SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Septic
arthritis
and
arthropathy
of
the
rotator
cuff:
remember
this
association
夽
Danilo
Sobreira
∗,
Neydson
de
Souza,
José
Inácio
de
Almeida,
Alberto
de
Castro
Pochini,
Carlos
Vicente
Andreoli,
Benno
Ejnisman
UniversidadeFederaldeSãoPaulo,EscolaPaulistadeMedicina,DepartamentodeOrtopediaeTraumatologia, CentrodeTraumatologiadoEsporte,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received31May2015 Accepted25September2015 Availableonline29June2016
Keywords: Jointdiseases Rotatorcuff Arthritisinfectious Arthroscopy
a
b
s
t
r
a
c
t
Objective:Todescribeoccurrences ofsepticglenohumeralarthritisamongpatientswith arthropathyoftherotatorcuff,andtohighlighttheimportanceofcorrectdiagnosisand surgicalprocedures.
Methodology:Eight surgical drains were installed in seven patients with glenohumeral pyoarthritis.Allthepatientspresentedarthropathyoftherotatorcuff(fourmalesandthree females).Sixpatientspresentedpyoarthritisinthedominantshoulder.Theagerangewas from53to93years(mean:74years).Themeandurationofthesymptomsbeforethe sur-gicallavagewassixweeks.Sixpatientsunderwenttreatmentconsistingofacombination ofarthroscopicirrigationanddebridement,andonepatientwastreatedbymeansofopen arthrotomy.Allthepatientsreceivedsystemicantibiotictherapyinaccordancewiththeir bacterialsensitivity.
Results:Allsevenpatientsachievedsatisfactoryresults,takingintoconsiderationespecially theimprovementofpainandthepatients’satisfaction.Thefunctionalassessmentwas performedusingtheUniversityofCaliforniaLosAngeles(UCLA)scale.Onlyonepatient neededtogothroughanotherarthroscopicprocedure.Staphylococcusaureuswasisolated fromfourculturesandEscherichiacolifromoneculture.Thereweretwosituationsinwhich thepatientsusedempiricalantibiotictherapyandtheculturesshowednegativeresults. Amongtheassociatedprocedures,tenotomyofthebicepswasperformedinfourcases, resectionofthelateralthirdoftheclavicleduetoosteomyelitisinonecaseandarthrotomy ofthekneeinonecase.
Conclusion:Surgical treatment was effective in the cases of arthritis associated with arthropathyoftherotatorcuff.Inpatientswitharthropathyoftherotatorcuffand subclin-icallyalteredlaboratorysigns,thepossibilityofpyoarthritisshouldalwaysbesuspected.
©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheUniversidadeFederaldeSãoPaulo,EscolaPaulistadeMedicina,DepartamentodeOrtopediaeTraumatologia, CentrodeTraumatologiadoEsporte,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](D.Sobreira).
http://dx.doi.org/10.1016/j.rboe.2015.09.016
Artrite
séptica
e
artropatia
do
manguito
rotador:
lembrar-se
dessa
associac¸ão
Palavras-chave: Artropatias Manguitorotador Artriteinfecciosa Artroscopia
r
e
s
u
m
o
Objetivo:Descreveraocorrênciadeartritesépticaglenoumeralempacientescomartropatia domanguitorotador,bemcomodestacaraimportânciadocorretodiagnósticoe procedi-mentocirúrgico.
Metologia: Foramfeitas oitodrenagens cirúrgicasem sete pacientescom pioartritegle-noumeral.Todosospacientesapresentavamartropatiadomanguitorotador(quatrodosexo masculinoetrêsdofeminino).Seispacientesapresentavampioartritenoombrodominante, aidadevarioude53a93anos(médiade74anos).Adurac¸ãomediadossintomasantesda lavagemcirúrgicafoideseissemanas.Seispacientesforamsubmetidosaotratamentocom acombinac¸ãodeirrigac¸ãoartroscópicaedesbridamento,umpacientefoitratadopor artro-tomiaaberta.Todosospacientesreceberamantibioticoterapiasistêmicadeacordocoma sensibilidadebacteriana.
