider thediagnosis ofAHAIinthe presenceofMM aswell
asvice versa,inordertomakeearlierdiagnosesand
treat-mentsthataremoreeffective.Inaddition,newcasesneedto
bereportedtosupportresearchrelatedtothesetwo
patholo-gies, sothat throughalargeranalysis, sciencecan reacha
coherentandeffectiveconclusion.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.FriedlandM,SchaeferP.Myelomatosisandhemolyticanemia. Hemolyticanemia,ararecomplicationofmultiplemyeloma, issuccessfullymanagedbysplenectomy.RIMedJ.
1979;62(12):469–71.
2.SilvestrisF,CafforioP,TucciM,DammaccoF.Negative regulationoferythroblastmaturationbyFas-L+/TRAIL+highly malignantplasmacells:amajorpathogeneticmechanismof anemiainmultiplemyeloma.Blood.2002;99(4):1305–13.
3.PatelR,SalamassiS.Possibleautoimmunehemolysiswith multiplemyeloma:acasereportwithreviewoftheliterature. Blood.1987;70suppl1:113.
4.KashyapR,SinghA,KumarP.Prevalenceofautoimmune hemolyticanemiainmultiplemyeloma:aprospectivestudy. AsiaPacJClinOncol.2016;12(2):e319–22.
5.PirofskyB.Clinicalaspectsofautoimmunehemolyticanemia. SeminHematol.1976;13(4):251–65.
revbrashematolhemoter.2017;39(4):357–359
359
7.VaiopoulosG,KyriakouD,PapadakiH,FessasP,EliopoulosGD. Multiplemyelomaassociatedwithautoimmunehemolytic anemia.Haematologica.1994;79(3):262–4.
8.WadaH,YataK,MikamiM,SuemoriS,NakanishiH,KondoT, etal.Multiplemyelomacomplicatedbyautoimmune hemolyticanemia.InternMed.2004;43(7):595–8.