Resultados: Os sete pacientes obtiveram resultados satisfatórios, se levarmos em considerac¸ãoprincipalmenteamelhoriadadoreasatisfac¸ãodospacientes.Aavaliac¸ão funcionalfoifeitapormeiodaescaladaUniversidadedaCalifórniaemLosAngeles(UCLA). Apenasumpacienteprecisoupassarporumnovoprocedimentoartroscópico,em qua-tro culturasfoi isolado oStaphylococcus aureus,em uma cultura a Escherichiacoli eem duassituac¸ões,nasquaisospacientesusavamantibioticoterapiaempírica,essasculturas tiveramresultadonegativo.Entreosprocedimentosassociadosfez-sequatrotenotomiasdo bíceps,umaressecc¸ãodo1/3lateraldaclavículadevidoàosteomieliteeumaartrotomiado joelho.
Conclusão: Otratamentocirúrgicofoieficaznoscasosdeartriteassociadaaartropatiado manguitorotador.Sempresuspeitar,empacientescomartropatiadomanguitorotadorcom sinaissubclínicoselaboratoriaisalterados,dapossibilidadedeumapioartrite.
©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Degenerativearthropathyoftherotatorcuffisthe collapse oftheglenohumeraljointsecondarytochronicmassive rota-tor cuff injury. It causes elevation of the humeral head, jointdestruction,synovialfluidchanges,subchondralcysts, flatteningofthegreatertubercle,osteophytes, acetabulariza-tion of the coracoacromial arch, and osteopenia1,2 (Fig. 1).
It manifests as pain, crepitus, and decreased range of motion.3
Pyogenicarthritisofthe shoulderischaracterizedbyan inflammatoryprocessofinfectiousoriginaffectingthe gleno-humeraljoint.Hematogenicrouteisthemostcommoncause. However,othercausesincludecontiguity,previoussurgery,or intra-articularinjection.4,5
Septicarthritisoftheglenohumeraljointisrelativelyrare, representing10–15%ofalljoint infections,andcan leadto severeresiduallimitationwithpotentiallyfatalimplications.6
ThemostcommonlyfoundpathogenisStaphylococcusaureus, andtheirenzymesmaydestroytheauricularcartilagewithin 24–48h.7
Tothebestoftheauthors’knowledge,therearenostudies thatcorrelatebothconditions.Thisstudyaimedtodescribe the occurrenceofsepticglenohumeral arthritisinpatients with rotator cuff arthropathy, as well as to highlight the
importanceofcorrectdiagnosis ofinfection and early ade-quatetreatmenttopreventirreversiblechangestoboththe boneandsurroundingsofttissues.
Methodology
Between May 2009 and March 2014, seven patients with rotator cuff arthropathy developed septic arthritis of the glenohumeraljointandunderwentsurgicaltreatmentby sur-gicaldrainageandsystemicantibiotictherapytotheinfecting germ.Eightsurgicalprocedureswereperformed:fourpatients were male andthree were female,whose agerangedfrom 53 to 93 years (mean 74 years). Associated comorbidities were investigated, and patients were evaluated using the UCLAfunctionalscalethreemonthsaftertheprocedure.Six patients were subjectedtoarthroscopic procedure by com-biningarthroscopicirrigationanddebridementandonewas treatedwithopenarthrotomy.Themeanintervalfrom symp-tomonsettosurgicaldebridementwassixweeks(range:15–70 days).
Fig.1– X-raysinanteroposteriorandaxillaryincidenceofashoulderwithrotatorcuffarthropathy.
Fig.2–Leftimageshowsapunctureintheglenohumeraljoint.Rightimageshowstheaspiratedpurulentliquid.
Surgical
technique
Oftheeightjointsurgeries,sevenwereconducted arthroscopi-cally.Arthroscopicdebridementoftheglenohumeraljointwas performedwithpatientundergeneralanesthesiaoverbeach chairpositioning.Anarthroscopewith30◦ angular
inclina-tionwasintroducedthroughtheposteriorportalandaninitial inspectionofthejointwasmade.Then,asecond anterosu-periorportalwascreatedintherotatorintervalandthejoint wasirrigatedwith10Lofsalinesolution.Throughtheanterior portal,amotorizedshaverbladewasintroducedfor debride-mentoftheinflamedsynoviumandofthearticularfibrotic tissue.Athirdlateralportalwascreatedfordebridementof thesubacromialspace.
Anopenarthrotomywasperformedwiththepatientunder generalanesthesia over beachchair positioning,using the deltopectoral approach and dissectionby layersuntil joint exploration;devitalizedtissuewasremovedandthejointwas irrigatedwith10Lofsalinesolution.
Results
Allsevenpatientsinthestudyhadcomorbidities:fivehadtype 2diabetesmellitus,onehad chronicliverdisease,fourhad
Table1–Comorbiditiesvs.numberofcases.
Comorbidities Numberofcases
Arterialhypertension Four
Diabetesmellitus Five
Smoking Two
Alcoholism One
Liverdisease One
Infectionatanothersite(pyogenic arthritisoftheknee)
One
HIV One
Osteomyelitisinlateralthirdofthe clavicle
One
arterialhypertension,onehadahistoryofpyogenicarthritis oftheknee,onewasachronicalcoholic,twoweresmokers, onehadosteomyelitisatthelateralthirdoftheclavicle,and onewasHIV-positive(Table1).
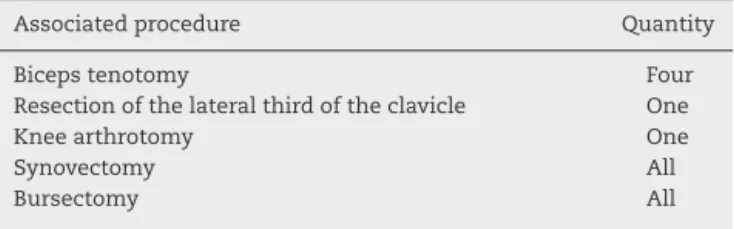
Thefollowingassociatedprocedureswereperformed intra-operatively: four biceps tenotomies, one resection of the lateralthirdoftheclavicleinthepatientwithosteomyelitis, andonekneearthrotomyinthepatientwhohadconcomitant pyogenicarthritisoftheknee;synovectomyandbursectomy wereperformedinallcases(Table2).
Table2–Associatedproceduresvs.quantity.
Associatedprocedure Quantity
Bicepstenotomy Four
Resectionofthelateralthirdoftheclavicle One
Kneearthrotomy One
Synovectomy All
Bursectomy All
infourpatients,andEscherichiacoliwasobservedinonecase. Thetwopatientswhopresentednegativecultureswereusing oralantibiotics.
Insixcases,theinfection waseradicatedwithonlyone surgicalprocedure.Inonepatient,asecondarthroscopywas necessaryduetoinfectionrecurrence.
Meanfollow-upwas12.2months(6–24).MeanUCLAscore attimeoflastfollow-upwas22points(15–29).Onlyonepatient wasnotsatisfiedwiththeresult.
Discussion
Theterm“Milwaukeeshouldersyndrome”wasfirstusedin 1981todescribefourelderlywomeninMilwaukee,inthestate ofWisconsin,UnitedStates,who presentedwith recurrent bilateralshouldereffusions,radiographicevidenceofsevere destructivealterationsintheglenohumeraljoint,andmassive rotatorcuffinjuries.8,9
Patientswithrotatorcuffarthropathyhavesignificantpain, functionallimitation,and strength reduction.4 Whenthese
patientsdevelopglenohumeralsepticarthritissuperimposed byarotatorcuffinjury,thepre-existingsymptomsmaymask theinfection.
Theauthors ofthe present study believe that infection shouldbesuspectedinanypatientwithaprogressivepainful conditionthatprimarilyaffectstheshoulderinthepresence ofelevatedinflammatorymarkers(WBC,CRP,andESR). His-toryofpreviousshoulderprocedure,whetheraninfiltrationor previoussurgery,withsubsequentprogressionofsymptoms, shouldonlyincreasesuspicion.
Earlydiagnosisandtreatmentofpyogenicarthritisofthe glenohumeraljointisessentialtopreventirreversiblechanges totheboneorsurroundingsofttissues,therebyavoiding com-promisingtheresultsofothersurgicalproceduresthatmay benecessary.10–12 Jeon et al.,10 intheir retrospective study,
demonstratedthe safety andefficacy ofarthroscopic treat-mentin19patientsdiagnosedwithpyogenicarthritisofthe glenohumeraljoint.Patientswhounderwentsurgerywithin twoweeksofarthroscopiclavagehadbetteroutcomesthan thosewhohad symptomsforalongertime.Thoseauthors also observed a high proportion ofmedical comorbidities, suchasdiabetes,previousinfiltrationsintheshoulder,and pre-existingrotatorcuffinjuriesintheirsample.However,in thatstudy,theauthorsdidnotmentionadirectassociation betweenthemassiverotatorcuffinjuryandpyogenicarthritis. Arthroscopicaltreatmentofsepticarthritisoftheshoulder withlavageanddebridementhasbeenreportedinselected casesaftertheearlydiagnosticofinfection.11,12 Inturn,an
opensurgicalapproachismorecommonlyperformedincases oflatediagnosisorlatestagesofinfection.13
Duncanetal.advocatetheearlydetectionandproper treat-mentofpyogenicarthritisoftheglenohumeraljointinorder topreventirreversiblechangestotheboneandsurrounding softtissues.11
Abdel et al.14 observed that most patients with
sep-tic arthritisare elderly, immunocompromised, and present increased inflammatory markers. Patients and surgeons shouldbeawarethatoneinthreepatientsrequiresadditional surgeryafterprimaryarthroscopy.
Inthisliteraturereview,nootherstudiescorrelatingrotator cuffarthropathywithpyogenicarthritisoftheglenohumeral jointwereretrieved.
As strengthsofthe present study,the sampleindicated anassociationthathadnotbeendescribedintheliterature, andshowstheimportanceofearlydiagnosisandtreatmentof pyogenicarthritisoftheglenohumeraljointsinpatientswith rotatorcuffarthropathy.
Asweaknesses,thesmallsamplesizeandtheshort follow-uptimeinsomepatientsarenoteworthy.Also,astheUCLA questionnairewasnotappliedpreoperatively,comparisonof clinicaloutcomespreandpost-treatmentwasnotpossible.
Conclusion
Pyogenicarthritisoftheglenohumeraljointshould be sus-pected inpatients withrotator cuffarthropathyassociated withsubclinicaland/orlaboratoryalterations.Surgical treat-mentshouldbeconductedasearlyaspossible,whetheropen orarthroscopically.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.HamadaK,FukudaH,MikasaM,KobayashiY.
Roentgenographicfindingsinmassiverotatorcufftears.A long-termobservation.ClinOrthopRelatRes.1990;(254):92–6.
2.NeerCS,CraigEV,FukudaH.Cuff-teararthropathy.JBone JointSurgAm.1983;65(9):1232–44.
3.PollockRG,DelizED,McIlveenSJ,FlatowEL,BiglianiLU. Prostheticreplacementinrotatorcuff-deficientshoulders.J ShoulderElbowSurg.1992;1(4):173–86.
4.JeroshJ.Acutejointinfection:diagnosisandtreatment. Orthopade.2004;338(11):1309–18.
5.LeslieBM,HarriesJM3rd,DriscollD.Septicarthritisofthe shoulderinadults.JBoneJointSurg.1989;71(10):1516–22.
6.KellyPJ,CoventryMB,MartinWJ.Bacterialarthritisofthe shoulder.MayoClinProc.1965;40:695–9.
7.BrowerAC.Septicarthritis.RadiolClinNAm. 1996;34(2):293–309.
8.GarancisJC,CheungHS,HalversonPB,McCartyDJ. “Milwaukeeshoulder”–associationofmicrospheroids containinghydroxyapatitecrystals,activecollagenase,and neutralproteasewithrotatorcuffdefects.III.Morphologic andbiochemicalstudiesofanexcisedsynoviumshowing chondromatosis.ArthritisRheum.1981;24(3):484–91.
proteasewithrotatorcuffdefects.I:Clinicalaspects.Arthritis Rheum.1981;24(3):464–73.
10.JeonIH,ChoiCH,SeoJS,SeoKJ,KoSH,ParkJY.Arthroscopic managementofsepticarthritisoftheshoulderjoint.JBone JointSurgAm.2006;88(8):1802–6.
11.DuncanSFM,SperlingJW.Treatmentofprimaryisolated shouldersepsisintheadultpatient.ClinOrthopRelatRes. 2008;466:1392–6.
12.KirchhoffC,BraunsteinV,BuhmannS,OedekovenT, MutschlerW,BiberthalerP.Stage-dependantmanagementof
septicarthritisofshoulderinadults.IntOrthop. 2009;33(4):1015–24.
13.RuhmannO,SchmolkeS,BohnsackM,FlammeC,WirthCJ. Shoulderarthrodesis:indications,technique,results,and complications.JShoulderElbowSurg.2005;14(1): 38–50.